

Key Takeaways:
-
EHR integration for 50-plus hospital networks starts at $250,000 to $750,000 for first-phase platforms.
-
Discovery, HL7 v2 feeds, FHIR R4 APIs, data normalization, EMPI logic, and HIPAA controls are included.
-
Audit trails, monitoring, UAT, and rollout support are essential components of enterprise integration development.
-
The first phase covers priority workflows but not every hospital, specialty, and downstream system connection.
-
How Intellivon builds this: a reusable interoperability foundation preparing large health systems for AI-ready clinical workflows.
A 50-hospital EHR integration platform build costs between $250,000 and $780,000, with the range driven by EHR vendor count, FHIR R4 implementation depth, and legacy data volume. EHR integration development cost is a phased investment, and capital requests that flatten it into one number are how projects lose their budgets before go-live.
That range is largely set by one architectural decision made before development starts. Without a vendor-neutral integration engine separating EHR-specific APIs from the core data layer, the build becomes point-to-point connections that need rebuilding every time a vendor updates its API, turning a $350,000 project into a $600,000 one. Health systems with mature integration engine environments report 40–60% lower per-interface build costs than point-to-point approaches.
Intellivon has spent over ten years building enterprise EHR integration platforms at this scale, applying a FHIR-first, compliance-led architecture that makes cost modeling predictable. This blog breaks the EHR integration development cost down phase by phase, from integration engine architecture to data normalization, compliance, and maintenance, so you have real numbers before committing.

How Much Does EHR Integration Development Cost?
The initial EHR integration development cost usually starts at $250,000 to $750,000 for a first-phase enterprise platform built for a 50+ hospital network. This capital range covers the engineering of a centralized, reusable interoperability layer rather than executing a concurrent installation across dozens of distinct physical facilities.
By establishing this foundational data clearinghouse first, an integrated delivery network provides its systems with a scalable core for priority data feeds, data normalization, and compliant patient matching.
Phase-by-Phase Capital Allocation Breakdown
| Cost Area | What It Covers | Estimated Range |
| Discovery & Integration Audit | EHR inventory, system map, workflow review, vendor access review | $20,000–$55,000 |
| Architecture & Delivery Roadmap | Integration design, FHIR strategy, rollout plan, security model | $30,000–$75,000 |
| HL7 v2 & CDA Integration Layer | ADT, labs, orders, results, document exchange, message routing | $60,000–$160,000 |
| FHIR API Implementation | FHIR R4 resources, authentication, API access, SMART on FHIR basics | $55,000–$150,000 |
| Data Normalization & Mapping | LOINC, SNOMED CT, RxNorm, ICD-10, local code cleanup | $40,000–$125,000 |
| Light EMPI & Patient Matching | Duplicate detection, match rules, confidence scoring, review queues | $35,000–$100,000 |
| HIPAA & Security Controls | RBAC, encryption, audit trails, access logs, PHI safeguards | $35,000–$110,000 |
| UAT & First Rollout Support | Multi-site testing, go-live support, issue triage, stabilization | $30,000–$85,000 |
| Monitoring Dashboard | Failed messages, latency, feed health, data-quality alerts | $25,000–$70,000 |
| Total First-Phase Estimate: | Reusable Centralized Interoperability Core Layer | $250,000–$750,000 |
1. First-Phase Platform Cost Breakdown
An enterprise EHR integration development cost sits between $250,000 and $750,000 when limited to a core architectural framework.
This phase deploys a centralized, multi-tenant integration engine that handles foundational data streams from selected pilot facilities rather than a 50-hospital big bang rollout.
- Core Focus: Establishes the centralized hybrid cloud integration layer, security infrastructure, and core database models.
- Data Scope: Focuses on high-priority clinical feeds like Admission, Discharge, and Transfer (ADT) messages and basic lab results.
- Infrastructure Strategy: Allows the health system to validate data flows in a controlled sandbox before committing heavy capital to full-scale facility rollouts.
This initial architectural setup directly dictates the trajectory and financial predictability of your later facility rollout cost.
2. Later Facility Rollout Cost Factors
Deploying the established platform across the remaining facilities in a 50-hospital network introduces incremental, repetitive costs driven by local infrastructure variations.
Each additional facility requires custom configuration, validation testing, and local connection mapping to tie into the central hub.
- Per-Hospital Variable Cost: Averages $15,000 to $45,000 per facility depending on the state of the local EHR instance.
- On-Site Validation: Covers local user acceptance testing (UAT), network engineering, and local firewall configurations.
- Rollout Strategy: Executing rollouts in phased waves of 5 to 10 hospitals stabilizes cash flow and lets team members apply optimization lessons from earlier waves.
Once the physical connections are planned, health systems must account for unavoidable EHR vendor and API licensing cost structures.
3. Vendor and API Licensing Cost Realities
EHR vendor and API licensing cost components are separate from development fees and are paid directly to software vendors like Epic, Oracle Health, or Meditech.
These proprietary ecosystems enforce strict commercial models for accessing production environments or using specific web services.
- Epic App Market and Care Everywhere: Requires annual developer fees or transaction-based volume pricing for data exchange.
- Oracle Health (Cerner) Ignite APIs: Utilizes multi-tiered licensing models based on patient connection counts or API call volumes.
- Third-Party Middlewares: Platforms like Mirth Connect premium tiers or Rhapsody add predictable annual line-item licensing expenses.
These vendor fees directly feed into the broader calculation of your ongoing maintenance cost and system health monitoring.
4. Ongoing Maintenance and Data Pipeline Monitoring
Ongoing maintenance cost structures typically require 18% to 25% of the initial platform build capital on an annual basis.
For an enterprise platform with a first-phase cost of $250,000 to $750,000, this equates to roughly $45,000 to $187,500 per year.
- Schema Drift Adaptation: Upkeep covers updating data pipelines when an EHR vendor changes its internal database schemas or API payloads.
- Compliance and Security Auditing: Includes continuous vulnerability patching, encryption certificate rotation, and mandatory log reviews.
- Throughput Optimization: Ensures real-time data integration cost balances stay flat by managing database indexing and cloud storage tiers.
To properly allocate these funds, enterprise leads must understand the breakdown of internal staffing and governance cost factors.
5. Internal Staffing and Governance Cost Demands
Building the platform requires a dedicated internal governance structure to manage clinical data ownership, cross-facility coordination, and clinical safety. Technical development cannot succeed without explicit administrative alignment regarding how data is normalized and shared.
- Clinical Data Committees: Require protected hours from Chief Medical Information Officers (CMIOs) and clinical directors to approve terminology mappings.
- Project Management Overhead: Demands experienced enterprise program managers to coordinate across 50 separate hospital IT departments.
- Legal Compliance Alignment: Involves ongoing legal review for Business Associate Agreements (BAAs) and multi-facility data sharing agreements.
This collaborative approach ensures your internal teams possess the exact knowledge required to maintain long-term platform stability.
The honest answer is not that $750,000 connects all 50 hospitals instantly on day one. Rather, a budget of $250,000 to $750,000 builds the foundational, high-throughput interoperability layer that makes every subsequent hospital connection significantly cheaper, faster, and safer to deploy.
What Does the $250K–$750K First Phase Actually Include?
A $250,000 to $750,000 first-phase EHR integration build delivers the core infrastructure needed to prove stable data exchange across a defined cluster of pilot facilities. This allocation builds a centralized, multi-tenant interoperability layer, configures high-priority HL7 and FHIR pipelines, installs automated data normalization engines, and deploys system monitoring tools.
It establishes a highly reusable architectural core that validates clinical workflows before capital is deployed on a massive, facility-wide rollout.
1. Phase 1 Core Deliverables Matrix
| System Component | Technical Execution Profile | Production Scope Boundary |
| Priority EHR Connections | Ingestion endpoints configured for primary target platforms via web services and native interface engines. | Limited to 2–3 vendor instances (e.g., Epic + Oracle Health) at initial pilot sites. |
| Priority Clinical Feeds | Real-time message streaming, parsing, and structured database routing for essential care data. | Constrained to core operational objects: ADT, labs, vitals, medications, and clinical notes. |
| Integration Engine Layer | Central processing core configured with explicit routing, retry policies, and message failure loops. | Deploys a unified, highly available containerized cluster running on cloud infrastructure. |
| Managed FHIR API Gateway | Read-only and limited write RESTful endpoints mapped to standardized clinical data stores. | Implements targeted US Core IG resources: Patient, Observation, and Encounter profiles. |
| Data Normalization Core | Real-time translation pipelines converting localized strings into standardized terminology maps. | Focused on validating the highest-volume clinical concepts across incoming data feeds. |
2. Priority EHR Connections
Phase one connects the network’s high-volume clinical systems to validate data exchange pathways across distinct vendor environments. This approach caps your initial multi-EHR vendor integration spend by focusing engineering on primary pilot facilities rather than a simultaneous 50-hospital installation.
- Epic Installations: Connections are established with local instances to manage initial Epic integration cost variables through targeted Epic FHIR API implementation pipelines.
- Oracle Cerner Environments: Technical endpoints link to the core database infrastructure to handle Cerner integration cost buckets via the Cerner Millennium API.
- Ambulatory Touchpoints: Engineers build interface adapters for community nodes, covering Meditech integration cost, athenahealth API integration, Allscripts integration cost, and eClinicalWorks integration frameworks.
Decoupling individual connection profiles into an abstract adapter layer isolates local system variances. This technical isolation prevents custom local scripts from fragmenting the central database architecture.
3. Priority Clinical Data Feeds
The initial development phase limits ingestion to high-value, foundational data types rather than attempting historical migrations of all legacy records. This restriction keeps transactional message queues responsive and helps contain data quality management cost factors.
- Workflow Operations: Real-time Admission, Discharge, and Transfer (ADT) messages provide immediate synchronization for patient demographics, active encounters, and discharge summaries.
- Clinical Elements: Processing pipelines capture laboratory results, diagnostic orders and results, medication profiles, documented allergies, and active problem lists.
- Documentation and Notes: Structured document ingestion parses inbound clinical notes and transition summaries to extract narrative care insights.
Isolating these specific fields ensures consistent system performance across the network during high-volume periods.
4. First Integration Engine Setup
An engine core serves as the central spine of the integration engine architecture, programmatically routing, transforming, and retrying incoming messages. Without a centralized broker, every hospital endpoint requires a standalone, fragile connection mesh.
- Message Broker Optimization: The platform deploys enterprise brokers to handle high-throughput HL7 v2 message integration streams.
- Document Processing: Ingestion maps parse complex clinical documents to enable standardized HL7 CDA document exchange.
- Pipeline Observation: Engineers configure continuous tracking tools to address integration monitoring and alerting cost lines.
- Commercial Platforms: Deployed cloud packages like Rhapsody as a Service establish fixed software licensing starting at $50,000 annually for entry-tier setups, matching commercial Mirth Connect implementation cost expectations.
This architectural layer converts varying local payloads into predictable transactional streams.
5. First FHIR API Layer
The initial Fast Healthcare Interoperability Resources (FHIR) framework provides downstream applications with uniform, RESTful access to clinical data objects. This phase deploys specific, high-utilization core profiles to keep implementation schedules predictable.
- API Management Gateway: A secure access point deploys to handle centralized FHIR R4 API integration requests.
- Workflow App Launching: Native frameworks integrate OAuth 2.0 validation via SMART on FHIR integration rules to run external clinical apps directly inside user frames.
- Real-Time Alerts: Contextual events hook into standard care pathways through targeted CDS Hooks integration triggers.
- Compliance Infrastructure: Bulk extraction pipelines deploy via the FHIR bulk data API to lower your regulatory patient access API compliance cost liabilities.
This secure gateway provides external applications with a compliant data-access layer.
6. First Data Normalization Layer
Raw data feeds are rarely uniform upon arrival and require a centralized semantic transformation pipeline to translate local facility vocabularies. This parsing layer ensures diverse incoming clinical messages conform to a single, standardized corporate dictionary.
- Clinical Taxonomy Mapping: Automated transformation rules evaluate incoming clinical codes, directing real-time SNOMED CT mapping pipelines for deep diagnostic records.
- Diagnostic Lab Labs: Inbound raw lab strings run through automated LOINC code mapping layers to match variable test formats to international markers.
- Therapeutic Terminology Normalization: Incoming medication strings convert via automated RxNorm mapping blocks to align varying drug descriptions.
- Administrative Code Sorting: Historical and active billing items route through ICD-10 code normalization tracks to enforce data uniformity.
This structural cleanup guarantees clear, reliable data across downstream systems.
This precise baseline inventory makes the immediate capabilities of your phase-one capitalization fully transparent. The subsequent phase focuses on defining the explicit architectural boundaries by outlining what is intentionally excluded from this initial deployment budget.
What Is Not Included in the First-Phase Cost?
The $250,000 to $750,000 range does not include every hospital, every specialty workflow, every legacy system, every downstream analytics use case, and every future acquisition. It covers the first controlled platform build.
However, the full enterprise rollout requires later waves, separate facility onboarding budgets, and ongoing support planning.
1. Phase 1 Explicit Exclusions Framework
| Out-of-Scope Item | Technical Boundary Deviation | Alternative Capital Allocation Stream |
| Complete Network Rollout | Concurrent deployment to all 50 physical production environments is explicitly excluded. | Funded iteratively via localized facility activation waves ($15K–$45K per site). |
| Bidirectional Database Write-Backs | Advanced clinical orchestration engines that directly alter core EHR records are out of scope. | Managed as specialized clinical application development additions in Phase 2. |
| Enterprise Master Patient Index (EMPI) | Full-scale algorithmic deterministic and probabilistic record matching for millions of lives. | Built initially as a lightweight, rule-based matching queue before full scaling. |
| Comprehensive HITRUST Certification | Formal corporate certification audits against the consolidated CSF security framework. | Handled via independent institutional compliance budgets ($70K–$250K framework fees). |
2. Multi-Facility and Cross-Vendor Scaling
Consequently, the initial capital allocation explicitly avoids simultaneous integration across all 50 hospitals or onboarding every minor niche vendor software tool across the enterprise. Trying to force parallel installations during the platform phase splits your technical engineering team, creating severe configuration drift across local endpoints.
For this reason, production endpoints remain strictly restricted to selected reference sites to ensure early pipeline stability.
- Geographic and Instance Limits: The scope isolates initial infrastructure to 2 or 3 distinct vendor instances rather than configuring localized data adapters for all 50 network destinations concurrently.
- Minor Vendor Omissions: Specialty applications and niche software packages used in independent departments are left offline until core messaging streams normalize.
- Acquisition Isolation: Furthermore, any hospital systems acquired mid-project require separate, dedicated post-acquisition integration work rather than drawing from the initial budget.
As a result, this physical boundary ensures that developers can exhaustively test transport stability without managing a mountain of unique local facility firewall policies. Therefore, once the core architectural layer handles data uniformly at the pilot sites, onboarding subsequent facilities becomes a repetitive, lower-risk engineering step.
3. Advanced Data Orchestration and Lakes
Meanwhile, phase one establishes standard message ingestion pipelines but does not build long-term cold storage data architecture or complex algorithmic write-back engines. This boundary prevents early development from stalling out under heavy data architecture design cycles.
- Write-Back Exclusion: Data streams operate on read-only or transactional notification architectures; however, avoiding deep, risky bidirectional write-back workflows into production EHR databases.
- Storage Framework Bounds: Structural elements exclude a full clinical data repository or an un-nested, analytic-ready FHIR data lake architecture.
- AI Readiness: While the incoming pipelines normalize data, advanced AI model deployment, clinical vector index calculations, and automated agent processing loops are entirely out of scope.
In contrast, maintaining a sharp focus on transport-only logic avoids exposing the initial platform build to heavy data storage governance reviews. Consequently, this approach ensures your technical teams deliver clean, active pipelines that can easily feed into downstream repositories during later capital cycles.
4. Specialized Departmental Interfaces
In addition, high-complexity ancillary departmental software frameworks are completely omitted from the initial integration pass to preserve development velocity. These specialized modules run on unique data variants that require extensive local workflow modeling.
- Financial Networks: Core pipelines ignore revenue cycle integration requirements, keeping billing schemas separate from early clinical transport layers.
- Ancillary Systems: Specifically, the interface boundaries exclude custom standalone pharmacy systems, complex imaging archives (PACS), and direct point-of-care medical device interfaces.
- Specialty Workflows: Oncology protocols, transplant registries, and high-intensity behavioral health fields are left out of early data normalization sprint schedules.
Ultimately, omitting these isolated data streams keeps the platform focused on high-volume clinical data sets like ADT and laboratory feeds. Because of this, it prevents specialized department requirements from complicating your core integration engine maps.
5. Comprehensive Institutional Security Certifications
Finally, the foundational platform code implements strict security controls but does not cover the final organizational certification fees required for advanced security frameworks. Formal institutional auditing is treated as a separate, distinct administrative capital line item.
- HITRUST Certification Boundaries: The core budget excludes the heavy costs associated with achieving a formal HITRUST certification profile. According to 2026 audit metrics, an enterprise assessment can demand $75,000 to $250,000 in independent assessor fees alone.
- Penetration Testing Scope: Development fees include standard code reviews, but exclude comprehensive third-party penetration testing and continuous red-team exercises.
- Long-Term Internal Staffing: Capital allocations fund specialized outsourced delivery engineers, leaving long-term internal IT hiring and corporate business associate agreement (BAA) management to operations.
Thus, this clear separation keeps your development dollars focused entirely on software delivery rather than administrative compliance processing. As an outcome, the platform ships compliance-ready, allowing internal information security teams to pursue formal audits on an independent timeline.
What Drives EHR Integration Cost Up or Down?
EHR integration cost moves toward the lower end when the project has fewer vendors, cleaner data, standard workflows, limited bidirectional exchange, and strong internal ownership.
It moves toward the upper end when the network has several EHR vendors, messy local codes, custom workflows, high data volume, strict uptime needs, and deeper compliance requirements.
1. Capital Variance Matrix
| Cost Driver | Lower-Cost Scenario | Higher-Cost Scenario |
| EHR Vendor Mix | One or two vendors | Epic, Oracle Health, Meditech, athenahealth, Allscripts, and legacy systems |
| Data Exchange Type | Read-only access | Bidirectional clinical workflows |
| Standards | Limited FHIR resources | HL7 v2, CDA, FHIR, Bulk FHIR, SMART, CDS Hooks |
| Data Quality | Clean fields and codes | Local codes, duplicates, missing values, inconsistent workflows |
| Patient Identity | Basic matching | Enterprise EMPI with review workflows |
| Security Scope | Standard HIPAA controls | Zero-trust, SOC 2 evidence, penetration testing, HITRUST planning |
| Rollout | Few priority sites | Multiple facility types and acquired hospitals |
| Monitoring | Basic alerts | Real-time dashboard, SLA tracking, anomaly detection |
| Vendor Access | Clear API access | Custom approvals, licensing, marketplace review, interface fees |
2. Vendor Complexity
Deploying pipelines across a single vendor environment accelerates engineering timelines.
Conversely, a diverse multi-vendor footprint introduces distinct data-handling schemas that amplify your infrastructure expenditures.
- Custom Interface Mapping: Separate connection frameworks must be engineered for each vendor, as Epic does not communicate natively with Meditech databases.
- Workflow Inconsistencies: Even identical EHR platforms require custom endpoint tuning if independent hospitals configure local fields and templates differently.
- API Tollgates: Multi-vendor networks multiply vendor marketplace review times and proprietary endpoint access licensing fees.
Therefore, harmonizing a mixed network requires independent data transformation logic for each separate software provider, shifting the capital requirement to the higher end.
3. Data Quality
Clean, well-structured inbound data elements allow automated validation rules to process transactional messages instantly.
In contrast, incoming data plagued by structural inconsistencies requires intensive parsing, algorithmic remediation, and custom filtering scripts.
- Code Multiplicity: Local clinical descriptions require manual translation when hospitals use non-standard naming conventions for lab results or medications.
- Record Duplication: Unmanaged databases often contain missing values and duplicate identities, which requires deploying complex patient-matching logic.
- Pipeline Friction: Clean fields require simple pass-through logic, whereas messy data structures double your validation and parsing code footprint.
According to research from AHIMA, data inaccuracies and duplicates can inflate data quality management cost lines by thousands of dollars per facility. As a result, resolving messy local codes substantially drives up your engineering validation lifecycle.
4. Integration Depth
Read-only pipelines that fetch patient data structures require minimal backend choreography and run on simpler authorization protocols.
However, implementing bidirectional clinical workflows introduces intense state-management dependencies and extensive database-locking logic.
- State-Management Load: Simple fetch APIs run independently, but write-back pipelines must confirm database updates without corrupting active EHR files.
- Workflow Complexity: Advanced automation, such as clinical decision support and prior authorization triggers, requires deeper transaction handling.
- Testing Cycles: Bidirectional access demands prolonged user acceptance testing (UAT) and governance sign-offs to protect patient safety.
For this reason, deeper data write access demands rigorous verification layers to protect target systems. Consequently, shifting from passive viewing to active write-backs dramatically raises development hours.
5. Reliability Requirements
Standard visualization applications can typically tolerate minor transactional processing latencies without disrupting overall administrative operations.
Meanwhile, active clinical decision engines require strict real-time, event-driven message architectures to safely guide care delivery.
- Redundancy Infrastructure: High availability designs require mirror servers and automated cloud load-balancers to avoid single points of failure.
- Failover Execution: Disaster recovery environments demand near-zero data loss parameters, which requires continuous data replication pipelines.
- Queue Monitoring: Maintaining low latency under heavy volume requires complex monitoring scripts and immediate alert systems.
Consequently, engineering a highly fault-tolerant network framework raises your base infrastructure and active monitoring cost line items. Thus, strict service level agreements push budgets toward the higher tier.
Cost variation follows vendor complexity, data quality, workflow depth, compliance pressure, and reliability requirements. That is why discovery must come before any serious estimate.
Real-World EHR Cost Examples From Health Systems
Real-world EHR cost examples show why large health systems need careful integration planning. These examples are broader EHR implementation or EHR unification projects, not direct custom integration platform estimates.
Still, they show the scale of spending when health systems replace, consolidate, or modernize clinical technology across multiple facilities.
1. Enterprise Capital Expenditure Benchmarks
| Organization | Reported Cost | What the Project Involved | How to Use This Example |
| Northwell Health | $1.2B | Epic implementation to unify a large health system | Shows how expensive full EHR replacement can become |
| University of Vermont Health Network | $151.7M | Epic implementation across four hospitals over six years | Shows cost of replacing fragmented systems |
| Mass General Brigham | $1.2B | Large Epic launch after original estimate was lower | Shows how staffing, training, and rollout can expand cost |
| Kaiser Permanente | Multi-Billion | One of the largest Epic EHR projects publicly reported | Shows the scale of enterprise EHR standardization |
| Mayo Clinic | $1.5B | Enterprise EHR modernization benchmark | Shows why phased integration can be a lower-risk starting point |
2. Northwell Health ($1.2B)
Deploying a single, unified database across a sprawling healthcare ecosystem represents a massive capital commitment. Specifically, Northwell Health initiated a $1.2 billion capital program to consolidate more than 30 separate medical record platforms into a singular instance of Epic.
- System Consolidation: The multi-year infrastructure strategy aims to phase out mismatched software engines across 28 distinct hospital campuses.
- Application Scope: Beyond the core EHR layer, the modernization lifecycle replaces roughly 200 secondary clinical applications to ensure data continuity.
- Operational Readiness: Post-launch evaluations frequently require unplanned infrastructure and staffing investments to preserve patient safety margins.
3. University of Vermont Health Network ($151.7M)
Replacing disconnected software tools across smaller regional networks still demands substantial local capital outlays.
Meanwhile, the University of Vermont Health Network secured state approvals for a $151.7 million Epic installation spanning four regional hospitals.
- Fragmented Foundations: The deployment replaced an aging collection of custom interfaces that restricted cross-facility care coordination.
- Extended Timelines: Engineering, testing, and rolling out the unified platform required six years of phased development sprints.
- Regulatory Oversight: Multi-hospital standardizations remain subject to intense public utility reviews and strict budget cap compliance mandates.
As a result, even mid-sized regional networks face major capital constraints when replacing legacy systems root-and-branch. For this reason, decision-makers must carefully weigh immediate replacement budgets against targeted middleware optimization paths.
4. Mass General Brigham ($1.2B)
Initial enterprise software estimates can expand dramatically during active rollout phases due to unforeseen workflow dependencies.
In addition, Mass General Brigham (originally operating as Partners HealthCare) experienced a total capital climb reaching $1.2 billion for its enterprise Epic rollout.
- Scope Creep Dynamics: The baseline integration budget inflated as developers discovered hidden data quality issues across legacy databases.
- Training Overhead: Educating thousands of clinical staff members on new database workflows dramatically raised operational rollout costs.
- Stabilization Sprints: Maintaining data integration and alerting cost profiles required extended go-live engineering support teams.
Ultimately, software licensing accounts for only a fraction of a full system modernization program. Because of this, unexpected training demands and complex legacy data remediation frequently push capital needs beyond original projections.
5. Kaiser Permanente (Multi-Billion Benchmark)
Standardizing record structures for millions of active patient lives represents the upper limit of healthcare IT spending. Furthermore, Kaiser Permanente executed one of the largest enterprise EHR standardizations ever recorded by deploying a unified data layer nationwide.
- Massive Infrastructure Scale: The multi-billion-dollar framework connects hundreds of independent medical offices and dozens of dedicated hospitals.
- Data Lake Foundations: The architecture required building heavy, high-throughput data pipelines to aggregate real-time diagnostic inputs.
- Long-Term Lifecycle TCO: Maintaining a national software monolithic environment requires billions in recurring operational support allocations.
Thus, this extreme baseline highlights the sheer scale of centralized data management within massive integrated delivery networks. Consequently, organizations study these frameworks to map out large-scale data governance models.
6. Mayo Clinic ($1.5B Benchmark)
Modernizing clinical workspaces across world-class academic medical centers involves deep technical restructurings. In contrast, the Mayo Clinic consolidated its historic data networks under a single $1.5 billion system program named Project Plum.
- Data Normalization Scale: The engineering sprint mapped millions of complex patient histories into a standardized terminology library.
- Clinical Decision Velocity: The unified core integrates specialized analytics to supply care teams with real-time diagnostic insights.
- Resource Allocation: Capital allocations were heavily split between core software configurations and long-term internal IT governance staff.
As a outcome, total system replacement requires sacrificing massive amounts of operational focus and capital resources. Therefore, many health systems view these historic budgets as a clear sign to evaluate less disruptive software optimization strategies.
These examples should not be used to claim that custom EHR integration costs hundreds of millions. Instead, they show the alternative path. A $250,000 to $750,000 first-phase integration platform can be positioned as a controlled interoperability investment. It gives leadership a way to improve data flow before committing to massive system replacement or multi-year consolidation.
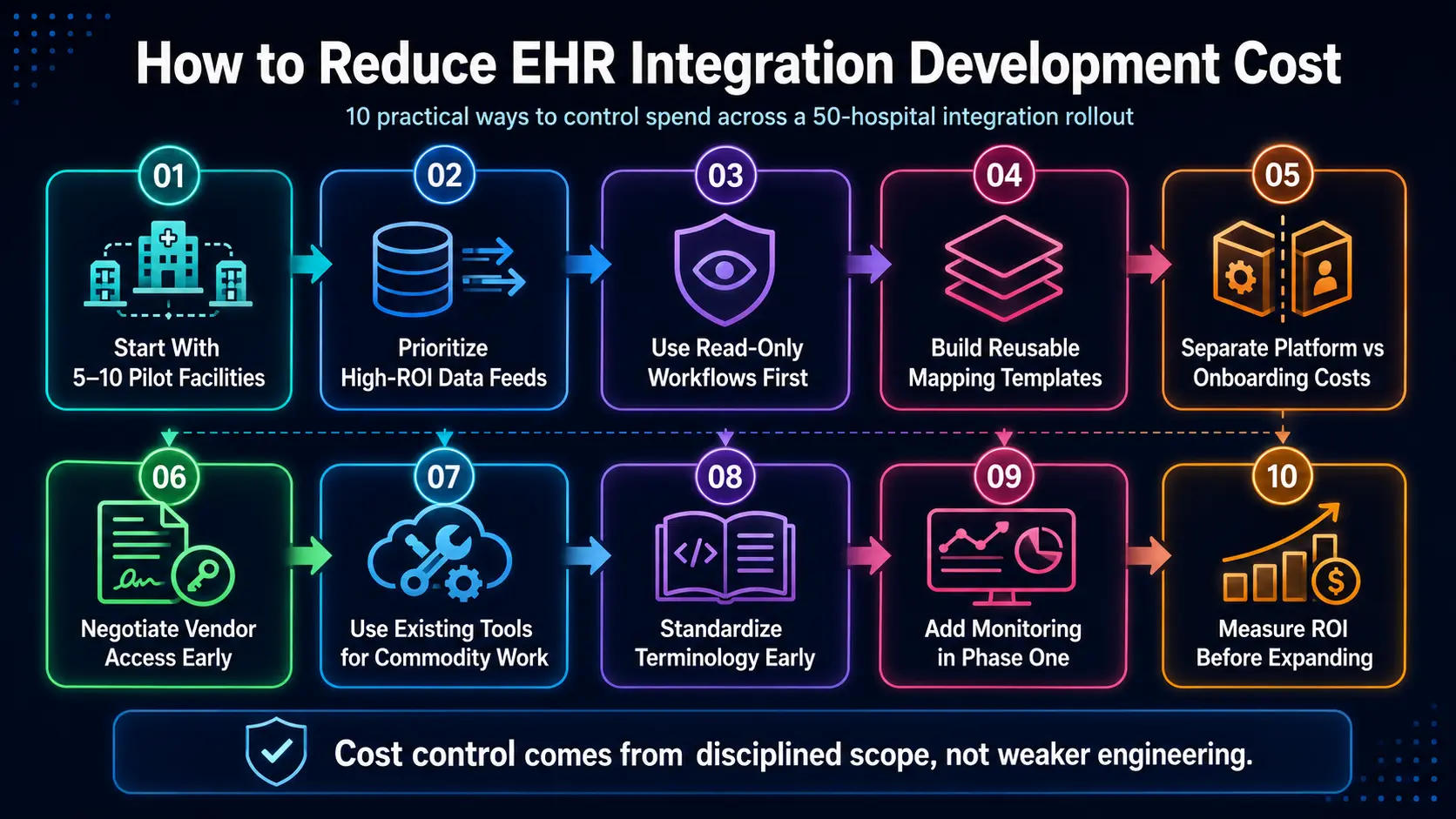
How to Reduce EHR Integration Development Cost
Health systems can reduce EHR integration development cost by narrowing the first phase, reusing interface patterns, prioritizing high-value data feeds, standardizing mappings early, limiting write-back workflows, negotiating vendor access upfront, using mature integration tools where useful, and measuring ROI before adding more facilities.
Cost control comes from disciplined scope, not weaker engineering.
1. Start With 5–10 Representative Facilities
Onboarding all 50 hospitals concurrently fragments your engineering focus and drives up early capital burn. Instead, launching the platform across a balanced cohort of 5 to 10 pilot facilities lets you safely evaluate your real-world vendor mix.
- Infrastructure Proofing: Developing within a smaller footprint allows engineers to stabilize transport layers before committing heavy capital.
- Mitigating Configuration Drift: Early site deployment exposes hidden local customization variances without corrupting the central database.
- Preventing Rework: Resolving architectural bugs within a restricted footprint protects future deployment waves from repeating costly design mistakes.
Consequently, this tactical footprint validates system performance while conserving capital resources. Therefore, initial phase scaling remains financially predictable because core code patterns are fully stabilized before wide deployment.
2. Prioritize High-ROI Data Feeds First
Attempting to ingest every obscure clinical data field at the start inflates testing windows and complicates your data schema maps. Meanwhile, prioritizing foundational, high-utilization feeds yields immediate operational utility for downstream applications.
- Transactional Anchors: Real-time Admission, Discharge, and Transfer (ADT) messages provide instant value for core patient tracking.
- Diagnostic Backbones: Laboratory results, active medication histories, documented allergies, and primary diagnoses offer the highest clinical insight per pipeline.
- Administrative Evidence: Discharge summaries, formal referral records, and core revenue cycle evidence satisfy immediate compliance and billing verification needs.
As a result, limiting early scope to these core elements prevents your message processing queues from becoming bottlenecked by low-value data. For this reason, specialty workflows should stay on the product roadmap until the primary business case is fully realized.
3. Use Read-Only Workflows Before Write-Back
Building bidirectional data exchange paths introduces intense database-locking dependencies and complex state-management requirements. However, leading with read-only data access layer delivery allows you to securely stream and view patient data profiles.
- Minimized Security Risk: Read-only architectures prevent external data payloads from accidentally corrupting source electronic health records.
- Streamlined Governance: Eliminating early write-backs shortens clinical safety review cycles and accelerates administrative sign-offs.
- Workflow Validation: Care teams gain complete visibility into aggregated records while engineering refines background messaging performance.
Consequently, this passive approach establishes a safe baseline before modifying source databases. Thus, delaying risky transactional writes until phase two preserves development velocity and lowers technical risk.
4. Build Reusable Mapping Templates
Engineering custom, point-to-point data mapping profiles for every individual facility endpoint quickly destroys project economics. In contrast, building abstracted, reusable transformation assets allows the platform to ingest data uniformly across common environments.
- Standardized Dictionaries: Creating baseline translation models maps localized clinical strings to international formats automatically.
- Reusable Data Objects: Universal data templates ingest provider IDs, demographic blocks, and common document types without unique code modifications.
- Repeatable Scaling: Onboarding costs drop sharply as developers apply pre-built templates to subsequent hospitals using similar EHR brands.
Therefore, investing in structural mapping frameworks during phase one protects the financial feasibility of the “Hospital 51” rollout. As a outcome, onboarding turns from an unpredictable engineering challenge into a repetitive configuration task.
5. Separate Core Platform Work From Facility Onboarding
Mixing core architectural engineering costs with local facility activation line items obscures your actual infrastructure return on investment. Specifically, partitioning the central core platform budget from site-specific setup fees brings total clarity to your capital allocations.
- Infrastructure Capitalization: Central middleware engineering, data lake construction, and core security frameworks are treated as a single asset investment.
- Variable Onboarding Line Items: Local firewall configurations, custom port modifications, and site-specific testing hours are billed as individual facility expenses.
- Predictable Financing: Finance teams can easily calculate the marginal cost to onboard a new hospital instance by reviewing isolated site fees.
Ultimately, this clear financial separation prevents localized configuration bottlenecks from distorting your primary platform budget. Because of this, executive leadership can accurately assess long-term infrastructure assets independent of local deployment waves.
6. Negotiate Vendor Access Before Development
Discovering hidden interface fees or restrictive API access rules mid-sprint can cause expensive development delays. In addition, finalizing explicit commercial data access terms with proprietary EHR vendors upfront ensures unblocked engineering timelines.
- Sandbox Procurement: Securing stable developer sandboxes before launch prevents highly paid engineers from sitting idle during active sprints.
- Clear Licensing Bounds: Reviewing marketplace terms ahead of time prevents unexpected transactional volume pricing from inflating your ongoing TCO.
- Data Rights Verification: Confirming institutional data ownership and third-party access parameters eliminates potential downstream legal blocks.
As a result, resolving vendor access dynamics early eliminates administrative roadblocks during software assembly. Therefore, your active engineering cycles stay focused entirely on pipeline production.
7. Use Existing Tools Where They Reduce Commodity Work
Building every message router and parsing utility from scratch unnecessarily inflates your development timeline. Conversely, using mature commercial integration engines and cloud healthcare utilities allows you to bypass commodity code production.
- Cloud Native APIs: Services like Google Cloud Healthcare API, AWS HealthLake, or Azure Health Data Services handle baseline storage and compliance routing.
- Proven Integration Core Layers: Incorporating established tools like Mirth Connect optimizes low-level HL7 message parsing straight out of the box.
- Targeted Engineering Focus: Internal development focus shifts entirely to building proprietary patient matching algorithms and unique care workflow logic.
Consequently, using proven infrastructure components reduces capital expenditure on baseline utility code. Thus, your custom development budget is spent entirely on high-value, proprietary workflows.
8. Standardize Terminology Early
Postponing data normalization until messy records reach downstream clinical analytics engines multiplies your technical debt. Instead, installing a semantic parsing layer directly at the ingestion boundary ensures all clinical data is cleansed upon arrival.
- Universal Diagnostics: Mapping local lab strings to international LOINC code standards creates a unified diagnostic repository.
- Unified Problem Lists: Translating custom local descriptors to SNOMED CT and ICD-10 sets ensures accurate cross-facility disease tracking.
- Therapeutic Alignment: Normalizing variable medication names through RxNorm references secures accurate drug interaction cross-checking.
Furthermore, early terminology cleanup optimizes your data quality management cost vectors across the network. As a result, downstream systems receive clean data, which prevents expensive retrospective database cleansing sprints.
9. Add Monitoring in Phase One
Omiting system observability tools to save early capital creates heavy operational support costs when silent data drops occur. In contrast, deploying a centralized monitoring and alerting framework during phase one ensures continuous data pipeline integrity.
- Immediate Error Trapping: Real-time dashboards flag, isolate, and log stalled or corrupted HL7 v2 messages instantly.
- Latency Trace Analysis: Infrastructure monitors track performance drops, allowing engineers to resolve database queues before workflows degrade.
- Operational Tracking: Dashboards display total transaction volumes and queue depths, giving IT teams full platform visibility.
Consequently, early monitoring deployments dramatically lower post-go-live support overhead. Therefore, system administrators can fix data anomalies proactively before clinicians experience workflow delays.
10. Measure ROI Before Expanding
Pushing into large-scale network deployment based solely on a successful technical test introduces severe capital risk. Meanwhile, pausing to verify hard financial and clinical metrics across your pilot cohort validates the expansion business case.
- Clinical Efficacy Tracking: Quantifying reductions in duplicate lab testing confirms the platform’s immediate care coordination value.
- Administrative Optimization: Measuring manual labor hours saved through automated data fetching validates workflow efficiency claims.
- Onboarding Cost Verification: Confirming that the per-facility onboarding fee falls within your $15,000 to $45,000 target justifies broader deployment financing.
Thus, gathering concrete pilot data secures reliable internal leverage for cap-ex expansion approvals. Consequently, you scale the platform across the remaining hospitals backed by verified operational savings.
Cost reduction does not mean cutting compliance, testing, or security. It means choosing the right first scope, reusing the right components, and delaying expensive workflows until the foundation is proven.
ROI of EHR Integration for Large Health Systems
EHR integration ROI comes from fewer duplicate tests, faster data access, lower manual chart retrieval, cleaner revenue cycle evidence, faster facility onboarding, better compliance readiness, and stronger AI-readiness.
Large health systems should measure ROI across clinical, financial, IT, compliance, and strategic value instead of looking only at interface cost.
1. Interoperability Capital Return Metrics
| ROI Area | What Improves | How to Measure It |
| Duplicate Testing | Fewer repeat labs and imaging orders | Avoided tests × average test cost |
| Care Coordination | Faster access to outside records | Staff hours saved × loaded labor cost |
| Revenue Cycle | Better documentation and claim evidence | Fewer delayed claims and avoidable denials |
| IT Productivity | Fewer repeated interface fixes | Ticket reduction × support cost |
| Acquisition Speed | Faster onboarding of new facilities | Weeks saved × operational value |
| Compliance Readiness | Better audit logs and access records | Audit preparation hours saved |
| AI-Readiness | Cleaner longitudinal data | Data cleanup avoided × engineering cost |
2. Reduced Duplicate Testing
Enforcing cross-facility data liquidity instantly curtails redundant clinical spending across connected hospital systems. Specifically, when a patient transitions between regional care facilities, clinicians can immediately view historical diagnostic profiles.
- Order Rationalization: Access to external records drives a measurable duplicate testing reduction integration metric.
- Asset Utilization: Eliminating unnecessary repeat imaging scans optimizes internal machinery throughput and shifts resource focus.
- Clinical Velocity: Eliminating diagnostic duplication enhances overall clinical workflow efficiency integration parameters.
3. Lower Manual Record Retrieval
Relying on manual workflows to aggregate external health histories fragments administrative focus and introduces significant care delays. Meanwhile, automating cross-platform document ingestion allows clinical documentation to populate user screens instantly.
- Friction Elimination: Medical records move securely across automated networks, completely bypassing traditional calling and faxing bottlenecks.
- Operational Reallocation: Case managers and care teams save thousands of annual hours previously spent tracking down missing charts.
- Reconciliation Accuracy: Automated pipelines pull historical data into active windows, eliminating manual data entry mistakes.
4. Better Revenue Cycle Evidence
Missing clinical evidence within billing documentation triggers frequent payer rejections and defers legitimate organizational revenue. In addition, establishing real-time data connectivity bridges the historical gap between clinical events and administrative tracking.
- Payer Adjudication: Ingestion pipelines optimize your revenue cycle integration cost by delivering clear prior authorization evidence access.
- Denial Remediation: Billing departments protect revenue streams by securing complete claim evidence at the initial submission.
- Audit Protection: Coding workflows remain highly accurate because compilers have immediate access to complete, structured coding support data.
For a deeper breakdown of revenue-focused automation, see our guide on AI Revenue Cycle Management Software Development. Consequently, compiling robust clinical justification at the point of care drives down overall denial volume.
5. Faster Post-Acquisition Integration
Integrated health systems often acquire regional hospitals faster than internal IT teams can manually deploy custom interface architectures. Conversely, a reusable, multi-tenant interoperability platform eliminates the need to engineer custom code for each new corporate asset.
- Onboarding Acceleration: Onboarding subsequent facilities follows pre-built architectural patterns, reducing deployment delays from months to weeks.
- Standardized Playbooks: Acquired facilities adapt to pre-existing mapping templates, which limits localized configuration friction.
- Rapid Asset Unification: New facilities achieve complete data connectivity quickly, accelerating clinical and financial consolidation.
Therefore, a centralized integration framework transforms post-acquisition technology alignment into a predictable, programmatic task. Thus, health systems reduce enterprise integration timelines and secure rapid market-expansion value.
6. AI-Ready Data for Future Use Cases
Deploying sophisticated clinical intelligence software fails if algorithms are fed fragmented, unnormalized local data streams. In contrast, an enterprise integration platform continuously cleanses and organizes clinical transactions into structured longitudinal records.
- Algorithmic Foundation: Normalized data pipelines provide the clean data streams necessary for automated population health tracking.
- Predictive Alerting: Real-time data feeds allow clinical decision systems to execute predictive risk scoring and catch care gaps early.
- Operational Intelligence: High-fidelity data structures enable the deployment of advanced denial prediction models and automated workflow routing.
For a deeper breakdown of healthcare automation use cases, see our guide on AI Healthcare Automation Platform Development. Ultimately, establishing a clean data layer ensures your architecture is immediately ready for advanced machine learning tools.
The ROI case should never depend on one metric. The business case becomes stronger when it combines duplicate testing savings, labor savings, revenue protection, acquisition speed, compliance readiness, and AI-readiness.
Compliance and Regulatory Costs to Plan For
Compliance costs should be planned from the start because Protected Health Information (PHI) moves through APIs, message queues, logs, dashboards, databases, cloud services, vendors, and support workflows.
For a $250,000 to $750,000 first-phase platform build, security and compliance engineering typically accounts for $35,000 to $110,000 of the initial capital budget. Failing to embed these guardrails early forces expensive architectural rewrites when security teams block deployment during pre-live validation reviews.
1. HIPAA and PHI Security
Securing health data transport requires deploying continuous encryption protocols that cover data fields both while moving across networks and when resting in databases.
Consequently, the underlying architecture must eliminate plain-text transmission risks by establishing automated cryptographic key management loops.
- Boundary Protection: Implementation teams allocate a portion of the HIPAA compliance integration cost line to establish point-to-point data encryption integration cost standards.
- Access Entitlements: Developers embed strict role-based access control integration protocols to restrict data visibility to verified clinical or administrative credentials.
- Immutable Tracking: Code blocks create a tamper-proof audit trail integration platform framework to record every external query or record mutation automatically.
Therefore, meeting strict PHI security integration rules requires treating infrastructure logs as highly sensitive data stores. As a result, vendor agreements must secure native BAA requirements integration vendors’ sign-offs before any live data crosses the integration hub.
2. CMS and ONC Interoperability Planning
EHR platforms must align with evolving federal interoperability standards to prevent severe institutional reimbursement penalties. Meanwhile, federal compliance mandates require underlying health IT architectures to adopt standardized data transport formats.
- Data Object Upgrade: Systems must accommodate modern USCDI v3 datasets to satisfy current ONC HTI-1 rule compliance cost parameters.
Invene - Prior Auth Modernization: Architectures must implement structured API pathways to manage the incoming CMS interoperability rule compliance cost frameworks.
Agadia Systems - Reimbursement Protection: Deploying open data pipelines prevents administrative penalties by demonstrating active information blocking rule compliance.
According to the Office of the National Coordinator (ONC), certified health systems must expose clinical records via standardized FHIR R4 interfaces.
For this reason, establishing a patient access API compliance cost line ensures your network satisfies core transparency mandates. Consequently, proactive engineering prevents your health system from facing sudden CMS validation failures.
3. Security Testing and Assurance
Validating code infrastructure against specialized hostile intrusion scenarios represents a major capital line item before live data activation. In addition, configuring modern zero-trust integration architecture structures demands strict validation of cross-network traffic.
- External Attestation: Engineering teams allocate resources toward checking core data pipelines to satisfy SOC 2 compliance integration cost audits.
- Hostile Vulnerability Scans: Budget lines cover detailed penetration testing integration cost requirements to uncover fragile endpoint variables.
- Long-Term Framework Alignment: Code architecture is constructed to match strict regulatory compliance integration cost guidelines, preparing data structures for a future HITRUST certification cost profile.
Ultimately, completing these defensive validation sprints provides institutional leaders with verifiable proof of platform structural safety. Because of this, third-party assessors can audit your data exchange loops without uncovering exposed unencrypted log fields. Thus, entering production remains highly predictable because core security barriers are fully verified under stress.
Compliance is not a final checklist. It shapes architecture, access control, vendor selection, testing, monitoring, and long-term support.
Total Cost of Ownership After Go-Live
Enterprise EHR integration platform total cost of ownership includes maintenance, vendor fees, cloud infrastructure, mapping updates, monitoring, security reviews, support staffing, and new facility onboarding.
For a $250,000 to $750,000 first-phase build, the annual operating cost usually starts around $45,000 to $187,500 before major new rollout waves. Health networks must recognize that go-live is not a financial finish line but the start of a recurring operational lifecycle.
1. Post-Go-Live Operational Cost Matrix
| TCO Category | What It Includes | Planning Range |
| Maintenance & Support | Bug fixes, vendor changes, small updates | 18%–25% of initial build cost |
| Vendor Fees | API access, marketplace licensing, interface fees | Vendor-dependent (Per-call/seat) |
| Cloud Infrastructure | Compute instances, data pipelines, message queues | $18,000–$90,000 yearly |
| Mapping Updates | Code modifications, terminology adjustments | $20,000–$85,000 yearly |
| Monitoring | Live feed tracking, latency alerts, dashboards | $25,000–$100,000 yearly |
| Security Reviews | Access audits, continuous penetration testing | $15,000–$75,000 yearly |
| New Site Onboarding | Adding additional hospitals or acquired facilities | $15,000–$45,000 per facility |
| Internal Staffing | Project owners, data stewards, integration leads | Organization-dependent |
2. Cloud and Data Storage Costs
Managing a healthcare data pipeline cost structure requires matching cloud consumption models with the real-time processing demands of your hospital network.
Consequently, the initial setup budget must account for continuous compute charges that scale alongside your network transaction metrics.
- Ingestion Processing: System fees expand as your data exchange volume cost scales, requiring dedicated servers to clear messaging buffers safely.
- Pipeline Transformations: Running a high-capacity ETL pipeline healthcare cost profile involves serverless compute spending to convert raw payloads into structured schemas.
- Throughput Variables: Managed environments like AWS HealthLake enforce specialized structural pricing, billing roughly $0.27 per hour per datastore alongside structured storage tiers.
Therefore, your monthly cloud statement varies based on the overall transaction throughput cost metrics across the network. As a result, unoptimized formatting or redundant API queries quickly inflate your base storage fees. Consequently, technical teams must implement caching strategies to balance low latency with flat infrastructure expenditures.
Build a 50-Hospital EHR Integration Roadmap With Intellivon
Intellivon helps hospital networks design EHR integration roadmaps that connect clinical, operational, financial, and patient data across multiple facilities without creating fragmented workflows, duplicate records, or unstable point-to-point interfaces.
For a 50-hospital system, EHR integration is not only a technical project. It is a phased transformation that must account for different EHR vendors, legacy systems, specialty workflows, data formats, security rules, clinical ownership, and rollout risk.
A. What Intellivon Helps You Plan
- Multi-hospital integration discovery: Map every EHR, departmental system, interface, data source, vendor dependency, and clinical workflow across the hospital network.
- EHR vendor and system alignment: Plan integrations across Epic, Oracle Health/Cerner, Meditech, athenahealth, custom EHRs, LIS, RIS, PACS, billing systems, claims platforms, pharmacy systems, and patient portals.
- FHIR, HL7, and API architecture: Define how patient demographics, encounters, orders, results, medications, allergies, notes, scheduling, referrals, and billing data should move across systems.
- Data mapping and standardization: Create a unified data model that reduces duplicate records, inconsistent fields, broken handoffs, and reporting gaps across hospitals.
- Security and compliance planning: Define HIPAA-ready access controls, audit logs, encryption, consent rules, role-based permissions, data retention, and integration monitoring requirements.
- Phased rollout strategy: Group hospitals by complexity, EHR type, readiness, interface dependencies, and operational risk so implementation happens in controlled waves.
- Testing and cutover planning: Build validation plans for data quality, interface performance, user access, downtime risk, clinical safety, and go-live support.
B. When to Build a 50-Hospital EHR Integration Roadmap
A roadmap becomes essential when a hospital network is merging systems, standardizing EHR workflows, launching AI tools, building enterprise analytics, modernizing patient access, or connecting multiple hospitals after acquisition.
It is especially important when each facility has different EHR configurations, departmental tools, data formats, interface engines, reporting needs, and compliance processes. Without a roadmap, integration work becomes reactive, expensive, and difficult to govern.
C. What You Get Before Implementation Begins
Before engineering starts, Intellivon helps define your integration scope, system inventory, data flows, interface priorities, vendor dependencies, security requirements, rollout waves, governance model, cost range, timeline, and risk controls.
The early roadmap can include hospital readiness scoring, EHR integration architecture, FHIR and HL7 strategy, data mapping plans, interface modernization priorities, testing workflows, migration risks, clinical stakeholder alignment, and phased deployment planning.
D. Why This Matters
A 50-hospital EHR integration project can fail when teams treat every interface as a separate technical task. The real goal is to create a connected data foundation that supports safer care, faster operations, cleaner reporting, AI readiness, and better patient experience.
Intellivon builds EHR integration roadmaps around workflow reality first. That means every integration decision connects back to clinical usability, operational continuity, compliance, data quality, and long-term scalability.
If your hospital network is planning EHR consolidation, interoperability modernization, AI implementation, or enterprise data integration, start with a structured roadmap before development begins. Talk to Intellivon to scope your EHR landscape, integration architecture, rollout phases, compliance controls, cost range, and implementation plan.
Conclusion
A 50-hospital EHR integration roadmap should create one controlled path for data exchange, workflow alignment, security, and rollout governance. Because FHIR supports electronic healthcare information exchange, the roadmap must connect standards, legacy interfaces, vendor dependencies, and clinical workflows into phased execution.
The strongest plans reduce integration risk, improve data quality, protect continuity of care, and prepare the network for analytics, automation, and AI adoption
Things To Know About EHR Integration Development Cost
Q1. How much does EHR integration cost for 50 hospitals?
A1. EHR integration development cost for a 50+ hospital network usually starts at $250,000–$750,000 for the first controlled enterprise build. This phase covers priority HL7 feeds, FHIR APIs, data normalization, HIPAA controls, monitoring, UAT, and rollout support. However, full 50-hospital expansion should continue through later facility waves.
Q2. What is included in enterprise EHR integration platform cost?
A2. Enterprise EHR integration platform cost includes discovery, architecture, integration engine setup, HL7 v2 feeds, FHIR R4 APIs, CDA exchange, data mapping, light EMPI logic, HIPAA controls, audit trails, testing, monitoring, and go-live support. However, vendor fees, interface licenses, infrastructure, and later facility onboarding should be estimated separately.
Q3. How long does a first-phase EHR integration build take?
A3. A first-phase EHR integration build usually takes 4–8 months. However, the timeline depends on vendor access, number of priority feeds, FHIR resource availability, data quality, UAT complexity, security review, and facility readiness. Therefore, larger rollout waves should begin only after the first phase proves architecture, performance, and ROI.
Q4. Is FHIR enough for multi-hospital EHR integration?
A4. FHIR is not enough for most multi-hospital EHR integration projects. Although it improves standardized API-based data access, large health systems still need HL7 v2, CDA, legacy feeds, integration engines, EMPI, terminology mapping, monitoring, security controls, and workflow validation. Therefore, FHIR should support the architecture, not replace it.
Q5. What ROI should a hospital expect from EHR integration?
A5. EHR integration ROI usually comes from fewer duplicate tests, faster chart access, lower manual work, cleaner revenue cycle evidence, better acquisition onboarding, stronger compliance readiness, and AI-ready data. However, the best ROI model tracks savings across clinical, financial, IT, compliance, and data teams instead of measuring interface completion alone.
Key Takeaways
- A $250,000–$750,000 EHR integration budget should be positioned as the first controlled enterprise build, not the full cost of connecting all 50 hospitals.
- The first phase should prove architecture, data quality, security, monitoring, UAT, and ROI before broader rollout.
- The most overlooked cost is clinical data normalization, not API development.
- Hospital 51 becomes cheaper only when the first build creates reusable architecture, mappings, test scripts, and support patterns.
- EHR integration ROI should combine duplicate testing reduction, manual work savings, revenue cycle visibility, acquisition speed, compliance readiness, and AI-ready data.



