

Key Takeaways:
-
Prior auth automation requires requirement detection, payer criteria matching, and clinical documentation extraction.
-
FHIR R4 prior auth APIs, HL7 CRD/DTR/PAS readiness, and medical necessity validation are core requirements.
-
Submission automation, status tracking, denial appeal support, audit trails, and human review queues are essential.
-
Production-grade AI prior authorization platforms cost $120,000 to $420,000 depending on scope and complexity.
-
Intellivon builds prior authorization systems as controlled healthcare infrastructure where AI prepares, and humans approve.
The core features that matter most in prior authorization automation are clinical criteria matching, NLP documentation extraction, and a payer-specific rules engine. These three are what actually reduce denial rates. Everything else, like status tracking, dashboards, and notifications, supports the workflow but does not move the approval number.
The platforms that genuinely reduce denial rates build clinical criteria matching directly into the automation layer, not just the submission process. This means the system checks clinical notes against payer requirements and catches documentation gaps before the request goes out, rather than after a denial comes back.
Organizations that do this consistently see PA approval rates improve by 20 to 30% within 6 months, and the AMA estimates prior auth tasks consume nearly two full business days of physician time per week.
Intellivon has spent over a decade building prior authorization automation with CMS 2026 compliance designed in from day one, not retrofitted afterward. This post walks through the core prior auth automation features that actually move outcomes, what each one does, and what to evaluate before committing to a build.

What is a Prior Authorization Automation Platform?
A prior authorization automation platform is a software system that manages payer approvals for medical procedures, medications, and services. Rather than staff submitting requests manually, the platform handles submission, criteria checking, and status tracking.
It pulls clinical data from the EHR and checks it against payer requirements in real time. So the system catches documentation gaps before the request reaches the payer, which means faster approvals and far fewer denials.
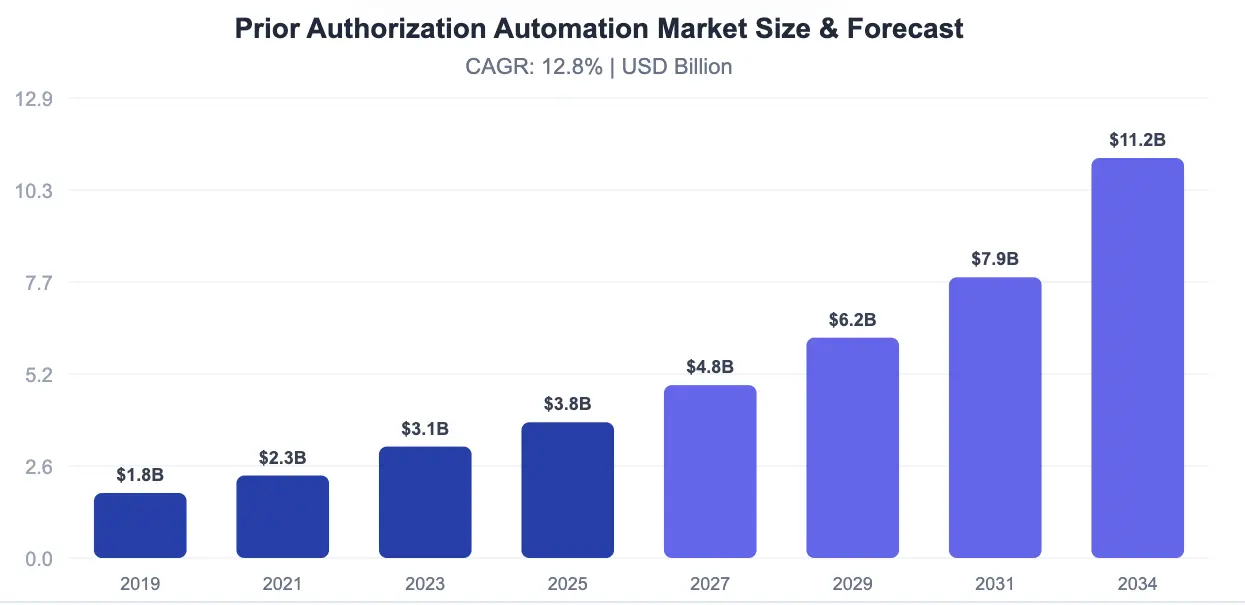
Why Are Hospitals Choosing To Adopt This?
Healthcare organizations are rapidly adopting prior authorization automation platforms as the global market grows at 12.8% CAGR, projected to reach $11.2 billion by 2034. CMS mandates on electronic prior authorization (ePA) and rising administrative burdens are forcing providers to automate manual processes.
1. CMS Regulatory Mandates Drive Adoption
The Centers for Medicare & Medicaid Services (CMS) now mandates electronic prior authorization (ePA) for Medicare Advantage plans, requiring API integration by 2027.
This regulatory push makes automation platforms essential, not optional, for healthcare providers and payers to comply with federal requirements.
2. Administrative Burden Crisis
Healthcare practices complete 41 prior authorizations per physician per week, consuming 13–14 hours weekly (nearly two full business days).
Manual processes create massive bottlenecks, delaying patient care and burning out staff. Automation eliminates these inefficiencies while accelerating approval times.
3. Proven ROI and Speed Improvements
AI-based prior authorization platforms deliver 30–50% faster approval times while reducing operational costs by 40–60%.
The AI-based segment specifically is growing at 19.38% CAGR, reaching $4.21 billion by 2031. Major players like Optum, Availity, Cohere Health, and Olive AI dominate this space.
4. EHR Standardization Enables Integration
HL7 FHIR API standards now enable seamless EHR-payer connectivity, making automation platforms technically feasible.
North America holds 46.3% market share ($1.76B) with healthcare providers as the largest segment at 44.7%. Infrastructure is ready for widespread adoption.
The combination of CMS mandates, administrative burden, proven ROI, and technical readiness makes prior authorization automation platforms a strategic imperative for healthcare organizations competing in 2026.
What Should Prior Auth Automation Features Actually Do?
Prior auth automation features should automate the full authorization lifecycle, not only submission. The platform should detect requirements, validate payer criteria, extract clinical documentation, prepare supporting evidence, submit requests, track responses, route exceptions, generate appeals, and report outcomes.
This turns prior authorization workflow automation into controlled infrastructure instead of task-level digitization.
1. Core Lifecycle Capabilities
True prior authorization automation replaces manual chart chasing with automated, end-to-end data pipelines. To help your team evaluate technology, true prior auth automation features should be judged by outcomes, not demo screens.
- Electronic Prior Auth (ePA) vs. AI Automation: Legacy software simply digitizes forms, forcing staff to paste notes manually. Modern systems use AI to read charts, check rules, and manage the entire revenue cycle without constant human intervention.
- Multi-Channel Submission: The platform must use a FHIR R4 prior auth API to communicate instantly with modern payer networks. For older systems, it uses robotic process automation (RPA) for automated payer portal navigation.
- Specialized Transaction Handling: Your system must support pharmacy benefits via NCPDP ePA automation and the NCPDP SCRIPT standard prior auth. It must also handle complex medical benefits like surgical or radiology prior auth automation.
- Balanced Feature Framework: A complete AI prior authorization platform feature checklist must balance clinical accuracy, technical EHR integrations, CMS compliance, and revenue cycle safety.
2. Feature Category Breakdown
To make these capabilities easy to review, the table below organizes the core functional layers.
This framework shows what each feature category does and how it affects your clinical operations.

| Feature Category | Core Purpose | Operational Impact |
| Requirement Detection | Automated checking of insurance rules at the point of care. | Eliminates unnecessary authorization attempts entirely. |
| Criteria Matching | Matches clinical notes against specific payer medical policies. | Prevents missing documentation before submission occurs. |
| Clinical Extraction | Uses NLP clinical criteria matching to find evidence in the EHR. | Reduces manual chart review time for clinical staff. |
| Medical Necessity Validation | Verifies that the pulled evidence meets InterQual or MCG rules. | Boosts approval rates by catching gaps early. |
| Submission Automation | Sends completed requests via API or portal automation. | Removes manual typing and speeds up PA submission automation. |
| Status Tracking | Continually checks payer systems for decisions. | Provides real-time visibility into authorization status. |
| Denial & Appeal Support | Automates clinical justification generation for denied claims. | Speeds up the PA denial appeal workflow dramatically. |
| Human Review Workflow | Routes complex exceptions to staff based on confidence scores. | Maximizes staff productivity by filtering simple cases. |
| Compliance & Audit | Logs every AI action, user click, and data transmission. | Ensures absolute readiness for strict healthcare audits. |
| Analytics & Reporting | Tracks turnaround times and active denial patterns. | Provides the financial data needed to measure exact ROI. |
A prior authorization platform should reduce manual work and improve authorization quality at the same time. Therefore, the first serious feature layer is not submission. It is knowing whether authorization is needed in the first place.
This requirement detection phase acts as the foundation for the entire automated workflow. Without accurate rules engine checks, your team will waste hours submitting requests that payers do not actually require. Consequently, let us look at how advanced platforms automate requirement checking directly within the clinical workspace.
Authorization Requirement Detection Comes First
Authorization requirement detection is the first feature because every downstream workflow depends on it. The system must determine whether a CPT code, ICD-10 diagnosis, drug, device, imaging order, surgery, home health service, or DME request needs prior authorization for a specific payer, plan, patient, and care setting before staff build a packet.
1. CPT and ICD-10 Code Diagnostics
This initial step ensures that every medical procedure and diagnosis code accurately aligns with insurance coverage rules. Specifically, the system scans clinical orders immediately to cross-reference codes with payer databases.
The software conducts automated ICD-10 diagnosis prior auth matching and CPT procedure prior auth matching simultaneously. Therefore, your billing team avoids wasting valuable administrative time on procedures that are already fully covered.
2. Multi-Payer Coverage Logic
Managing multiple insurance networks requires an engine that adapts instantly to changing rules across different commercial and government plans. This capability provides multi-payer prior auth support by unifying different rules into a single query engine.
The system performs payer-specific criteria matching by reading the patient’s exact policy group number. Because insurance companies change rules often, the software handles payer criteria update management and criteria decay management prior auth automatically.
3. Medication and Specialty Drug Checkers
Pharmacy benefits operate under highly strict rules that require faster processing times than typical medical procedures. This specialized layer handles medication prior auth automation and specialty drug prior auth logic simultaneously.
The software checks active plan formularies to confirm step therapy rules or dosage limits automatically. Consequently, the team can submit a complete clinical justification without manual research.
4. Specialized Service Routing
Different care types require completely distinct evaluation tracks, making rigid, one-size-fits-all automation tools highly ineffective. This feature layer provides specialized logic for durable medical equipment authorization alongside behavioral health prior auth routines.
For instance, radiology prior auth automation focuses heavily on matching imaging guidelines with clinical notes. Meanwhile, surgical prior auth automation handles multiple related procedures inside a single operating room event.
Requirement detection prevents unnecessary work before it starts. According to the Council for Affordable Quality Healthcare (CAQH), manual authorization tracking costs providers billions in administrative waste (CAQH Index). However, detection alone cannot raise approval rates. The next layer must prove that the requested service meets payer criteria.
Criteria Matching Is the Core Approval Feature
Prior auth criteria checking is the core approval feature because payers approve evidence, not requests. The platform must compare the patient’s diagnosis, history, test results, failed therapies, contraindications, and provider notes against payer-specific medical necessity rules before submission.
This is where AI prior auth automation platform features create measurable approval-rate lift.
1. InterQual and MCG Criteria Automation
This step converts complex insurance guidelines into structured checklists that can be verified automatically. Specifically, standard clinical guidelines must be ingested continuously to prevent criteria decay.
The software runs InterQual criteria automation and MCG criteria automation side by side. Consequently, it maps patient charts directly to industry-standard medical necessity logic.
Therefore, your care managers do not have to flip through physical books or separate software screens. This integration keeps your team aligned with active utilization management standards.
2. Milliman and Private Payer Verification
Some criteria are highly structured, but private payer rules are often hidden inside PDF attachments, portals, or local coverage policies. This layer handles Milliman criteria checking alongside highly customized payer-specific criteria matching.
The system uses versioned criteria ingestion to read, catalog, and store these fragmented rules automatically. Every criteria rule displays an effective date, source, payer, service line, and tracking confidence score.
As a result, your team avoids using outdated guidelines that lead to immediate rejections. This protects your revenue cycle from sudden, unannounced rule shifts.
3. Medical Necessity Documentation Automation
This component acts as an automated quality check by verifying that your submission contains all required medical proof. Specifically, the system manages medical necessity documentation automation and supporting documentation automation simultaneously.
The engine uses NLP clinical criteria matching and LLM prior auth documentation tools to extract relevant evidence. Therefore, it eliminates the manual typing that slows down your care coordination teams.
Furthermore, it builds a cohesive clinical justification generation summary directly from the provider’s recorded notes. This summary presents a clear timeline of the patient’s condition for the insurance reviewer.
4. Completeness and Confidence Scoring
Before any data leaves your system, the platform analyzes the gathered evidence to calculate an objective completeness score. This score specifically identifies missing lab results, progress notes, imaging files, prior therapies, or duration data.
Packets that fall below your target confidence threshold are instantly blocked from auto-submission. The system uses exception routing prior auth to send these low-confidence packets directly to your clinical staff.
If a critical piece of evidence is entirely absent, physician query automation prior auth flags the ordering doctor. This pre-submission check ensures that you only transmit airtight requests to payers.
5. Formulary and Step Therapy Tracking
Pharmacy benefits require highly specialized checking routines due to complex drug tiers and substitution rules. This feature manages step therapy automation and formulary exception automation inside the same clinical workflow.
It checks the patient’s specific plan to see if they must try preferred medications first. If a patient has a contraindication, the system pulls that medical restriction from the chart automatically.
Consequently, the platform builds a complete formulary exception packet without forcing staff to run manual checks. This keeps specialty drug approvals moving forward without unnecessary delays.
Criteria matching is where automation shifts from speed to outcome quality. According to the American Medical Association (AMA), 94% of physicians report that prior authorizations cause care delays (AMA Survey). Once the platform knows what evidence the payer needs, it must find that evidence inside the EHR.
This validation layer ensures that no incomplete packet ever reaches an insurance reviewer. By establishing a rigorous internal check, you directly reduce your overhead costs and shorten care delays. Consequently, let us examine how deep EHR integrations extract this clinical data smoothly at the point of care.
Clinical Documentation Extraction Must Be Evidence-Aware
Clinical documentation extraction prior auth features should pull the exact evidence needed for a payer rule, not summarize the chart generically.
The system must extract diagnoses, medications, failed therapies, lab values, imaging results, procedure history, functional limitations, provider notes, and contraindications from structured and unstructured EHR data.
1. NLP Narrative Analysis
This technical layer scans unstructured clinical text to identify critical medical facts that standard databases often miss. Specifically, natural language processing models isolate specific historical details like the duration of a patient’s symptoms or past therapeutic failures directly from progress notes.
- Targeted Text Extraction: Isolates timeline events, symptom severity, and past medication trials buried in unstructured notes.
- NLP Clinical Criteria Matching: Translates free-text clinical notes into discrete data points that align with specific insurance rules.
- EHR Integration Prior Auth Integration: Connects your narrative analysis directly with clinical documentation extraction prior auth systems.
Therefore, it replaces the manual reading process that traditionally consumes hours of nursing time. This data pipeline ensures that no vital piece of documented history is overlooked during the compilation phase.
2. LLM Evidence Synthesis
Large language models process the extracted clinical facts to construct a cohesive summary optimized for insurance review pipelines. Specifically, these models compile disparate elements like recent lab trends and medication changes into a concise clinical narrative.
- Automated Document Building: Compiles clinical documentation extraction prior auth elements into structured medical charts.
- LLM Prior Auth Documentation Generation: Drafts clear clinical summaries and letters based entirely on existing medical records.
- Retrieval-Augmented Generation Grounding: Binds every text generation to the clinical data extraction EHR source data to prevent hallucinated facts.
Therefore, your administrative teams do not have to write manual cover letters or text summaries for complex cases. Every single generated statement remains fully traceable back to real data found during the automated clinical chart scan.
3. Deep Electronic Health Record Syncing
A successful deployment relies entirely on direct, low-latency access to your core clinical databases where patient records reside. Specifically, the system connects via native webhooks to pull live updates the moment a physician completes an encounter note.
- Epic Prior Auth Integration Pipelines: Synchronizes real-time data from core Epic modules directly into the authorization software.
- Cerner Prior Auth Integration Links: Establishes secure, bidirectional communication with Cerner records for instant case creation.
- Practice Management Integration PA Webhooks: Connects patient schedules and demographic information with clinical care data.
As a result, your administrative workflow never operates on stale or outdated clinical information. These secure pathways ensure that clinical data moves instantly from the patient chart into the authorization pipeline.
4. OCR Document Digestion
Many authorization requests rely on external documents that arrive via legacy communication channels rather than direct digital feeds. This functional layer uses specialized optical character recognition engines to read scanned PDF referrals, outside lab reports, and incoming faxed records.
- Document Text Conversion: Transforms static image files, scanned notes, and incoming faxes into digital text.
- External Record Indexing: Tags and categorizes scanned documents automatically to match them with internal charts.
- Legacy Ingestion Pipelines: Imports unformatted data into the primary workflow without manual data entry.
Consequently, it unifies external records with your internal data architecture automatically. Therefore, your staff can use the same automated validation tools for out-of-network charts as they do for internal records.
5. Field-Level Confidence Scoring
Before any data moves to the next phase, an automated validation gate assesses the mathematical certainty of every extracted clinical element. Specifically, the system calculates an objective confidence score for each individual data point rather than scoring the case as a whole.
- Confidence Scoring Prior Auth Assessment: Calculates an explicit probability score for every extracted text value.
- Exception Routing Prior Auth Triggers: Automatically sends low-scoring extractions to a manual workflow.
- Human-In-The-Loop Prior Auth Review: Provides a dedicated dashboard where clinical experts can verify data fields.
Therefore, it prevents questionable or unverified data from reaching the insurance payer. This architecture delivers explainable AI prior auth decisions because your staff can review exactly why a case requires manual intervention based on clinical criteria validation.
Extraction gives the platform raw evidence. According to peer-reviewed health informatics research published in Health Affairs Scholar, provider staff spend the operational equivalent of 100,000 full-time registered nurses every year just navigating manual prior authorization administrative tasks (Health Affairs Scholar Analysis).
Submission Automation Must Support APIs, Portals, and Fallbacks
PA submission automation must support more than one submission path because payer connectivity remains uneven.
A strong platform should submit through FHIR APIs where available, use electronic prior authorization rails where supported, navigate payer portals when needed, and route exceptions when a payer requires manual documentation or additional review.
1. FHIR R4 and HL7 Da Vinci Readiness
Modern health networks must adopt standardized digital transmission protocols to remain compliant with changing federal insurance regulations.
Specifically, the Centers for Medicare & Medicaid Services (CMS) mandates that impacted government and commercial health plans deploy dedicated interoperability structures.
- FHIR R4 Prior Auth API Connectivity: Establishes direct, instant communication channels between provider networks and insurance systems.
- HL7 CRD Implementation Guide Alignment: Integrates the Coverage Requirements Discovery standard to find real-time plan rules at the point of care.
- HL7 DTR Implementation Specifications: Deploys Documentation Templates and Rules to gather precise medical necessity files inside the provider workflow.
- HL7 PAS Implementation Protocols: Drives Prior Authorization Support transactions to handle the core electronic packet delivery phase.
Therefore, your internal core systems require native components built to parse complex data objects according to standardized federal frameworks. These technical layers ensure absolute alignment with the CMS prior auth rule 2026 operational guidelines and the CMS prior auth automation compliance features framework.
2. Payer Portal and RPA Submission Layer
Many insurance organizations still rely heavily on legacy web architectures rather than modern data pipelines, creating severe connection fragmentation.
Specifically, this operational layer deploys robotic process automation tools to log into external health insurance portals when direct endpoints are missing.
- RPA Prior Auth Submission Routines: Fills out web forms automatically by moving structured medical data into portal fields.
- Payer Portal Navigation Software: Manages secure automated portal navigation, including multi-factor authentication and active session monitoring.
- Form Change Detection Frameworks: Scans web interfaces to flag layout updates before bad submissions break transmission streams.
- Bot Failure Recovery Protocols: Restarts stalled browser sessions instantly and alerts human teams if an interface lock occurs.
Consequently, it removes the manual data entry burdens that slow down clinical support staff. This dual-track architecture balances modern programmatic links with automated web extraction tools to maximize transaction success.
3. Pharmacy Benefit and Medication Frameworks
Pharmacy benefit paths require distinct communication standards to clear prescription drug claims rapidly at the point of dispensing.
Specifically, the system must interface with pharmacy benefit managers using separate regulatory rules than those used for inpatient or outpatient medical services.
- NCPDP ePA Automation Engines: Processes pharmacy benefit prior auth requests through dedicated real-time electronic transaction routes.
- NCPDP SCRIPT Standard Prior Auth Rules: Validates medication requests against standardized pharmacy framework transmission rules.
- Formulary Integration Checkers: Cross-references the drug request against active preferred medication listings automatically.
- Step Therapy Override Trackers: Attaches historical prescription success documentation to satisfy step requirements instantly.
Therefore, a unified system prevents pharmacy lines from splitting into manual standalone workarounds. By deploying dedicated script format routers, your medical group can clear specialized medications through the same central infrastructure used for major procedures.
4. Exception Routing and Validation Gates
When a submission route encounters an unexpected tech failure or an undocumented payer rule change, data transmission must be protected instantly. Specifically, an automated gate evaluates every transaction return code to identify submission errors or immediate document requests.
- Immediate Rejection Catchers: Intercepts transmission faults instantly to prevent broken requests from sitting in unviewed logs.
- Exception Routing Prior Auth Rules: Diverts failed automated attempts directly into an internal triage workspace for manual correction.
- Human-In-The-Loop Validation Workspace: Provides structured screens where billing teams can fix field errors without re-entering charts.
- Automated Attachment Appenders: Attaches missing PDF charts or imaging files to web portals when programmatic streams fail.
Consequently, your operational pipelines remain functional even when individual insurance portals change their underlying code overnight. This protective barrier keeps your technical submission metrics clean by preventing bad data loops from hitting external servers. It transforms a fragile script into a self-healing corporate transaction infrastructure.
Submission automation reduces data entry and payer chasing. According to operational studies published by the Council for Affordable Quality Healthcare (CAQH), moving from manual portals to fully automated electronic submission reduces transaction costs by over 80% per request (2025 CAQH Index Savings Report).
However, a submitted request still needs visibility, follow-up, and patient communication.
Which Features Improve Approval Rates vs Just Speed?
The most important prior auth automation features focus on approval quality, not just transaction speed. Specifically, submission bots reduce basic processing time, but deep features like pre-submission criteria matching drive true PA approval rate improvement.
Therefore, your platform must actively validate clinical evidence to achieve meaningful PA denial rate reduction across your entire enterprise revenue cycle.
Performance Impact Matrix
To help your technology teams choose between basic speed features and true quality-driving features, the framework below outlines how core capabilities affect your clinical and financial metrics.
| Feature Category | Mainly Reduces Time | Improves Approval Rate | Reduces Denials | Supports CMS Readiness | Buyer Priority |
| Requirement Detection | High | Medium | Medium | Medium | Must-have |
| Payer Criteria Matching | Medium | High | High | High | Must-have |
| Clinical Evidence Extraction | High | High | High | Medium | Must-have |
| Submission Automation | High | Low-Medium | Medium | High | Must-have |
| Status Tracking | High | Low | Medium | High | Must-have |
| Appeal Automation | Medium | High | High | Medium | Advanced |
| Gold Carding Tracking | Medium | Medium | Medium | Medium | Advanced |
| Analytics & Reporting | Medium | High over time | High over time | High | Must-have |
This operational impact framework gives technology leaders a clear evaluation lens before investing. For instance, tracking a gold carding feature prior auth or using payer performance analytics PA changes long-term financial outcomes.
Consequently, understanding these quality-driven capabilities prepares your organization for the upcoming custom development cost discussion.
How Much Do Prior Auth Automation Features Cost?
A custom platform with enterprise prior auth automation features usually costs $120,000–$420,000+, depending on EHR integrations, payer API connections, AI extraction models, CMS compliance scope, portal automation, analytics, security controls, and human review workflows. A focused MVP costs less, while multi-payer, multi-specialty infrastructure requires a larger build.
1. Breakdown by Engineering Phase
To provide full budgetary transparency, the table below outlines the precise dollar ranges and specific development scopes across every technical implementation phase.
| Development Phase | Estimated Cost Range | What It Includes |
| Discovery and Workflow Mapping | $8,000–$20,000 | PA volume analysis, payer mix, specialty workflows, current denial causes, build-vs-buy scope. |
| Architecture and Compliance Planning | $15,000–$35,000 | HIPAA design, PHI security, RBAC, audit trail model, API plan, data governance. |
| EHR and Practice Management Integration | $25,000–$90,000 | Epic, Cerner, athenahealth, HL7, FHIR, scheduling, RCM, case management integration. |
| Criteria Engine and Payer Rule Layer | $30,000–$85,000 | Payer-specific criteria matching, InterQual/MCG mapping, criteria versioning. |
| NLP and LLM Documentation Extraction | $35,000–$110,000 | Clinical note extraction, evidence matching, justification drafting, confidence scoring. |
| Submission and Payer Connectivity | $25,000–$95,000 | FHIR APIs, payer APIs, NCPDP ePA, RPA portal fallback, status polling. |
| Human Review and Queue Management | $20,000–$65,000 | Workload routing, exception queues, physician queries, reviewer approvals. |
| Analytics and ROI Dashboards | $18,000–$55,000 | Turnaround time, denial trends, payer performance, staff productivity, approval lift. |
| QA, Security Testing, and Deployment | $20,000–$60,000 | HIPAA checks, model testing, audit validation, UAT, production release. |
2. Long-Term Operating Maintenance Drivers
Deploying your platform into live production introduces ongoing operational management fees that scale with your infrastructure breadth. Specifically, annual maintenance typically tracks at 18%–28% of your initial capital construction cost.
Therefore, your financial modeling must account for continuous technical maintenance cycles rather than treating development as a single fixed cost.
- Payer Criteria Decay Upkeep: Requires recurring budget updates because commercial health plans frequently shift medical necessity guidelines without warning.
- Portal Automation Code Maintenance: Demands continuous monitoring because robotic script frameworks fail instantly if an insurance company alters their portal layout or security settings.
- Custom MLOps Infrastructure Monitoring: Drives data expenses to check for model drift, verify pipeline confidence scoring accuracy, and retrain neural networks on new provider charts.
These recurring expenses protect your initial technical layout from becoming obsolete. For a deeper breakdown of system sustainability and engineering models, see our guide on Cost to Develop Custom Hospital Software Platforms. Budgeting for routine adjustments ensures your pipeline maintains its structural accuracy over time.
What CMS and HIPAA Compliance Features Are Required?
CMS prior auth automation compliance features should include FHIR R4 API readiness, denial reason capture, decision-time tracking, public reporting support, prior authorization API workflows, audit logs, PHI protection, role-based access, encryption, and Business Associate Agreement readiness. Compliance should guide the feature roadmap, not sit at the end.
1. CMS Interoperability and Mandated FHIR APIs
Under the federal CMS interoperability prior auth rule, government-regulated health plans must establish standardized electronic data channels. Specifically, these pipelines allow health networks, insurers, and patients to exchange medical coverage data transparently.
- Prior Authorization API Integration: Manages the direct transmission of clinical evidence packets and automated tracking questions to payer servers.
- Provider Access API Pipelines: Permits safe peer-to-peer clinical data exchanges to coordinate treatment histories across active provider networks.
- Patient Access API Endpoints: Exposes approval timelines and real-time transaction statuses directly to patient-facing smartphone applications.
- Payer-to-Payer API Structuring: Transfers up to five years of historical medical records smoothly when an individual switches insurance coverage.
Consequently, these programmatic connections remove manual web portals and establish the core technical framework required for modern transaction tracking.
2. Shorter Response Windows and Denial Tracking
The CMS prior auth rule 2026 operational updates mandate rapid processing timelines and deep administrative clarity for all non-drug medical service claims. Specifically, health insurance plans must deliver specific, actionable textual justifications for every single rejected transaction.
- Accelerated Decision Timeframe Tracking: Monitors plan fulfillment of the mandated seven-day standard window and the 72-hour urgent processing limit.
- Denial Reason Capture Engines: Extracts specific rejection text strings from incoming electronic logs to coordinate instant clinical appeals.
- Public Metrics Reporting Monitors: Track running approval percentages and average processing delays across your various active commercial health plans.
- CMS Prior Auth Automation Compliance Features: Triggers automated timeline alerts to prevent payer processing delays from causing patient care issues.
Therefore, tracking these metrics directly inside your dashboard protects your organization from indirect operational bottlenecks when rules change.
3. Role-Based Access Controls and Data Shielding
Establishing a secure PHI prior auth platform requires strict identity validation rules across your entire operational computing landscape. Specifically, every single compiled medical evidence packet contains protected health information that requires absolute containment.
- Role-Based Access Control Prior Auth: Restricts chart visibility based on user duties, separating layouts for clinicians, billing clerks, and administrators.
- Zero-Trust Architecture Prior Auth Rails: Validates user identity and device security tokens continuously at every data extraction interface gate.
- Advanced Data Encryption Engines: Encrypts sensitive clinical data using modern cryptographic standards during both transmission and storage states.
- HIPAA Compliant Prior Authorization Automation Features: Regulates automated text processing models to stop unauthenticated users from exporting patient clinical data.
As a result, this defensive perimeter shields your medical records from data breaches and severe regulatory penalties.
4. Complete Audit Trails and Vendor Agreements
Achieving total HIPAA compliance prior auth standards requires comprehensive transaction logging of all automated and manual system modifications. Specifically, internal compliance officers must be able to reconstruct the operational lifecycle of any claim during formal federal investigations.
- Immutable Audit Trail Prior Auth: Logs every user view, data modification, submission attempt, and appeal generation event instantly.
- BAA Requirements Prior Auth Vendors: Outlines clear legal data protections that all downstream technology infrastructure developers must sign.
- Model Validation Auditing Protocols: Tracks automated text extraction confidence thresholds to show exactly why a script triggered a manual review flag.
- Exception Routing Log Modules: Records the complete chain of custody for patient records routed away from automated API lines.
Furthermore, this absolute audit readiness protects your medical enterprise during detailed federal data validation reviews.
Build vs Buy Prior Auth Automation Software Capabilities
Build custom prior auth automation software capabilities when your payer mix, specialty complexity, data ownership needs, integration requirements, or product roadmap exceed standard vendor coverage.
Buy when your workflows are simple, payer coverage is adequate, and your team needs fast implementation more than architectural control.
1. Strategic Implementation Comparison
The operational layout below evaluates how commercial off-the-shelf software packages match up against dedicated custom engineering pathways across critical business criteria.
| Feature Category | Buy (Commercial Vendor) | Build (Custom Architecture) | Hybrid (Integrated Framework) |
| Upfront Engineering Cost | Low initial software-as-a-service licensing fees. | Higher capital expenditure for initial layout. | Balanced procurement and development budget. |
| Market Deployment Speed | Immediate activation across standard structures. | Multi-month engineering lifecycle phases. | Fast baseline launch with rolling modular updates. |
| Workflow Customization | Rigid, generic configurations per default rules. | Absolute control over data pipelines. | Custom clinical front-end over vendor connections. |
| Data Ownership & Control | Vendor retains core model tracking assets. | Full proprietary equity of internal code bases. | Controlled storage of patient healthcare trends. |
| Payer Rule Flexibility | Dependent on external roadmap updates. | Immediate criteria engine optimization. | Flexible adjustment of complex clinical logic pathways. |
Deciding between building or buying your processing engines dictates your long-term revenue cycle resilience against health plan medical audits.
Ultimately, blending pre-built electronic transmission tracks with custom clinical data extraction engines delivers maximum operational scale without sacrificing organizational technical control.
How to Measure ROI From Prior Authorization Automation
ROI should be measured through authorization turnaround time, staff handling time, approval rate, denial rate, appeal success, avoidable cancellations, procedure scheduling speed, cash acceleration, and payer performance trends.
Prior auth automation software feature guide content should connect every feature to one measurable operational or financial outcome.
1. Operational and Financial Return Metrics
The table below breaks down the primary metrics that technology leads must monitor to calculate exact capital recovery and baseline performance increases.
| KPI | Why It Matters | Feature That Moves It |
| Average PA Turnaround Time | Protects patient access and scheduling. | Status tracking, payer follow-up. |
| Staff Minutes per PA | Measures productivity lift. | Submission automation, evidence extraction. |
| Approval Rate | Measures packet quality. | Criteria matching, documentation scoring. |
| Denial Rate | Measures avoidable revenue leakage. | Denial risk scoring, coding alignment. |
| Appeal Success Rate | Measures post-denial recovery. | Appeal automation, peer-to-peer prep. |
| Cancellation Rate | Measures schedule protection. | Real-time status, urgent workflows. |
| Payer SLA Performance | Shows payer bottlenecks. | Payer analytics dashboard. |
| Authorization-to-Claim Mismatch | Protects reimbursement. | Charge capture validation, coding alignment. |
Tying administrative metrics to clear software logic ensures your backend investment drives active revenue cycle prior auth integration goals. For instance, using detailed PA turnaround time reporting or deploying a dedicated authorization tracking dashboard surfaces exact performance bottlenecks.
For a deeper breakdown of billing-side revenue protection, see our guide on How to Build a Smart Healthcare Billing AI Platform. Relying on a payer performance analytics PA module alongside deep denial pattern analysis prior auth rules ensures your platform scales safely without losing capital to hidden billing errors or long insurance review delays.
How Intellivon Builds Prior Auth Automation Features
Intellivon builds custom prior auth automation features through a highly controlled engineering sequence. This framework covers workflow discovery, payer criteria mapping, EHR integration, clinical evidence extraction, submission orchestration, human review design, compliance controls, and production monitoring.
Consequently, this engineering approach keeps artificial intelligence completely useful, auditable, and safe inside real hospital operations.

Step 1 — Map PA Volume, Payers, and Service Lines
The first step maps where prior authorization work actually happens across your clinical enterprise. Teams must identify monthly request volume, payer mix, specialty lines, denial causes, turnaround times, staff workload, urgent cases, and high-dollar services.
Therefore, this baseline data prevents your development roadmap from copying a generic vendor feature list.
- Workflow Queue Ingestion: Isolates your active PA queue analysis alongside targeted payer and plan segmentation rules.
- Service-Line Ingestion: Conducts structured service-line segmentation to separate routine, complex, and urgent cases cleanly.
- Denial Reason Review: Examines historical rejection trends through targeted staff workflow interviews and deep denial reason review blocks.
Our team starts by separating routine, complex, urgent, and high-value authorization workflows. This focus helps define your minimum viable product around highly measurable clinical bottlenecks. Once the workflow is clear, the next step is payer criteria mapping.
Step 2 — Build the Payer Criteria Engine
The payer criteria engine defines what each request must prove before submission occurs. It stores active payer rules, plan policies, CPT requirements, ICD-10 logic, step therapy requirements, documentation fields, and effective dates.
This centralized engine becomes the primary technical control layer for automated medical necessity validation.
- Criteria Ingestion Architecture: Gathers multi-payer guidelines into versioned database objects cleanly using automated criteria ingestion.
- Effective Date Tracking: Manages criteria version control to prevent stale logic from corrupting internal data pipelines.
- Specialty Rule Mapping: Configures custom validation rails for InterQual/MCG mapping and localized specialty rule mapping.
We design payer criteria parameters as isolated, versioned objects. Therefore, sudden insurance updates never break the rest of your active workflow. Once the criteria are structured, the system needs clinical evidence.
Step 3 — Connect EHR and Clinical Data Sources
EHR integration gives the platform instant access to the evidence needed for prior authorization workflows. The system must connect patient demographics, diagnosis codes, procedure orders, medications, labs, imaging, encounter notes, referrals, and care plans. These elements link through secure FHIR, HL7, APIs, or approved developer networks.
- Core Database Pipelines: Deploys certified Epic prior auth integration and Cerner prior auth integration tools natively.
- Interoperable Data Feeds: Utilizes live FHIR R4 resources alongside legacy HL7 feeds for broad clinical data extraction.
- Practice Management Ingestion: Connects practice management data with active case management integration webhooks smoothly.
We design these data integrations specifically around the evidence fields needed for payer approval. Consequently, we avoid broad, risky data extraction processes. Once the data flows, AI can extract and match evidence.
Step 4 — Add NLP and LLM Evidence Extraction
NLP and LLM models should extract clinical evidence, match it to payer criteria, and generate source-backed justification drafts. They must never make final, autonomous authorization decisions.
The safest design uses AI to prepare medical evidence while forcing humans to approve high-risk submission packets.
- Semantic Text Extraction: Employs advanced NLP extraction to identify critical history inside unstructured clinical notes.
- RAG-Based Evidence Retrieval: Grounds language models securely to drive automated LLM justification drafting.
- Confidence Gate Frameworks: Activates automated confidence scoring to trigger missing documentation detection and human review triggers.
We build all intelligence outputs with strict, clickable traceability. Every generated statement points directly back to a verifiable clinical source. The next step turns evidence into payer-ready submissions.
Step 5 — Orchestrate Submission, Status, and Appeals
Submission orchestration sends clean packets through the best available channel and continuously tracks cases until a final decision is reached.
The system must support FHIR APIs, electronic rails, payer portals, RPA fallback, status polling, patient notifications, denial categorization, and automated clinical appeal packet drafting.
- Programmatic Core Delivery: Connects directly to modern networks using the official Prior Authorization API standard.
- Pharmacy Script Handling: Drives real-time prescription approvals using dedicated NCPDP ePA transactions.
- Payer Portal Automation: Deploys resilient web automation with integrated status webhooks and appeal workflow scripts.
We prioritize secure, API-first execution workflows across our systems. We deploy robotic portal navigation and peer-to-peer review prep fallbacks only where payer technology requires it. The platform is not finished until compliance and monitoring are active.
Step 6 — Add Compliance, Analytics, and Model Monitoring
The final step makes the platform completely measurable and auditable before production rollout. Technical teams require strict HIPAA controls, role-based access, audit trails, PHI security, model monitoring, payer criteria update management, dashboard reporting, and ROI measurement tools. This wraps your core automation features in protective governance layers.
- Identity and Access Shielding: Restricts core asset visibility using RBAC, an immutable audit trail, and database encryption.
- MLOps Monitoring Pipelines: Deploys proactive model drift tracking to catch language accuracy drops automatically.
- Criteria Decay Monitoring: Updates local business rules engines when commercial insurance guidelines change over time.
We treat infrastructure monitoring as a core component of the initial build phase. This step helps your custom ROI dashboard stay completely reliable after workflows alter. This build sequence prevents feature sprawl. It also gives CTOs a practical way to scope the platform before budget approval.
This structured implementation methodology prevents development sprawl across complex enterprise health networks. Ultimately, managing clinical criteria version control and building traceable data extractions ensures long-term system stability and direct capital recovery.
Build Prior Auth Automation Infrastructure With Intellivon
Intellivon designs prior auth automation infrastructure, so healthcare teams can reduce manual submissions, payer follow-ups, documentation gaps, and authorization delays without removing clinical and revenue cycle teams from the approval process.
Every AI-generated recommendation, documentation summary, payer-rule match, or appeal draft is built to remain reviewable, traceable, editable, and governed.
This gives hospitals, specialty practices, ambulatory surgery centers, RCM companies, and healthcare SaaS platforms a safer way to use AI for prior authorization without creating black-box approvals, unsupported clinical justifications, payer compliance risks, or more work for staff.
1. What Intellivon Helps You Build
- Prior auth requirement detection: Identify when a procedure, medication, device, imaging order, surgery, or specialty service needs authorization based on payer, plan, CPT code, ICD-10 code, and care setting.
- Clinical documentation extraction: Pull relevant notes, diagnoses, lab results, imaging references, failed therapies, medications, and medical necessity evidence from EHR and practice management systems.
- Payer criteria matching: Compare clinical evidence against payer-specific rules, InterQual, MCG, step therapy, formulary, documentation, and medical necessity requirements before submission.
- Submission and status automation: Support FHIR APIs, payer APIs, ePA workflows, portal submissions, status tracking, notification workflows, and exception routing across multiple payers.
- Human review and appeal workflows: Route uncertain cases to clinical, billing, or RCM teams, while supporting appeal packet generation, peer-to-peer preparation, and audit-ready review trails.
2. When to Build Prior Auth Automation Infrastructure
A custom prior auth automation platform makes sense when your team manages high authorization volumes, slow payer responses, frequent documentation gaps, complex specialty approvals, or repeated authorization-related denials.
It is also useful when generic prior authorization tools cannot match your payer mix, EHR setup, clinical workflows, CMS readiness needs, or reporting requirements.
This build is especially relevant if your organization handles radiology, oncology, infusion, surgery, behavioral health, DME, specialty pharmacy, home health, or multi-location authorization workflows. In these cases, basic submission automation may save time, but it will not solve the full authorization burden.
3. What You Get Before Full Development Begins
Before engineering starts, Intellivon helps your team define the prior authorization workflow, payer connectivity needs, clinical evidence gaps, compliance requirements, AI boundaries, reviewer permissions, and technical scope.
This gives clinical, revenue cycle, and technology leaders a clear build plan before investing in a production platform.
The early-stage roadmap can include:
- Prior auth workflow and payer mix assessment.
- EHR, FHIR, HL7, payer API, and portal integration planning.
- Clinical evidence extraction and criteria-matching architecture.
- Human review, exception routing, and appeal workflow design.
- MVP scope, cost range, timeline, and rollout roadmap.
4. Why This Matters
If your organization is evaluating prior auth automation features, start with a workflow and feature-readiness review before choosing models or vendors.
Talk to Intellivon to scope your payer connectivity, clinical documentation extraction, criteria-matching engine, human review controls, CMS readiness, analytics dashboard, development cost, and rollout roadmap before committing to a full build.
Conclusion
Prior auth automation features matter most when they improve evidence quality, reduce avoidable denials, and keep authorization work visible across clinical and revenue teams.
At the same time, basic automation can reduce clicks, but stronger systems connect payer criteria, clinical documentation, FHIR APIs, human review, appeals, and analytics into one controlled workflow.
For CTOs, VP of Clinical Operations, RCM leaders, and healthcare SaaS teams, the best roadmap starts with requirement detection and criteria matching before advanced AI. Once the foundation is stable, LLM documentation, status automation, appeal drafting, and payer analytics can create measurable ROI.
Things To Know About Prior Auth Automation Features
Q1. How long does prior authorization automation development take?
A1. A focused prior authorization automation MVP usually takes 12–16 weeks when the first release covers requirement detection, evidence extraction, and basic submission workflows. However, a production platform usually takes 5–9 months. Meanwhile, multi-specialty builds with Epic, Cerner, payer APIs, CMS reporting, and appeal workflows can take 9–14 months in practice.
Q2. What features should prior authorization automation include?
A2. Prior authorization automation should include requirement detection, payer criteria matching, clinical documentation extraction, medical necessity validation, submission automation, status tracking, appeal support, human review, audit trails, compliance controls, and analytics. Together, these features support the complete workflow from order placement to approval, denial, appeal, expiration, or follow-up action safely too.
Q3. What AI models are required for prior auth automation software capabilities?
A3. A strong platform usually needs NLP for clinical extraction, LLMs for justification drafting, rules engines for payer criteria, classification models for denial risk, and retrieval systems for source-grounded evidence. However, human review remains essential because uncertain outputs, clinical context, and reimbursement decisions need accountable review before submission or appeal approval.
Q4. What integrations matter most for enterprise prior auth automation features?
A4. The most important integrations include EHR systems, practice management platforms, payer APIs, FHIR R4 prior auth APIs, HL7 workflows, NCPDP ePA rails, case management tools, scheduling systems, RCM platforms, and patient notification systems. Without these connections, teams still copy data manually, even when the automation layer looks polished operationally daily.
Q5. Should hospitals build or buy prior auth automation software?
A5. Hospitals should buy when workflows are standard, payer coverage is already available, and speed matters more than control. However, they should build when they need data ownership, specialty workflows, deeper EHR integration, payer-specific criteria logic, custom analytics, or one platform that supports multiple locations, teams, and service lines reliably and securely.
Q6. What CMS prior auth automation compliance features are required?
A6. CMS-ready platforms should support prior authorization API workflows, denial reason capture, decision-time tracking, public reporting metrics, FHIR R4 readiness, Provider Access API awareness, and audit logs. Even when providers face indirect compliance pressure, these features help teams prepare for payer-side workflow changes, documentation demands, and interoperability expectations ahead by 2026.
To Sum Up:
- Prior authorization automation that only submits forms faster may reduce workload, but it will not reliably improve approval rates without criteria matching and evidence scoring.
- The most valuable AI feature is not clinical summarization. Instead, it is source-backed evidence extraction mapped to payer-specific medical necessity rules.
- CMS 2026 and 2027 readiness should be treated as product architecture, not a compliance footnote added after development.
- Payer portal automation should be a fallback layer, not the foundation, because portal changes can break fragile RPA workflows.
- Approval-rate improvement depends on documentation completeness, coding alignment, denial pattern analysis, and human review design working together.



