

Key Takeaways:
- Population health platforms require clinical data ingestion, cohort dashboards, care gap tracking, and outreach automation.
- EHR integration, claims data, patient matching, risk stratification, and HEDIS reporting are production-grade requirements.
- Care management workflows, audit trails, MLOps, and HIPAA-ready access controls ensure compliant platform operations.
- Lean MVPs start at $70,000 to $120,000 while production-ready platforms reach $250,000 to $450,000.
- How Intellivon builds population health platforms as healthcare data infrastructure connecting AI, compliance, and value-based care outcomes.
Building an enterprise population health platform costs between $70,000 and $450,000. That range is wide because data integration scope and risk model complexity drive costs in ways standard guides never break down by phase. So without phase-level numbers in hand, budget approval stalls, and this post gives you exactly what you need.
However, without separating your data integration architecture from your analytics build at the design stage, you will spend 40 to 60 % more correcting integrations post-launch. As a result, organizations that sequence development correctly, starting with data ingestion, then risk stratification, then care management, consistently reach positive ROI within 18 to 24 months. In fact, integrated population health programs with automated care gap closure have reduced total cost of care by up to 22% within two years.
Specifically, Intellivon has built healthcare AI systems with HIPAA compliance and data governance embedded into the architecture from the start, not retrofitted after. This blog covers every development phase and cost driver, from data integration and risk stratification to care management workflows, quality reporting, and ongoing maintenance. By the end, you will have a cost framework ready for a capital approval conversation.

What is an Enterprise Population Health Platform?
An enterprise population health platform is a centralized software system that aggregates patient clinical, claims, and social data across multiple networks. This unified data layer allows healthcare organizations to track patient groups, discover gaps in care, and deploy automated outreach campaigns.
Ultimately, these platforms use predictive models to balance financial risks in value-based care contracts.
Why Enterprises Need An Enterprise Population Health Platform
The global population health management market is expanding rapidly, reaching a value of 103.6 billion USD in 2025. According to market research from Fortune Business Insights, this sector will grow from 126.2 billion USD in 2026 to 514.1 billion USD by 2033, showing a steady annual growth rate of 22.2%.
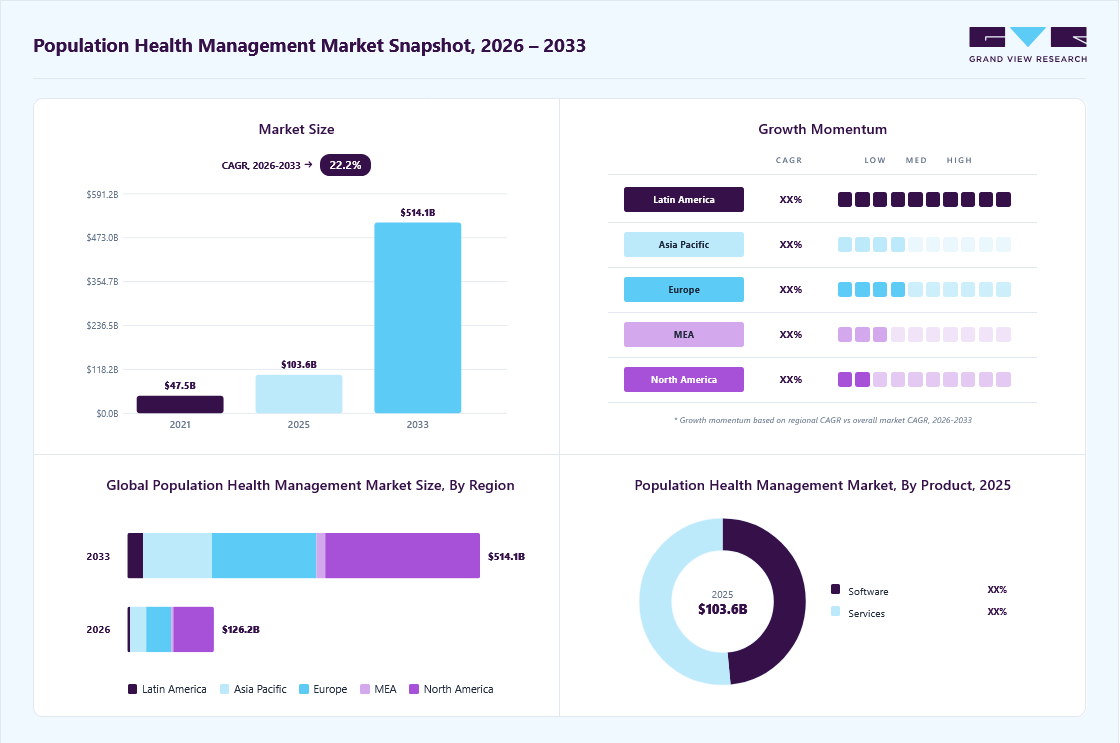
Consequently, North America continues to lead the space, commanding a dominant 46.0% share of the total global market.
1. Rising Healthcare Costs Demand Proactive Intervention
Increasing chronic disease burden and escalating healthcare costs are pushing organizations toward integrated digital solutions that identify at-risk patients before conditions worsen.
2. Value-Based Care Reimbursement Makes PHM Essential
The transition to Accountable Care Organizations (ACOs) and value-based contracting incentivizes hospitals to use PHM platforms to keep patients healthy and avoid costly hospitalizations.
3. Data Silos and Legacy Systems Block Care Continuity
60% of healthcare organizations still rely on legacy systems, creating interoperability gaps that fragment health information and jeopardize quality care. Enterprise platforms aggregate clinical data from multiple sources to enable proactive interventions.
Enterprises need population health platforms to reduce emergency visits by 12-18%, improve chronic disease control by 15-25%, and generate $50-150 per patient annually through value-based contract bonuses.
What A $70,000–$450,000 Population Health Platform Includes
A $70,000–$450,000 budget funds a controlled first release featuring focused data ingestion, patient matching, risk scoring, and care workflows. It delivers a production-ready enterprise foundation for up to three data sources, care gap tracking, and automated quality reporting. This range supports targeted value-based care operations rather than a national multi-tenant system.
This revised cost range assumes a highly controlled first release rather than a sprawling national system. Consequently, it does not include a full national multi-tenant SaaS product, dozens of concurrent EHR integrations, or costly HITRUST certification from day one.
- Exclusions: It also excludes complex payer-provider data exchange across many distinct markets, large-scale patient engagement applications, and advanced clinical decision support across every single disease area.
- Targeted Scope: Instead, this budget delivers a realistic enterprise foundation tailored for one to three priority data sources and one or two primary EHR environments.
The architecture reliably covers claims or eligibility file ingestion alongside a basic social determinants of health data cost structure.
Most importantly, it funds core clinical engines including a risk stratification model cost, care gap tracking, a custom population health analytics dashboard cost, and automated CMS reporting cost population health workflows.
Population Health Platform Scope
| Platform Scope | Cost Range | Best Fit |
| Lean MVP | $70,000–$120,000 | One population, limited data, basic care gap workflows |
| Controlled Enterprise MVP | $120,000–$250,000 | ACO, health plan, hospital, or SaaS team validating PHM operations |
| Production-Ready Enterprise Build | $250,000–$450,000 | Enterprise team scaling integrations, risk models, care workflows, and reporting |
Every system built within this tier must also account for a HIPAA compliance cost population health baseline, which includes data encryption, audit logs, and role-based access controls. Furthermore, early architecture choices will dictate your long-term ongoing maintenance cost population health trajectory.
- Engineering Baseline: At Intellivon, we ensure that these initial foundations use modular data pipelines so that teams can scale features without rewriting core code later.
- Strategic Growth: This approach protects your initial capital while ensuring the platform remains ready for multi-source data ingestion and complex terminology mapping when you are ready to scale.
This cost range is practical when the platform starts with the highest-value data and workflows. Therefore, leaders should avoid building every population health feature in the first release. Focusing on targeted data ingestion ensures the system delivers early, measurable financial returns.
Population Health Platform Cost By Build Tier
Population health platform cost changes significantly by build tier. A lean MVP usually costs $70,000–$120,000, a controlled enterprise MVP costs $120,000–$250,000, and a production-ready enterprise platform costs $250,000–$450,000. Each tier adds more integrations, AI model depth, workflow automation, reporting logic, and compliance controls.
The choice between these tiers depends entirely on your immediate operational scale and risk parameters. Choosing a tier without analyzing data sources will quickly lead to scope creep or budget overruns.
- Data Scale: The number of unique EHR feeds dictates your processing tier.
- Workflow Volume: Advanced automation requires higher investment to ensure clinical safety.
1. Tiered Population Health Platform Table
| Build Tier | Price Range | Primary Focus |
| Lean MVP | $70,000–$120,000 | Baseline data ingestion and simple patient list creation |
| Controlled Enterprise MVP | $120,000–$250,000 | Active care management and live EHR data feeds |
| Production-Ready Enterprise | $250,000–$450,000 | Advanced risk scoring, EMPI, and multi-source analytics |
2. Lean MVP Population Health Platform
A lean MVP population health platform usually costs $70,000–$120,000. This tier fits teams that need fast validation around patient cohorts, simple care gap identification, basic dashboards, limited outreach lists, and HIPAA-ready user access before investing in deeper EHR, claims, AI, or quality reporting automation.
- Data Ingestion: Technically, this step involves setting up one primary EHR export or standard API connection to establish a baseline for clinical data aggregation cost.
- Analytics Base: The architecture uses simple cohort analysis tools, cost frameworks, and a basic stratification dashboard cost to track high-risk groups.
- Care Gaps: Furthermore, the build includes basic care gap identification cost tracking based on flat-file or CSV claims ingestion.
- Security Core: It establishes role-based access population health cost parameters.
- Audit Base: It implements a basic audit trail for population health cost for data privacy.
Once the MVP proves data quality and workflow value, the next tier adds more integrations and workflow automation.
3. Controlled Enterprise MVP
A controlled enterprise MVP usually costs $120,000–$250,000. This tier works for hospitals, ACOs, Medicaid managed care teams, health plans, and healthcare SaaS companies that need EHR integration, claims data, patient matching, risk stratification, care management workflows, and HEDIS or CMS reporting in one controlled release.
- Clinical Ingestion: This level involves substantial EHR data integration cost population health work, deploying HL7 v2 integration population health cost loops and FHIR R4 population health cost services.
- Feeds & Claims: It combines standard claims data integration cost paths with live clinical updates, specifically tracking a dedicated admission-discharge-transfer cost framework and an automated ADT feed integration cost loop.
- Ancillary Data: The system also introduces lab results integration cost and pharmacy data integration cost modules.
- Identity Layer: It utilizes a custom patient matching algorithm cost block.
- Data Integrity: It uses a basic duplicate record management cost code to clean incoming files.
- Operational Tools: It launches a functional care management workflow cost engine.
- Automation: It deploys a patient outreach automation cost pipeline for automated messaging.
This structure builds the precise framework needed for HEDIS measure automation cost tracking and broader CMS quality program cost compliance. After the controlled MVP, a production-ready build adds stronger governance, AI monitoring, and broader reporting.
4. Production-Ready Enterprise Platform
A production-ready enterprise population health platform usually costs $250,000–$450,000. This tier includes stronger data normalization, multiple data sources, EMPI logic, AI risk models, care coordination workflows, value-based care reporting, HIPAA controls, MLOps basics, deployment support, and ongoing monitoring for enterprise use.
- Core Systems: The technical layer covers complex multi-source data ingestion cost structures across entirely separate health systems.
- Pipeline Setup: Engineers build advanced data normalization population health cost systems and clinical data normalization cost pipelines to handle mismatched files.
This requires deep terminology mapping cost population health routines, including SNOMED CT mapping cost logic, LOINC mapping population health cost tables, and RxNorm integration cost services alongside ICD-10 coding population health cost verification.
Selecting your build tier establishes your capital scope and integration roadmap. Consequently, teams must align their targeted patient population size and contract types with the corresponding architecture level before kickoff.
Enterprise Population Health Platform Build Cost Breakdown
An enterprise population health platform build cost breakdown should stay between $70,000 and $450,000 when the first release is focused. The largest cost areas are data ingestion, data normalization, patient matching, analytics, AI risk scoring, care workflows, quality reporting, HIPAA controls, deployment, and ongoing maintenance.
The phase-by-phase distribution of capital directly mirrors the engineering complexity of your underlying clinical data strategy. Consequently, evaluating these distinct investment zones prevents unexpected scope inflation during core pipeline construction.
- Integration Density: Expanding your active EHR footprint heavily shifts your initial configuration capital.
- Logic Specifics: Custom algorithmic tracking scales development costs based on targeted quality metric rules.
| Development Phase | Typical Cost Range | What It Covers | What Pushes Cost Higher |
| Discovery phase population health cost | $5,000–$18,000 | Population scope, contract goals, source inventory, workflow mapping, ROI baseline | Multiple teams, unclear measure ownership, complex reporting goals |
| Architecture and data governance | $8,000–$30,000 | Data model, access rules, lineage, consent logic, governance structure | Multi-entity governance, payer-provider data sharing |
| Data integration phase cost | $18,000–$95,000 | EHR data, HL7 v2, FHIR R4, claims, labs, pharmacy, ADT, SDOH | Multiple EHRs, HIE connectivity, custom APIs |
| Data normalization and patient matching | $12,000–$55,000 | SNOMED CT, LOINC, RxNorm, ICD-10, duplicate record management, EMPI logic | Poor identifiers, weak data quality, multiple facilities |
| Analytics development cost population health | $15,000–$70,000 | Cohort dashboards, stratification views, utilization analytics, quality dashboards | Custom dashboards, provider performance analytics |
| AI model development | $18,000–$85,000 | Risk scoring, rising risk, readmission prediction, ED utilization prediction | Multiple cohorts, model explainability, bias testing |
| Care management workflow build | $20,000–$85,000 | Care plans, outreach, referral tasks, SDOH tracking, care team collaboration | Community health worker features, multi-site routing |
| Quality reporting automation | $15,000–$75,000 | HEDIS, STARS, CMS, ACO, value-based care reporting | Payer-specific logic, audit files, measure versioning |
| HIPAA security and compliance | $12,000–$60,000 | PHI security, encryption, RBAC, audit trails, BAA requirements | SOC 2 readiness, zero-trust architecture, multi-tenant controls |
| Deployment and launch | $8,000–$35,000 | UAT, production setup, release support, validation, training support | Multi-facility rollout, parallel reporting validation |
| Ongoing maintenance cost | 15%–25% yearly | Interface support, measure updates, model monitoring, security patches | New measures, new contracts, new integrations |
Get Your Population Health Platform Cost Estimate
Planning a population health platform budget? Intellivon can map your EHR integrations, claims feeds, AI model scope, care workflows, reporting needs, HIPAA controls, and launch phases into a realistic $70,000–$450,000 development estimate.
- Engineering Validation: We review your active clinical schema to establish precise pipeline boundaries.
- Predictable Architecture: Our team scopes data normalization rules ahead of code deployment to secure capital efficiency.
The budget should not be presented as one vague software number. Instead, each cost phase should connect to a specific technical and operational outcome.
For a deeper breakdown of building interoperable health networks, see our guide on how to build a health information exchange platform. This video explains technical foundations like FHIR R4 mapping and identity matching, which directly influence your overall clinical data aggregation budget.
What Drives Custom Population Health Platform Development Cost?
An enterprise population health platform build cost breakdown should stay between $70,000 and $450,000 when the first release is focused. The largest cost areas are data ingestion, data normalization, patient matching, analytics, AI risk scoring, care workflows, quality reporting, HIPAA controls, deployment, and ongoing maintenance.
The phase-by-phase distribution of capital directly mirrors the engineering complexity of your underlying clinical data strategy. Consequently, evaluating these distinct investment zones prevents unexpected scope inflation during core pipeline construction.
- Integration Density: Expanding your active EHR footprint heavily shifts your initial configuration capital.
- Logic Specifics: Custom algorithmic tracking scales development costs based on targeted quality metric rules.
| Development Phase | Typical Cost Range | What It Covers | What Pushes Cost Higher |
| Discovery phase population health cost | $5,000–$18,000 | Population scope, contract goals, source inventory, workflow mapping, ROI baseline | Multiple teams, unclear measure ownership, complex reporting goals |
| Architecture and data governance | $8,000–$30,000 | Data model, access rules, lineage, consent logic, governance structure | Multi-entity governance, payer-provider data sharing |
| Data integration phase cost | $18,000–$95,000 | EHR data, HL7 v2, FHIR R4, claims, labs, pharmacy, ADT, SDOH | Multiple EHRs, HIE connectivity, custom APIs |
| Data normalization and patient matching | $12,000–$55,000 | SNOMED CT, LOINC, RxNorm, ICD-10, duplicate record management, EMPI logic | Poor identifiers, weak data quality, multiple facilities |
| Analytics development cost population health | $15,000–$70,000 | Cohort dashboards, stratification views, utilization analytics, quality dashboards | Custom dashboards, provider performance analytics |
| AI model development | $18,000–$85,000 | Risk scoring, rising risk, readmission prediction, ED utilization prediction | Multiple cohorts, model explainability, bias testing |
| Care management workflow build | $20,000–$85,000 | Care plans, outreach, referral tasks, SDOH tracking, care team collaboration | Community health worker features, multi-site routing |
| Quality reporting automation | $15,000–$75,000 | HEDIS, STARS, CMS, ACO, value-based care reporting | Payer-specific logic, audit files, measure versioning |
| HIPAA security and compliance | $12,000–$60,000 | PHI security, encryption, RBAC, audit trails, BAA requirements | SOC 2 readiness, zero-trust architecture, multi-tenant controls |
| Deployment and launch | $8,000–$35,000 | UAT, production setup, release support, validation, training support | Multi-facility rollout, parallel reporting validation |
| Ongoing maintenance cost | 15%–25% yearly | Interface support, measure updates, model monitoring, security patches | New measures, new contracts, new integrations |
Get Your Population Health Platform Cost Estimate
Planning a population health platform budget? Intellivon can map your EHR integrations, claims feeds, AI model scope, care workflows, reporting needs, HIPAA controls, and launch phases into a realistic $70,000–$450,000 development estimate.
- Engineering Validation: We review your active clinical schema to establish precise pipeline boundaries.
- Predictable Architecture: Our team scopes data normalization rules ahead of code deployment to secure capital efficiency.
The budget should not be presented as one vague software number. Instead, each cost phase should connect to a specific technical and operational outcome.
Population Health Platform Architecture Cost
Population health platform architecture cost comes from creating a trusted data-to-action loop. The platform must collect data, normalize it, match patients, score risk, identify care gaps, trigger care workflows, measure quality performance, and maintain HIPAA controls across every layer.
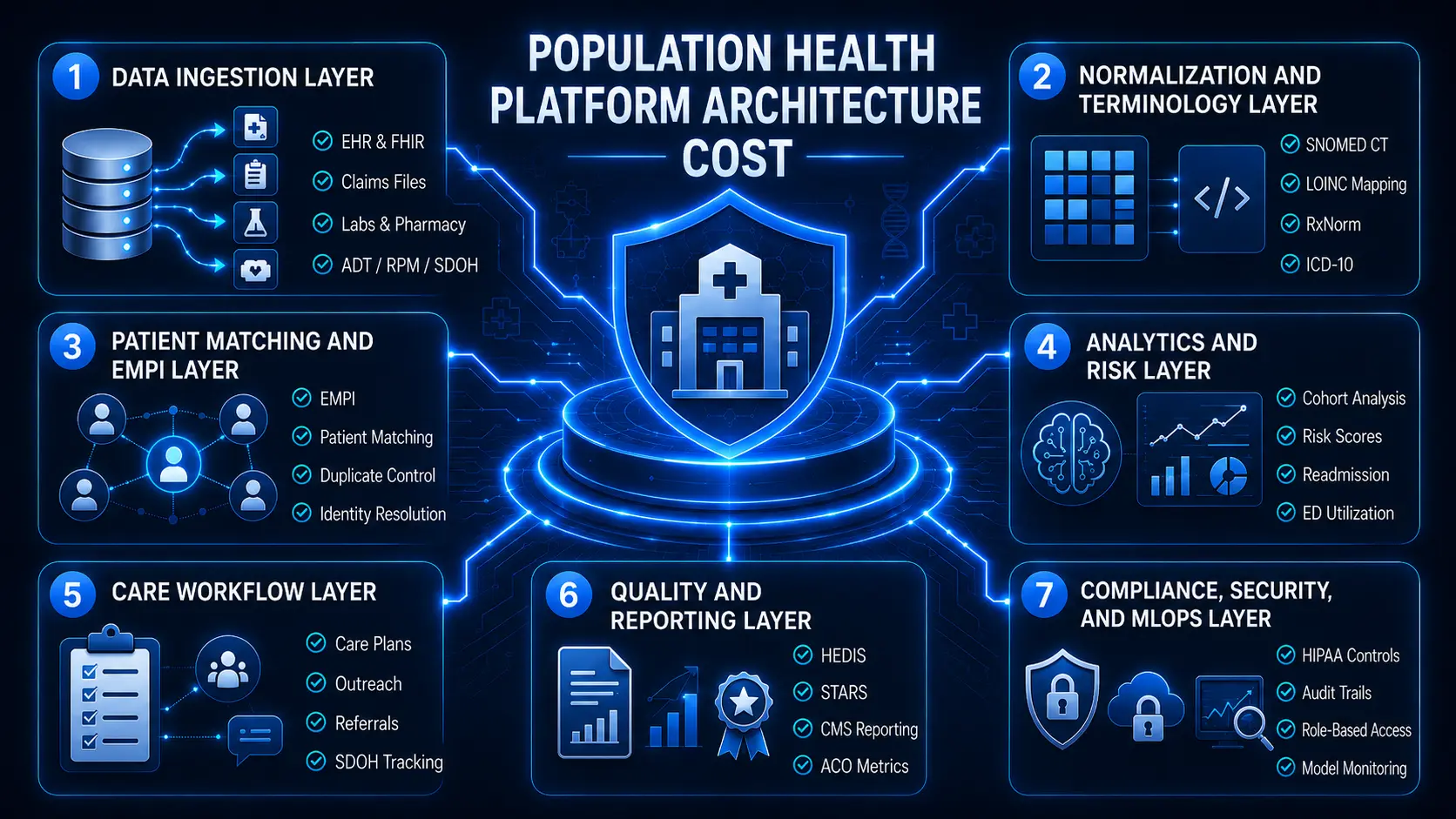
Layer 1 — Data Ingestion Layer
The data ingestion layer usually costs $18,000–$95,000 because it connects EHRs, claims files, lab data, pharmacy feeds, ADT messages, SDOH sources, RPM tools, and patient-generated health data. This layer determines whether downstream analytics, reporting, and AI models can use complete patient context.
Engineering this layer requires setting up real-time HL7 v2 feed listener ports alongside modern FHIR R4 APIs query structures to fetch clinical markers. Simultaneously, developers construct batched processing pipelines for incoming insurance claims files and member eligibility feeds to unify utilization history.
- Ancillary Connections: Engineers patch in dedicated routing lines for lab results and pharmacy data.
- Operational Streams: Live tracking requires active integration with hospital network ADT feeds.
- Modern Ingestion: High-volume arrays handle streaming data from consumer wearables and specialized RPM data hubs.
These technical data sets are then combined with contextual SDOH sources to flag environmental vulnerabilities. Once the data enters the platform, the next layer must make it usable.
Layer 2 — Normalization and Terminology Layer
The normalization layer usually costs $12,000–$45,000 because raw healthcare data arrives with inconsistent codes, labels, formats, and missing values. The platform must standardize SNOMED CT, LOINC, RxNorm, ICD-10, labs, medications, diagnoses, procedures, and encounter types before analytics can be trusted.
This environment addresses your core data quality management population health cost profile by enforcing automated clinical data normalization cost controls. Software engineers build a robust terminology mapping cost population health subsystem to handle disparate facility files.
- Clinical Standards: The mapping architecture routes codes through an integrated SNOMED CT mapping cost table.
- Diagnostic Mapping: Laboratory outputs are cross-referenced using a customized LOINC mapping population health cost grid.
- Prescription Codes: Pharmaceutical descriptions undergo real-time matching via a verified RxNorm integration cost layer.
Mismatched documentation is quickly translated using an active ICD-10 coding population health cost validation script. After normalization, the platform must know which records belong to the same person.
Layer 3 — Patient Matching and EMPI Layer
The patient matching and EMPI layer usually costs $12,000–$55,000. This layer links records across EHR, claims, lab, pharmacy, ADT, and outreach systems. It also detects duplicates, manages weak identifiers, and reduces the risk of care gaps appearing under the wrong patient.
Building this component requires a dedicated master patient index cost population health configuration. Developers deploy an advanced, multi-tiered patient matching algorithm cost block to crawl through inbound records.
- Enterprise Resolution: Complex multi-facility networks require a true enterprise master patient index EMPI cost system.
- Deduplication Queues: The engine automatically drives down costs by running background duplicate record management cost protocols.
- Quality Metrics: This mechanism directly controls your overall data quality management population health cost footprint.
This approach lowers manual review queues while preventing dangerous misidentifications. Once patient identity is reliable, the analytics layer can calculate cohort and risk views.
Layer 4 — Analytics and Risk Layer
The analytics and risk layer usually costs $15,000–$85,000. It includes dashboards, cohort analysis, risk tiering, predictive risk scoring, care gap logic, chronic disease models, readmission prediction, ED utilization prediction, and rising risk identification for care teams and value-based care leaders.
The consumer layer delivers a specialized population health analytics dashboard cost footprint for care executives. Engineers assemble a live quality performance dashboard cost layout to track multi-facility compliance.
- Segmentation Frameworks: Care cohorts are broken down using custom-built cohort analysis tools cost engines.
- Visual Stratification: Risk levels are populated across a distinct stratification dashboard cost interface.
- Financial Reporting: This engine aggregates processing numbers under a standard reporting and analytics cost population health structure.
The intelligence engine runs an automated risk stratification model cost routine. This pipeline surfaces acute trends using a custom predictive risk scoring cost matrix. Analytics creates visibility. However, the next layer turns that visibility into operational work.
Layer 5 — Care Workflow Layer
The care workflow layer usually costs $20,000–$85,000 because it turns population insights into assigned care tasks. This includes care plan automation, care coordination, referral management, patient outreach automation, SDOH intervention tracking, patient communication automation, and care team collaboration.
This environment underwrites your baseline care management workflow cost metrics. The application layer features an active care coordination platform cost interface to connect field nurses with clinic physicians.
- Task Automation: Care paths update dynamically using an integrated care plan automation cost system.
- External Transitions: Providers handle network tracking via a dedicated referral management cost population health engine.
- Social Care: Staff manage community placements through a dedicated community resource referral cost block.
This data feeds an automated SDOH intervention tracking cost dashboard. Specialized community health worker features cost templates keep mobile teams connected to the core system. Once care teams act, the platform must report the results.
Layer 6 — Quality and Reporting Layer
The quality reporting layer usually costs $15,000–$75,000 because it must calculate care gaps, measure denominators, exclusions, numerator movement, contract performance, and audit-ready reporting. This layer supports HEDIS, STARS, CMS quality programs, ACO reporting, and value-based care reporting.
The system continuously scans patient data to compute your real-time quality measure gap cost parameters. Developers integrate a specialized HEDIS measure automation cost engine to track preventative screening compliance.
- Payer Metrics: Medicare Advantage teams monitor contract positions using a STARS measure tracking cost routine.
- Federal Compliance: The core logic satisfies standard CMS quality program cost reporting demands.
- Risk Contracts: Shared-savings groups calculate performance metrics through an explicit ACO reporting cost engine.
This engine consolidates outcomes under a standard value-based care reporting cost framework. It manages long-term compliance through a regulatory reporting cost population health layer and a CMS reporting cost population health sub-routine. These engines are essential for teams preparing for NCQA accreditation cost benchmarks or formal URAC accreditation cost reviews.
Reporting uses sensitive data, so compliance must protect every layer.
Layer 7 — Compliance, Security, and MLOps Layer
The compliance, security, and MLOps layer usually costs $12,000–$60,000 in a focused build. It covers PHI security, encryption, role-based access, audit trails, BAA requirements, cloud controls, model drift monitoring, model retraining, and secure release management.
This core foundation covers your primary HIPAA compliance population health requirements. The infrastructure layer isolates patient logs using strict PHI security population health platform access frameworks.
- Legal Foundations: Hosting setups conform directly to institutional BAA requirements for population health.
- Data Protection: The framework applies a universal data encryption population health cost standard for files at rest and in transit.
- Access Control: Engineers build specific role-based access population health cost matrices across all database tables.
The platform secures network perimeters using a strict zero-trust architecture population health strategy. It maintains an unalterable audit trail population health cost database to track data viewing habits. This foundation supports your long-term SOC 2 compliance cost population health auditing and baseline HITRUST certification cost pathways.
All components run on a scalable cloud infrastructure cost population health layer, balancing your long-term scalability cost population health platform constraints. Finally, predictive safety is maintained via a functional MLOps pipeline cost population health engine.
A population health architecture is only as strong as its weakest layer. Therefore, investing heavily in analytics while ignoring your normalization and identity layers will result in flawed risk scores and untrusted clinical reports.
AI-Powered Population Health Platform Development Cost
Adding AI models into the population health platform cost usually adds $18,000–$85,000 inside a focused $70,000–$450,000 build. The cost depends on whether the platform uses rules-based stratification, one predictive model, or multiple monitored models for readmission, ED utilization, chronic disease risk, and rising risk identification.
The sophistication of your analytical layer should scale in lockstep with your clinical data quality. Consequently, deploying advanced algorithms on unnormalized data sources will lead to skewed risk scoring and lost care team trust.
- Logic Alignment: Simple structural filtering allows rapid rollout for early incentive contracts.
- Predictive Operations: True machine learning pipelines require explicit infrastructure for feature management and deployment validation.
1. Rules-Based Risk Stratification
Rules-based risk stratification usually costs $10,000–$25,000. It uses clinical criteria, claims history, diagnosis codes, lab thresholds, medication patterns, care gaps, and utilization triggers to group patients into low, rising, and high-risk cohorts without training a full predictive model.
- Logic Filters: This system uses precise chronic disease criteria alongside standard diagnosis code rules to map known disease profiles.
- Clinical Bounds: The engine applies specific lab threshold rules and matching medication rules to capture patient severity.
- Operational Flags: Code structures track active care gap flags combined with historical utilization thresholds.
The pipeline routes these metrics through defined provider or payer rules, generating static patient lists. Furthermore, developers incorporate explicit manual review support features so clinical leads can adjust risk assignments inside their dashboards.
2. Predictive Risk Scoring Model
A predictive risk scoring model usually costs $18,000–$45,000 for one defined use case. It can estimate readmission risk, ED utilization risk, chronic disease escalation, or rising-risk patients using clinical, claims, utilization, medication, lab, and demographic signals.
- Pipeline Code: The development phase covers deep feature engineering routines to convert messy clinical timestamps into mathematical inputs.
- Mathematical Training: Data scientists execute formal model training loops utilizing cleanly labeled historical labels.
- Model Validation: Algorithms go through strict train-test validation passes to verify statistical accuracy across distinct patient cohorts.
The system calculates clear SHAP explainability vectors so clinicians can see exactly which factors drove an individual score. Engineers run dedicated bias checks to protect marginalized groups, establish precise risk threshold design parameters, and build a dedicated monitoring dashboard for care managers.
Some teams need more than one model, but that increases the budget.
3. Multi-Model Population Risk Layer
A multi-model population risk layer usually costs $45,000–$85,000. This tier may combine readmission prediction, ED utilization prediction, chronic disease risk, rising risk identification, and outreach prioritization. It also requires stronger validation, monitoring, retraining, and model governance.
The system runs concurrent clinical predictions, managing your foundational readmission prediction model cost footprint alongside an ED utilization prediction cost system. This intelligence tier layers a specialized chronic disease risk model cost block next to a real-time rising risk identification cost routine.
- Operational Sorting: The outputs feed an automated patient outreach prioritization queue for field nurses.
- Performance Safety: To combat accuracy loss, the budget funds a model drift monitoring cost population health loop.
- Data Lifecycle: System scripts handle scheduled model retraining cost population health processes using fresh data enclaves.
- Production Core: This loop is managed by a dedicated healthcare MLOps pipeline cost population health framework.
AI is an operational optimization tool, not financial magic. So, start with transparent rules-based logic to align your care teams, and introduce predictive machine learning models only when your data pipeline achieves stable normalization.
The Intervention Attribution Ledger No One Budgets For
The intervention attribution ledger tracks if an automated risk alert actually led to patient outreach. It monitors if that outreach caused a clinical action, if the action closed a gap in care, and if that change improved your value-based contract payouts.
Most software discussions focus entirely on visual dashboards, AI tools, or basic patient portals. However, they rarely show how to prove that your platform caused a positive clinical change.
Without this ledger, your team cannot prove that your software was responsible for lower hospital readmissions. Consequently, building this tracking layer removes the historical guesswork from value-based care contracts.
1. What The Attribution Ledger Tracks
An intervention attribution ledger tracks the entire path from finding a patient risk to proving a financial outcome. It connects the initial data alert to the staff member who handled the outreach and records the patient’s actual response.
- Step One: The system assigns a unique risk signal ID to a specific patient and logs their clinical patient cohort.
- Step Two: It tracks the exact care gap type and names the assigned care team member responsible for making the call.
The database records the precise outreach timestamp and notes if the team used an email, text, or phone call. It then saves the patient response and records any necessary care plan update markers in the database.
- Field Action: The ledger tracks if the patient finished their referral completion step or needed a specific SDOH intervention.
- Final Results: Finally, these records link directly to positive quality measure movement and final insurance claims outcome updates.
2. What It Costs To Build
An intervention attribution ledger usually costs $18,000–$60,000 inside a custom population health platform. The total cost depends on how many systems you track, how deep your timestamps go, and the complexity of your payer contracts.
- Database Setup: Software engineers build a custom database event schema to act as a secure, fast data ledger.
- Activity Logging: The system compiles a continuous workflow activity log to connect daily clinical tasks with final insurance data.
The backend maintains an unalterable audit trail to back up your regional measure linkage reports. Furthermore, developers write simple contract logic to compare platform costs against your actual shared-savings financial returns.
- Staff Metrics: This tracking tool calculates care manager productivity to show how efficiently your teams work.
- Executive View: The system converts patient-level evidence and provider-level evidence into a clear, visual ROI dashboard for your financial team.
3. Why It Helps Secure Capital Approval
This ledger helps secure capital approval because it connects software spending directly to saved dollars. CFOs see lower hospital costs, quality teams see better metric scores, and CTOs get a clear, audit-ready data trail.
- Clear Value: It transforms your software from a general administrative cost into an active tool that drives financial revenue.
- Incentive Tracking: By connecting early patient outreach to final contract bonuses, the ledger proves the platform pays for itself.
Once the attribution layer is defined, leaders can compare build vs buy decisions more clearly.
If you do not build an attribution ledger, you cannot prove whether your platform closed care gaps or if it happened by accident. At the same time, true financial success in value-based care requires tracking the direct link between clinical insights and contract returns.
Build Vs Buy Population Health Platform Cost
Build vs buy population health platform cost should be decided by data control, workflow fit, reporting flexibility, AI model ownership, and long-term TCO. Here, buying is faster when needs are standard.
At the same time, building makes sense when the organization needs custom integration, proprietary risk logic, contract-specific reporting, and measurable workflow attribution.
The long-term total cost of ownership (TCO) changes dramatically based on how many distinct data layers your business operates. Consequently, choosing a standard pre-built platform without reviewing your custom engineering needs can lead to expensive vendor lock-in or integration roadblocks.
1. Build vs Buy
| Decision Factor | Buy PHM Software | Build Custom PHM Platform |
| First-Year Cost | Subscription and implementation fees | $70,000–$450,000 focused build |
| Launch Speed | Faster deployment | Slower but more controlled |
| Data Ownership | Vendor-defined limits | Organization-defined storage |
| Workflow Flexibility | Configuration limits | Custom care workflows |
| AI Model Control | Limited pre-built algorithms | Full model governance |
| Reporting Logic | Vendor roadmap dependent | Contract-specific setup |
| Interoperability | Vendor-supported connections | Built around exact systems |
| Best Fit | Standard PHM needs | Complex ACO, payer, or IDN workflows |
2. When Buying Makes More Sense
Buying makes more sense when the organization needs standard population health management software cost predictability, fast deployment, basic dashboards, standard care gap workflows, and limited customization. It also works when the team lacks engineering support or does not need proprietary AI models.
- Simple Setup: This model fits operations that use a single EHR environment with no messy outside fields.
- Basic Communication: Your daily teams only require standard patient outreach paths like manual calls.
The care team can track basic metrics without running complex, contract-specific reporting models across multiple groups. Furthermore, buying off-the-shelf tools works well when you do not have any custom EMPI needs or specialized identity match queues.
3. When Building Makes More Sense
Building makes more sense when the organization needs control over data, workflows, AI models, quality reporting, and intervention evidence. A custom build is stronger when population health performance depends on proprietary contract logic, multi-source integration, specialized cohorts, or value-based care platform development cost control.
- Data Silos: Custom builds handle incoming information across entirely separate, multiple EHRs simultaneously.
- Unified History: The pipeline continuously merges claims plus clinical data sets into one longitudinal view.
This custom layer accurately maps performance metrics directly into complex federal ACO reporting frameworks. It also deploys specialized Medicaid managed care workflows tailored for highly specific local demographics.
4. When A Hybrid Model Works Best
A hybrid model works best when the organization wants to buy commodity features but build differentiated infrastructure. For example, a team may buy messaging or CRM tools while building its own data layer, risk scoring engine, reporting logic, and attribution ledger.
- Outsource Channels: Your team can buy patient messaging APIs from standard communication vendors.
- Staff Tracking: You can easily buy a CRM module to handle basic phone scheduling logs.
This allows your internal engineering team to focus solely on building high-value data ingestion pipelines. Engineers write custom code to deploy an internal EMPI system and build tailored risk models for your exact chronic cohorts.
The build decision should not start with software demos. It should start with the parts of population health performance your organization must control. If your revenue depends on a unique care workflow or a proprietary risk scoring model, building your own system is the only way to protect that logic.
How To Build A Population Health Platform Within $70,000–$450,000
To build a population health platform within $70,000–$450,000, the project must move through distinct, controlled phases. Each step should release only the capabilities needed for immediate clinical or financial value.
A modular rollout schedule prevents engineering teams from trying to build too much at once. Consequently, completing phase-by-phase goals ensures early financial returns while keeping total infrastructure costs under control.
Population Health Platform Development Table
| Implementation Phase | Cost Range | Engineering Deliverable | Primary Operational Outcome |
| Discovery & Baselines | $5,000–$18,000 | Data source inventory, contract mapping, metric baselines | Prevents scope creep; defines care gap closure ROI goals |
| Data Ingestion Pipeline | $18,000–$95,000 | EHR integration, HL7 v2 feeds, FHIR APIs, claims files | Establishes the secure data landing zone for multi-source files |
| Deduplication & Matching | $12,000–$55,000 | Clinical data normalization, SNOMED CT mapping, EMPI logic | Fixes poor-quality records; tracks data lineage accurately |
| Analytics & Dashboards | $15,000–$70,000 | Cohort analysis tools, stratification dashboard | Shows care teams which patients need immediate action and why |
| AI Risk Scoring Engine | $18,000–$85,000 | Feature engineering, model training, predictive risk scoring | Prioritizes outreach lists using automated predictive models |
| Care Workflow System | $20,000–$85,000 | Care plan templates, patient outreach automation | Turns data insights into assigned, trackable staff actions |
| Quality & Value Reporting | $15,000–$75,000 | HEDIS measure automation, CMS reporting tools | Reduces manual audit work; calculates contract performance |
| Security & Launch | $20,000–$95,000 | PHI security, role-based access, encryption, UAT cycles | Delivers a fully compliant, production-ready system to users |
To execute this roadmap efficiently, Intellivon maps out all data connections and schema requirements before writing any code. We prioritize the two or three primary data sources needed for immediate workflow accuracy, saving high-frequency streaming tools for later updates.
- Logic Isolation: We build your measure logic and risk criteria as configurable rules rather than hard-coded scripts.
- Rework Prevention: Designing your security matrices and audit logs during the initial database layout avoids expensive compliance rewrites later.
Building a platform within this budget requires strict phase control. Do not try to integrate every data source or train five different AI models in your first release. Focus on setting up clean ingestion, reliable patient matching, and one active care workflow to prove financial value first.
Population Health Platform Total Cost Of Ownership
Population health platform total cost of ownership includes the initial $70,000–$450,000 build plus annual maintenance at 15%–25% of initial development cost. Maintenance covers integration support, reporting updates, model monitoring, security patches, cloud infrastructure, user feedback, and workflow improvements.
Calculating long-term operational costs prevents unexpected budget shortfalls after your system goes live. Consequently, evaluating these annual expenditure zones keeps your data layer scalable as patient populations and value-based contracts expand.
1. TCO of Population Health Platform
| Initial Build Cost | Estimated Annual Maintenance | What Maintenance Covers |
| $70,000 | $10,500–$17,500 | Basic support, small reporting updates, limited integration monitoring |
| $120,000 | $18,000–$30,000 | Data feed monitoring, dashboard updates, security patches |
| $250,000 | $37,500–$62,500 | Integration support, workflow updates, measure changes, model checks |
| $450,000 | $67,500–$112,500 | Multi-source support, model monitoring, reporting changes, release management |
2. Cloud Infrastructure Cost Population Health
Hosting a secure health platform requires budgeting between $500–$5,000 per month for smaller workloads. However, these infrastructure costs scale significantly higher as your system absorbs larger data volumes from across your medical network.
- Resource Allocation: The base budget covers essential cloud storage, compute processing power, system logging, automated backups, and performance monitoring tools.
- Compliance Design: Your hosting setup must use dedicated, highly secure environments to isolate protected health information safely.
Engineers must also configure strict data retention rules to manage long-term database expansion efficiently. At Intellivon, we use automated resource scaling to optimize cloud compute tasks, ensuring you only pay for heavy processing power when syncing massive data batches.
3. Reporting Maintenance Cost
Quality metric tracking requires continuous code updates because national measurement definitions change every single calendar year. Your annual maintenance budget must fund technical updates for HEDIS updates, STARS changes, CMS reporting updates, and ACO reporting changes.
- Logic Adaptability: Developers must constantly adjust the underlying database queries to align with fresh payer-specific logic.
- Audit Readiness: The reporting engine needs regular optimization to keep your automated audit export updates fully compliant during federal reviews.
Failing to update these calculation engines leads to inaccurate care gap tracking, which directly hurts your value-based contract performance.
4. AI Maintenance Cost
Machine learning models lose accuracy over time as clinical behaviors, demographic profiles, and charting habits shift. Consequently, teams must fund continuous model drift monitoring routines to verify that risk predictions remain clinically valid.
- Model Optimization: Your data science budget covers scheduled model retraining loops, feature updates, and precise risk threshold calibration work.
- Safety Controls: Engineers conduct routine explainability checks and formal bias review sessions to protect patient care decisions.
These ongoing validation processes ensure that your care managers can continue to trust automated risk scores for outreach prioritization.
5. Integration Maintenance Cost
External medical interfaces are highly unstable because hospitals constantly update their internal software configurations. Maintaining data accuracy requires continuous monitoring of your live EHR interface changes and unexpected claims format updates.
- Feed Management: Engineers must supervise ongoing lab feed changes, pharmacy file updates, and live ADT feed monitoring lines.
- Data Resolution: The development team manages technical error queues to capture and repair rejected records before they drop out of the system.
Budgeting for dedicated interface support ensures your downstream clinical dashboards never display outdated or missing patient records.
The first build is only the start of the budget. Population health platforms need maintenance because data feeds, measures, contracts, care teams, and risk logic keep changing. Therefore, plan for a 15%–25% annual operational budget to protect your initial engineering investment.
Population Health Platform ROI
Population health platform ROI comes from measurable care action, not dashboards alone. At the same time, leaders should connect the platform to readmission reduction ROI, ED utilization reduction ROI, care gap closure ROI, quality measure improvement ROI, and value-based contract performance ROI before approving the build.
A custom data framework transitions your software from an administrative expense into an active revenue generator. Consequently, connecting your data layer to trackable clinician actions allows you to claim shared-savings incentives and protect your upfront software investment.
1. ROI of the Platform
| Financial Benefit Area | Lower-Performing Systems | Higher-Performing Systems | Expected Shared-Savings ROI |
| Care Gap Closures | Manual chart chasing and late outreach lines | Real-time EHR data prompts at the point of care | Increases incentive revenue by 12%–18% |
| Utilization Costs | Passive tracking after hospital discharge occurs | Predictive risk modeling with automated SMS alerts | Cuts avoidable admission costs by 15%–22% |
| Quality Reporting | Hard-coded registry uploads compiled at year-end | Modular, rule-based clinical data calculation | Secures top-tier performance bonus payouts |
2. ROI From Care Gap Closure
Closing gaps in care directly triggers bonus payouts across all alternative payment models. At the same time, relying on automated tracking software helps teams surface outstanding preventive screenings before your annual contract deadlines close.
- Chronic Condition Tracking: The system monitors real-time diabetes measures and logs hypertension follow-up records.
- Adherence Management: Active data tools evaluate daily medication adherence scores using pharmacy claims data.
The application automatically schedules required annual wellness visits for your rising-risk patient cohorts. Closing these care opportunities before formal reporting deadlines prevents your business from missing out on substantial tier-level quality adjustments.
3. ROI From Utilization Reduction
Unmanaged emergency department use rapidly destroys shared-savings margins inside upside and downside risk models. Therefore, deploying custom software underwrites your baseline ED utilization reduction ROI by alerting staff before acute events scale.
- Acute Inpatient Mitigation: The predictive infrastructure manages your broader readmission reduction ROI goals.
- Targeted Outreach: The engine populates immediate lists for high-risk cohort outreach tasks.
Care coordinators access automated workflows to manage care transition follow-up paths right after hospital discharge. This immediate response reduces expensive avoidable admissions and optimizes patient care pathways during the critical 30-day post-discharge window.
4. ROI From Quality Measure Improvement
Modern insurance contracts tie performance bonuses directly to digitized quality metrics. Therefore, building a modular data schema drives your macro-level HEDIS movement and protects your long-term STARS improvement positions.
- Federal Payouts: The backend architecture supports high-scoring CMS quality program performance reviews.
- Registry Automation: Configurable rules seamlessly calculate complex ACO reporting parameters across all facilities.
The interface converts messy billing fields into clean provider performance analytics scorecards. Consequently, these clear dashboards encourage friendly internal competition while maximizing your network’s overall contract bonus potential.
5. ROI From Cost-Of-Care Management
Enterprise software controls risk by giving leaders total visibility into total healthcare spending. Thus, running active cost of care analytics cost models surfaces expensive treatment variations across your provider network.
- Actuarial Guardrails: The analytics environment includes continuous total cost of care modeling logic.
- Resource Allocation: Clinical directors leverage a modern utilization management cost population health block.
The compliance layer runs an automated network adequacy analysis cost matrix to spot referral leakage patterns early. By identifying provider performance variation, the platform stops patients from wandering out-of-network for expensive specialty services.
ROI appears when the platform changes behavior. If risk scores do not trigger outreach, referrals, medication review, or follow-up, the platform becomes an expensive reporting layer. Focus your initial build on the specific care gaps and utilization metrics that carry the highest financial weights in your contracts.
Build An Enterprise Population Health Platform With Intellivon
A population health platform budget should not start with a generic software quote. It should start with your data sources, EHR environment, claims feeds, patient populations, quality measures, care workflows, AI model needs, HIPAA controls, and rollout plan.
Intellivon helps healthcare organizations turn those requirements into a practical $70,000–$450,000 build roadmap.
1. Define The Right First Release
The first release should prove operational value before the platform expands. Intellivon helps teams identify which population, contract, care gap, or utilization problem should shape the MVP. This keeps the build focused on measurable outcomes instead of adding too many dashboards, integrations, or AI models too early.
For example, the first release may focus on diabetic care gap closure, readmission risk, ED utilization reduction, Medicaid outreach, or ACO quality reporting. Each use case requires a different mix of data ingestion, patient matching, workflow automation, and reporting logic.
2. Map Your Data And Integration Scope
Population health cost depends heavily on how much data the platform must connect and clean. Intellivon maps your EHR systems, claims files, lab feeds, pharmacy data, ADT feeds, SDOH data, RPM tools, patient portal data, and reporting exports before development starts.
This helps your team understand whether the first build should use simple file ingestion, FHIR APIs, HL7 v2 feeds, claims integration, or a more advanced data pipeline. It also gives leadership a clearer view of what can fit inside a $70,000–$120,000 MVP, a $120,000–$250,000 controlled build, or a $250,000–$450,000 production release.
3. Design The Architecture Before Writing Code
A population health platform needs more than dashboards. It needs a reliable architecture for data ingestion, clinical data normalization, patient matching, cohort analysis, risk scoring, care gap tracking, quality reporting, audit trails, and access control.
Intellivon designs this foundation before engineering begins. This prevents costly rework later, especially when teams add new EHRs, new contracts, new quality measures, or new care management workflows after launch.
4. Build AI Around Real Care Actions
AI should not sit inside the platform as a disconnected prediction feature. Intellivon helps teams decide where AI can support real operational decisions, such as outreach priority, readmission risk, ED utilization risk, chronic disease escalation, or rising-risk identification.
Each model is planned with clear inputs, thresholds, review workflows, monitoring needs, and human oversight. This makes the AI layer easier to trust because every score connects to a specific care action.
5. Include Compliance And Maintenance Planning Early
HIPAA controls, PHI security, role-based access, audit trails, encryption, BAA requirements, and secure deployment should not be added at the end. Intellivon includes compliance planning during architecture so the platform can move safely from pilot to production.
The team also helps plan ongoing maintenance. This includes interface monitoring, model drift checks, quality measure updates, reporting changes, security patches, cloud support, and workflow improvements after launch.
What You Can Build With Intellivon
With Intellivon, healthcare teams can build a focused population health platform that supports:
- Clinical and claims data ingestion
- EHR, HL7, FHIR, lab, pharmacy, ADT, and SDOH integration
- Patient matching and duplicate record management
- Cohort dashboards and care gap tracking
- Risk stratification and predictive risk scoring
- Care management workflows and patient outreach
- HEDIS, STARS, CMS, ACO, and value-based care reporting
- HIPAA-ready access controls, audit trails, and PHI security
- Deployment, monitoring, and long-term maintenance planning
Intellivon can help you turn your platform idea into a clear development plan before you commit budget. The team can map your integrations, workflows, AI model scope, quality reporting needs, compliance controls, and rollout phases into a realistic $70,000–$450,000 cost estimate.
Build your population health platform cost plan with Intellivon.
Conclusion
Population health platform cost should be planned as phased infrastructure, not a single software line item. Instead, leaders should fund the data foundation, patient matching, AI models, care workflows, quality reporting, HIPAA controls, and deployment in sequence.
Therefore, the strongest first release focuses on trusted data, priority patients, care action, and measurable value. As the platform proves impact, teams can expand integrations, automation, and reporting with less financial risk later.
Things To Know About Population Health Platform Cost
Q1.How much does a population health platform cost to build?
A1. Population health platform cost usually ranges from $70,000–$450,000 for a focused enterprise build. A lean MVP costs $70,000–$120,000. However, a production-ready platform with EHR integration, claims data, risk scoring, workflows, reporting, and HIPAA controls costs $250,000–$450,000.
Q2. What is the enterprise population health software development cost for an MVP?
A2. Enterprise population health software development cost for an MVP usually ranges from $70,000–$120,000. This covers basic data ingestion, cohort dashboards, care gap tracking, simple outreach workflows, role-based access, and HIPAA-ready controls. Therefore, it works best for one defined population or contract.
Q3. What is the population health management platform build cost for production?
A3. Population health management platform build cost for production usually ranges from $250,000–$450,000. This version includes deeper EHR integration, claims ingestion, patient matching, AI risk models, care workflows, HEDIS or CMS reporting, audit trails, and maintenance planning. As a result, it supports real enterprise use.
Q4. What is the population health analytics platform cost?
A4. Population health analytics platform cost usually ranges from $70,000–$180,000. This budget covers dashboards, cohort views, stratification, care gaps, utilization reports, and basic quality reporting. However, costs increase when analytics must combine EHR, claims, SDOH, pharmacy, lab, and ADT data.
Q5. What does a HIPAA-compliant population health platform cost?
A5. A HIPAA-compliant population health platform usually adds $12,000–$60,000 to a focused build. This covers PHI security, encryption, role-based access, audit trails, BAA requirements, secure cloud setup, access monitoring, and compliance documentation. Therefore, compliance should be planned before development starts.
Q6. How long does population health platform development take?
A6. A lean MVP usually takes 10–14 weeks. Meanwhile, a controlled enterprise MVP takes 14–22 weeks. Therefore, a production-ready platform with EHR integration, claims data, AI models, care workflows, reporting, and HIPAA controls usually takes 5–8 months.
To Sum Up:
- A $70,000–$120,000 MVP can prove population health value when it focuses on one population, one workflow, and a small number of trusted data sources.
- The highest-cost part of a focused platform is the data foundation that makes care gaps, risk scores, and reports trustworthy.
- AI risk scoring only creates ROI when it changes care team action. A score without workflow ownership is just another dashboard metric.
- The missing layer in most population health platforms is intervention attribution. Leaders need to prove which care actions changed quality, utilization, or contract performance.
- Annual maintenance should be planned at 15%–25% of the initial build because integrations, measures, models, and contracts change after launch.



