

Cardiology sits at the intersection of volume, risk, and time sensitivity. As cardiovascular cases increase and specialist availability decreases, organizations need to rethink how they provide cardiac care beyond physical locations. Tele-cardiology has evolved from being an option to becoming an essential clinical capability.
White-label tele-cardiology platforms change this situation. Instead of using separate SaaS tools, organizations gain control over cardiac workflows, data intelligence, and patient engagement. Platforms like Auxira show what is possible when remote cardiac workflows, secure data pipelines, and specialist access are brought together as a unified system. However, many healthcare organizations still depend on fragmented tools that were not designed to work at a large scale or under ongoing clinical demands.
At Intellivon, we have spent over a decade creating healthcare platforms that can handle real clinical volumes and meet strict compliance standards. Based on this experience, we are using this blog to explain how to build a white-label tele-cardiology platform like Auxira from scratch.

Why Health Systems Need a White-Label Tele-Cardiology Platform in 2025
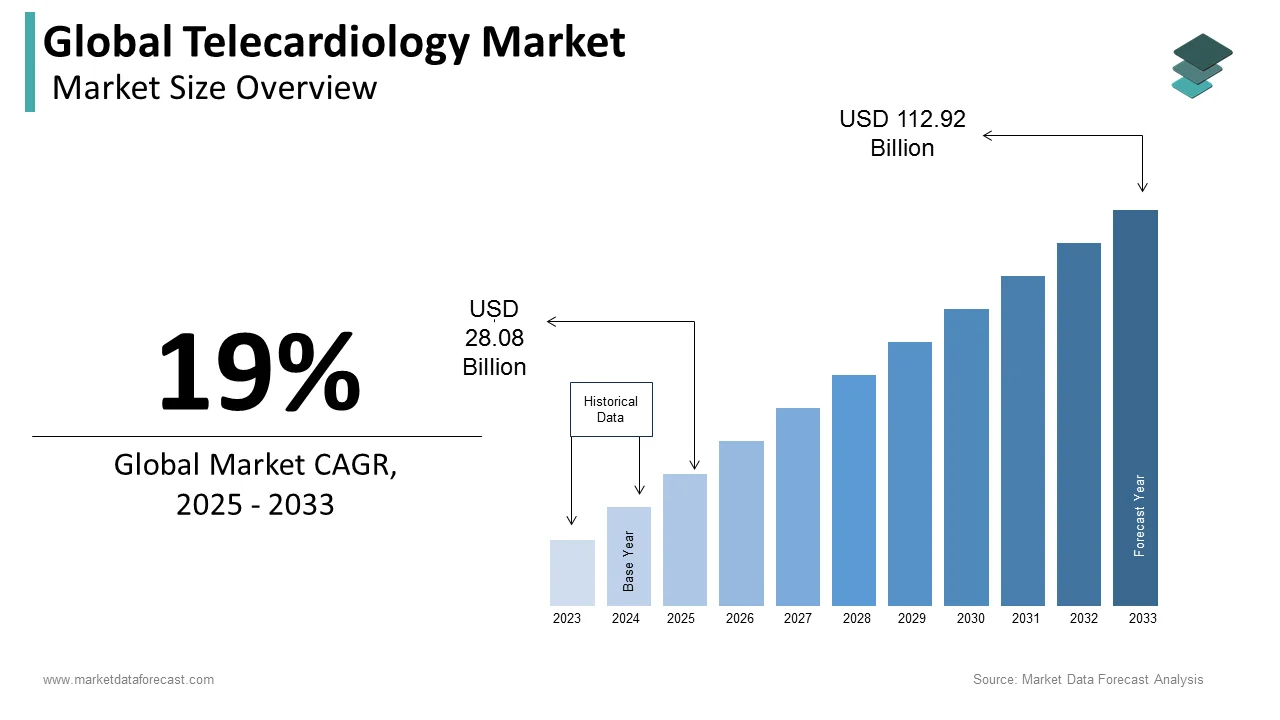
Industry forecasts show tele-cardiology moving into a strong growth phase. Market value is expected to rise from the low-to-mid-teens (USD billions) in the mid-2020s to anywhere between roughly USD 40 billion and well over USD 100 billion by the early-to-mid 2030s, reflecting sustained annual growth in the high-teens.
This expansion is being fueled by rising demand for remote cardiac care, specialist shortages, and accelerated adoption of digital health platforms across enterprise healthcare systems.
Market Drivers:
- Telecardiology within telemedicine is one of the fastest-growing application segments, with telecardiology telemedicine expected to grow at around 18.8% CAGR from 2024 to 2030.
- Cardiovascular disease remains the leading global killer; projections show a 90% increase in CVD prevalence and cardiovascular deaths, rising from 20.5 million in 2025 to 35.6 million by 2050.
- In the US, cardiovascular diseases account for roughly 40% of CVD-related deaths and around 11% of total health expenditures, underscoring the budget impact of cardiac care.
Clinical benefits: Chronic Cardiac Care and Outcomes
- Projections suggest cardiovascular prevalence will rise 90% by 2050, even as age-standardized mortality falls.
- Remote patient monitoring is now a dominant telecardiology service segment because it delivers continuous, real-time measurements for cardiac patients.
- RPM and telecardiology support proactive management of post-MI and heart failure patients by capturing subtle vital-sign deviations.
- Studies and RPM case reports show that continuous monitoring combined with structured follow-ups can reduce readmissions.
- Patients using RPM for chronic diseases such as hypertension and heart failure report higher engagement and satisfaction.
Revenue and ROI Levers: Reimbursement and Cost Efficiencies
- Within telemedicine, telecardiology and RPM services are emerging as high-value segments, as payers increasingly reimburse for remote monitoring and virtual visits to manage costly chronic cardiac conditions.
- Medicare and many private insurers now reimburse for RPM, with specific CPT codes and monthly fees for device supply, data interpretation, and care management, creating predictable recurring revenue streams for cardiology practices.
- The FCC estimated that widespread RPM adoption could save the healthcare system up to 700 billion USD over 15–20 years, via reduced readmissions, shorter hospital stays, and lower operational costs.
- Telecardiology and RPM programs also help reduce avoidable readmission penalties and improve quality metrics tied to value-based contracts, further strengthening ROI beyond direct reimbursement.
- White-label telecardiology platforms avoid the capital expense and time risk of building greenfield systems, letting health systems redirect capital toward scaling RPM devices.
What Is The White-Label Tele-Cardiology System Auxira?
Auxira is a white-label tele-cardiology system that enables enterprises to deliver branded remote cardiac care by integrating ECG interpretation, tele-echo, specialist workflows, and EHR-connected clinical governance into one scalable platform.
The platform enables remote ECG interpretation, tele-echo review, and cardiology consultations across hospitals, clinics, and emergency settings. It integrates with EHRs, cardiac devices, and clinical workflows so cardiac decisions move directly into existing care pathways without disruption.
From an enterprise standpoint, Auxira provides operational ownership. Organizations retain control over data, workflows, branding, and clinical governance while scaling cardiology services across regions. This model supports faster response times, better specialist utilization, and consistent cardiac care delivery without increasing on-site cardiology staffing.
What Is a White-Label Tele-Cardiology System?
A white-label tele-cardiology system is a customizable remote cardiac care platform that enterprises brand and integrate into EHR, billing, and scheduling systems to deliver governed cardiology workflows at scale.
How Tele-Cardiology Differs From Generic Telemedicine
Generic telemedicine platforms are designed for broad virtual care use cases. Tele-cardiology systems, by contrast, are built around cardiac-specific data, decision timelines, and specialist workflows.
The difference becomes clear when comparing how each platform handles clinical complexity.
| Area | Generic Telemedicine Platforms | White-Label Tele-Cardiology Systems |
| Clinical Focus | General consultations across specialties | Cardiology-specific diagnosis and monitoring |
| Data Types | Video, chat, basic vitals | ECG, telemetry, echo, RPM cardiac data |
| Workflow Design | Appointment-centric | Event-driven and condition-based |
| Decision Support | Limited or rules-based | Cardiology-focused clinical logic and AI support |
| Specialist Involvement | On-demand, non-specialized | Embedded cardiologist workflows |
| Integration Depth | Surface-level EHR access | Deep EHR, device, and reporting integration |
White-label tele-cardiology systems are designed for high-risk conditions, continuous monitoring, and specialist-driven decision-making. For enterprises managing cardiac populations across facilities or regions, this distinction determines whether telehealth becomes a strategic asset or an operational bottleneck.
How Auxira’s Model Changes Cardiology Care Delivery
Auxira’s tele-cardiology model embeds virtual clinical pods into cardiology practices, enabling scalable follow-ups, low-acuity virtual visits, and inbox management without disrupting physician-led care delivery.
1. Precision-Matched Virtual Care Pods
Auxira deploys dedicated virtual “pods” made up of advanced practice providers, medical assistants, and registered nurses. These pods are aligned to specific cardiology practices, not pooled generically across systems.
Because the teams are practice-aligned, they follow the same care protocols, escalation rules, and documentation standards as the on-site staff. This preserves continuity while allowing work to shift out of the clinic setting.
2. Low-Acuity Care Moves Out of the Clinic
Routine follow-ups, medication checks, symptom reviews, and patient questions are handled through telehealth visits managed by the virtual pod. Cardiologists step in only when escalation is clinically necessary.
This approach keeps specialists focused on complex cases while ensuring patients still receive timely attention. It also shortens wait times for both virtual and in-person appointments.
3. Inbox and EHR Load Is Actively Managed
One of the most immediate impacts of Auxira’s model is inbox relief. Virtual pods take ownership of patient messages, result reviews, and non-urgent tasks inside the EHR.
In MedStar deployments, this model has been associated with reduced after-hours EHR time for cardiologists. That reduction directly affects burnout risk and long-term workforce sustainability.
4. Measured Improvements in Access and Satisfaction
Reported outcomes from Auxira and MedStar implementations include higher patient satisfaction scores and improved appointment availability across cardiology services. Patients benefit from faster responses, while practices regain scheduling flexibility.
These gains come from operational redesign rather than increased staffing, making the model economically viable at scale.
Auxira’s approach reframes tele-cardiology as a workforce and workflow strategy, not just a technology deployment. By embedding virtual care pods into cardiology practices, it expands capacity, protects specialist time, and improves patient experience.
Business and Revenue Models of Auxira
Auxira uses an enterprise-aligned business and revenue model that embeds virtual cardiology services into existing practices, enabling scalable care delivery without disrupting clinical operations or financial structures.
Business Models of Auxira
Auxira’s business model focuses on becoming an extension of the cardiology organization rather than an external service provider. This positioning allows health systems to scale virtual care while preserving internal governance and brand continuity.
1. Embedded Clinical Operations Model
Auxira integrates virtual clinical pods directly into cardiology practices. These teams operate under the same protocols, documentation standards, and escalation pathways as on-site staff.
This model ensures remote care feels operationally invisible to patients and clinicians while expanding capacity behind the scenes.
2. Practice-Aligned Deployment Model
Instead of pooled virtual staffing, Auxira aligns teams to specific practices or service lines. This preserves familiarity with patient populations, clinician preferences, and local workflows.
As a result, enterprises avoid the fragmentation commonly seen with shared telehealth resources.
3. Enterprise Integration Model
Auxira embeds its workflows within existing EHR, scheduling, and communication systems. Organizations do not need to introduce parallel platforms or retrain staff on new systems.
This lowers adoption friction and accelerates time to value.
Auxira’s business model works because it adapts to enterprise realities. By fitting into established cardiology operations, it enables scale without forcing structural change.
Revenue Models of Auxira
Auxira’s revenue structure mirrors how health systems prefer to pay for clinical capacity rather than per-interaction software usage. This alignment supports predictable financial planning.
1. Subscription-Based Service Contracts
Health systems typically engage Auxira through recurring contracts tied to service scope, volume, or practice coverage. This provides cost predictability while allowing gradual expansion.
2. Per-Provider or Per-Practice Pricing
Pricing often scales by the number of cardiologists, practices, or service lines supported. This aligns costs directly with the operational footprint rather than patient volume spikes.
3. Value-Based Enablement Model
Auxira supports quality metrics, access improvements, and clinician efficiency that contribute to value-based care performance. While not always billed directly, these outcomes influence long-term revenue retention and contract expansion.
Auxira’s revenue approach prioritizes stability over transaction volume. By aligning pricing with enterprise operations and long-term outcomes, it supports sustainable growth for both the provider and the platform.
Tele-Cardiology Systems Cut Critical Delays by 33.3 Minutes
Tele-cardiology platforms reduce treatment delays by 33.3 minutes, accelerate ECG interpretation, and lower specialist dependency by shifting cardiac decisions upstream using remote ECG, AI triage, and tele-echo workflows.
Primary research now shows that tele-cardiology is not just improving access. It is fundamentally reshaping time-to-treatment, specialist utilization, and operational efficiency across care networks.
1. Prehospital Tele-ECG Accelerates Reperfusion Decisions
A 2024 primary study found that prehospital digital ECG transmission reduced door-to-device time by 33.3 minutes when compared to standard workflows. This reduction occurred before patients even entered the catheterization labs.
By transmitting ECG data directly from ambulances to cardiac teams, hospitals were able to activate cath labs earlier and eliminate avoidable handoffs.
Enterprise impact:
- Faster STEMI activation without expanding on-site cardiology teams
- More predictable emergency workflows
- Improved outcomes tied to time-based cardiac KPIs
2. AI-Assisted Tele-ECG Delivers Specialist-Grade Speed
In a real-world emergency network study analyzing 22,159 ECGs, AI-assisted tele-ECG systems achieved a median report turnaround time of 75 seconds. Even high-risk STEMI cases were reported in a median of 375 seconds.
Within that cohort, STEMI prevalence was 0.9% (202 cases), highlighting how tele-cardiology systems help clinicians identify rare but critical events without slowing overall throughput.
Enterprise impact:
- Cardiologists focus on high-risk cases instead of screening volume
- Emergency departments reduce interpretation bottlenecks
- AI becomes a throughput accelerator, not a diagnostic replacement
3. Tele-Echo Reduces Specialist Visits
In a neonatal tele-echocardiography program, remote cardiology consultations eliminated the need for in-person specialist visits in 194 cases. An additional 26 consultations were safely delayed, saving approximately 4.2 specialist person-hours per week.
Care quality was maintained while specialist availability improved across facilities that previously relied on physical presence.
Enterprise impact:
- Fewer unnecessary transfers and on-site consultations
- Better utilization of limited cardiology expertise
- Scalable cardiac coverage across multiple hospitals
Tele-cardiology platforms prove their value where it matters most: time, access, and consistency. Cutting over half an hour from critical workflows, delivering ECG interpretations in seconds, and reducing specialist load are not marginal gains. They reshape how cardiac care scales.
Key Capabilities of a WL Tele-Cardiology Platform Like Auxira
A white-label tele-cardiology platform like Auxira combines cardiac-specific workflows, remote monitoring, specialist coordination, and EHR-native integration to deliver scalable, governed cardiology care.
Platforms modeled after Auxira focus on precision, continuity, and governance rather than generic telehealth functionality.
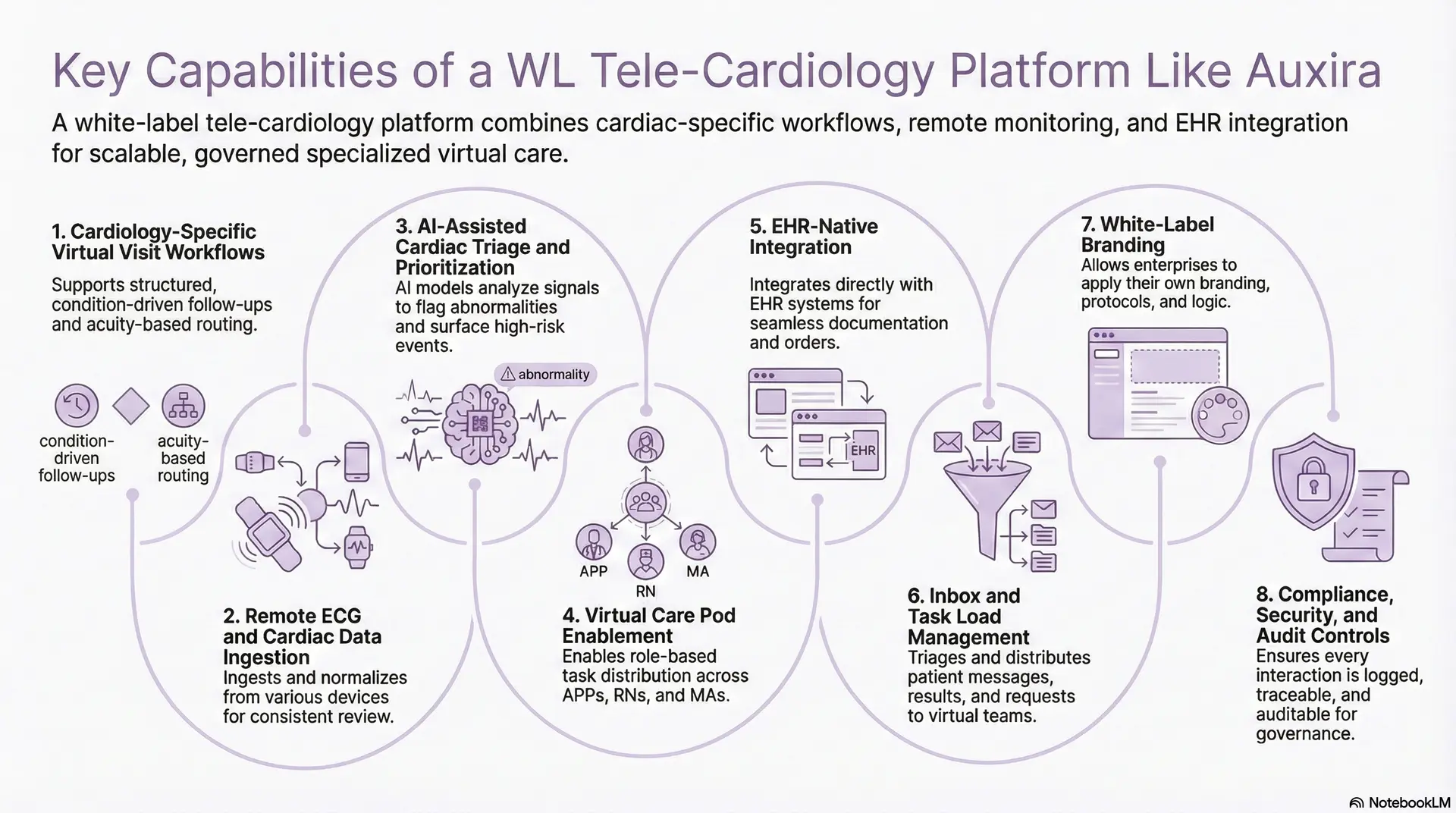
1. Cardiology-Specific Virtual Visit Workflows
Unlike general telehealth, cardiology visits follow condition-driven pathways. White-label tele-cardiology platforms support structured follow-ups for heart failure, arrhythmia monitoring, post-procedure checks, and medication titration.
Visits are routed based on acuity and protocol. Low-risk interactions are handled by APPs or nurses, while cardiologists engage only when escalation thresholds are met. This preserves care quality while expanding appointment capacity without adding physicians.
2. Remote ECG and Cardiac Data Ingestion
These platforms ingest ECGs, telemetry, and RPM data from ambulatory devices, clinics, and emergency settings. Data normalization ensures cardiologists review consistent signal formats regardless of source.
This capability eliminates manual uploads and fragmented reviews. It also allows cardiac data to flow directly into patient records, enabling faster interpretation and better continuity across encounters.
3. AI-Assisted Cardiac Triage and Prioritization
AI models analyze incoming cardiac signals to flag abnormalities, detect trends, and surface high-risk events. The system prioritizes what needs attention now versus what can wait.
Crucially, AI supports triage rather than diagnosis. Clinicians remain accountable for decisions, while AI reduces noise and cognitive load in high-volume environments.
4. Virtual Care Pod Enablement
White-label platforms support role-based task distribution across APPs, RNs, and MAs. Each role operates within defined scopes, protocols, and escalation rules.
This mirrors Auxira’s pod-based model, allowing routine work to move out of physician queues. As a result, cardiologists spend more time on complex cases instead of inbox management.
5. EHR-Native Integration
Enterprise adoption depends on workflow continuity. These platforms integrate directly with EHR systems for documentation, orders, messaging, and result review.
Clinicians do not switch tools or duplicate work. Cardiac care becomes an extension of existing workflows rather than a parallel system that erodes efficiency.
6. Inbox and Task Load Management
Patient messages, test results, refill requests, and follow-up questions are triaged and distributed across virtual teams. Tasks are prioritized based on urgency and clinical relevance.
This prevents cardiologists from becoming default owners of every interaction. It also reduces after-hours EHR time, a major driver of burnout.
7. White-Label Branding
Enterprises can apply their own branding, care protocols, escalation logic, and documentation standards. The platform adapts to regional regulations and organizational preferences.
This flexibility enables multi-entity deployments while preserving a consistent patient experience and clinical governance model.
8. Compliance, Security, and Audit Controls
Security is embedded across data ingestion, access controls, and clinical actions. Every interaction is logged, traceable, and auditable.
This level of governance supports HIPAA alignment, internal risk management, and long-term regulatory readiness for cardiac programs.
A white-label tele-cardiology platform like Auxira succeeds because it aligns technology with how cardiology actually functions. When features are designed to protect specialist time, manage data intelligently, and integrate deeply with enterprise systems, tele-cardiology becomes a durable growth capability rather than a temporary fix.
Architecture of a WL Tele-Cardiology Platform Like Auxira
A white-label tele-cardiology platform like Auxira uses a layered architecture that integrates cardiac devices, AI triage, clinical workflows, and EHR systems into a secure, scalable enterprise framework.
Platforms modeled after Auxira are built to function as clinical infrastructure. Each architectural layer solves a specific operational challenge while supporting long-term scalability, governance, and integration.
1. Device and Data Ingestion Layer
This layer is responsible for acquiring cardiac data from diverse sources, including ambulatory ECG devices, wearable monitors, bedside telemetry, and home-based RPM tools. It must support both continuous streams and episodic uploads without loss or delay.
Beyond simple connectivity, this layer validates signal quality, timestamps events, and standardizes incoming data formats. By resolving device-level variability early, the platform ensures downstream systems operate on consistent, reliable cardiac signals regardless of where or how data is captured.
2. Clinical Data Processing Layer
Once ingested, raw cardiac data is transformed into clinically usable information. This layer performs signal conditioning, noise filtering, artifact detection, and baseline normalization to prepare data for interpretation.
Crucially, raw data is preserved alongside processed outputs. This allows clinicians to revisit original signals when needed and supports auditability, clinical review, and model validation over time. The layer acts as a bridge between device-grade data and clinical-grade insight.
3. AI and Clinical Decision Support Layer
This layer applies machine learning and rule-based logic to identify abnormal rhythms, trend deviations, and escalation triggers across large data volumes. Its purpose is prioritization, not autonomous diagnosis.
AI outputs are contextualized within clinical thresholds and practice-specific protocols. Human-in-the-loop safeguards ensure that clinicians retain decision authority, which is essential for regulatory compliance and clinical trust. At scale, this layer reduces cognitive overload while preserving accountability.
4. Workflow Automation Layer
The workflow automation layer translates clinical signals into actionable work. It routes alerts, follow-ups, and tasks to the appropriate role based on acuity, protocol, and current workload.
This logic mirrors real cardiology operations. Routine interactions flow to nurses or APPs, while cardiologists are engaged selectively. By automating coordination, the platform prevents bottlenecks and eliminates reliance on manual task assignment.
5. Application and Experience Layer
This layer delivers role-specific interfaces for clinicians and patients. Cardiologists access prioritized worklists, ECG viewers, and escalation alerts. Nurses and APPs manage follow-ups, symptom checks, and inbox activity.
Patients interact through branded portals or mobile applications for messaging, virtual visits, and care updates. The experience remains consistent and intuitive, reinforcing trust while reducing operational friction.
6. Integration and Interoperability Layer
Enterprise tele-cardiology platforms must integrate deeply with existing systems. This layer connects the platform to EHRs, scheduling tools, billing systems, and analytics environments using standards-based interfaces.
Clinical insights flow directly into patient records, ensuring continuity across care settings. This integration prevents duplicate documentation and allows tele-cardiology to function as part of daily operations rather than a parallel workflow.
7. Security and Governance Layer
Security is embedded across identity management, access control, encryption, and audit logging. Every clinical interaction, data access event, and AI output is traceable.
This layer supports HIPAA alignment, internal risk management, and regulatory readiness. It also enables enterprises to enforce clinical accountability across distributed teams and virtual care models.
8. Infrastructure and Scalability Layer
The underlying infrastructure is designed for elasticity and resilience. Cloud-native services scale automatically based on data volume and clinical demand, ensuring performance during peak cardiac events.
This layer supports high availability, disaster recovery, and cost-efficient growth. Enterprises can expand services without re-architecting the platform or overprovisioning resources.
A white-label tele-cardiology platform like Auxira succeeds because its architecture respects clinical reality. This architectural discipline is what allows tele-cardiology to scale safely, operate reliably, and remain adaptable as care models evolve.
AI Capabilities Of WL Tele-Cardiology Platforms Like Auxira
AI in white-label tele-cardiology platforms like Auxira supports cardiac triage, risk prioritization, and workflow efficiency while keeping clinical decisions under physician control.
When implemented correctly, AI becomes an operational amplifier that improves speed and consistency without compromising accountability.

1. AI-Assisted ECG Interpretation
AI models analyze incoming ECG and telemetry data to identify abnormal rhythms, waveform deviations, and patterns that warrant attention. This occurs across large data volumes that would otherwise overwhelm manual review.
The system highlights findings and context, allowing clinicians to review critical cases first. Final interpretation remains with cardiologists, preserving clinical responsibility.
2. Automated Risk Stratification
AI continuously assesses patient data to categorize risk levels based on predefined clinical thresholds and historical trends. Patients showing early signs of deterioration move higher in review queues.
This prioritization ensures limited specialist time is spent where impact is highest, especially in high-volume or distributed care networks.
3. Event Detection for Heart Failure
For patients enrolled in remote monitoring programs, AI tracks longitudinal changes rather than isolated data points. Subtle trends, such as rising heart rate variability or weight fluctuations, trigger alerts.
This supports earlier intervention and reduces avoidable acute events without increasing manual oversight.
4. Workflow Automation and Task Routing
AI assists in routing tasks, messages, and alerts to the appropriate care team member. Routine actions flow to nurses or APPs, while escalation criteria bring cardiologists into the loop.
This reduces manual coordination and prevents workflow bottlenecks during peak periods.
5. Clinical Decision Support
Clinical decision support tools provide evidence-based guidance, protocol reminders, and contextual insights during reviews. These prompts are designed to assist, not direct, clinical decisions.
Bounded support helps maintain compliance with regulatory expectations around clinical autonomy.
6. Data Quality Monitoring
AI models assess signal quality at ingestion, flagging artifacts or incomplete data before review. This prevents clinicians from wasting time on unusable inputs.
Consistent data quality improves diagnostic confidence and operational efficiency.
7. Learning and Continuous Optimization
Over time, AI models adapt based on feedback, outcomes, and evolving protocols. Performance is monitored, validated, and adjusted within governed frameworks.
This ensures the system improves without introducing uncontrolled behavior.
AI capabilities in white-label tele-cardiology platforms like Auxira are most effective when they remain invisible to patients and supportive to clinicians. By focusing on prioritization, workflow efficiency, and early risk detection, AI strengthens cardiac care delivery without compromising trust, safety, or governance.
Compliance Requirements for Tele-Cardiology Platforms
Tele-cardiology platforms require built-in compliance across data privacy, clinical governance, and auditability to support safe, scalable cardiac care delivery.
For white-label tele-cardiology platforms, compliance must be designed into the system rather than enforced after deployment. Platforms modeled after Auxira treat compliance as an operational layer that governs every interaction.
1. Patient Data Privacy and Security Standards
Tele-cardiology platforms handle protected health information across devices, networks, and care teams. Systems must align with HIPAA requirements for data storage, transmission, and access control.
Encryption at rest and in transit, role-based access, and identity verification protect sensitive cardiac data. These safeguards must operate consistently across clinical and administrative workflows.
2. Clinical Accountability and Decision Governance
Remote cardiac care does not remove clinical responsibility. Platforms must clearly define who reviews data, who makes decisions, and how escalations occur.
Audit trails capture actions, timestamps, and user roles. This supports internal governance, clinical review, and regulatory readiness without slowing care delivery.
3. AI and Clinical Decision Support Boundaries
AI use in tele-cardiology is subject to strict oversight. Systems must ensure AI assists clinicians without making autonomous clinical decisions.
Clear documentation of model intent, outputs, and limitations is essential. Human-in-the-loop controls protect against overreliance and support regulatory compliance.
4. Medical Device and Software Regulations
Tele-cardiology platforms often interface with regulated medical devices. Depending on functionality, components may fall under the FDA Software as a Medical Device guidance or equivalent regional frameworks.
Architects must separate decision support from diagnostic authority to reduce regulatory risk while enabling innovation.
5. Interoperability and Data Integrity Requirements
Integration with EHRs and cardiac devices introduces compliance obligations around data accuracy and traceability. Standards-based interfaces help maintain consistency across systems.
Version control, data reconciliation, and validation processes ensure that clinical records remain reliable and defensible.
6. Multi-Entity and Cross-Region Compliance Management
Enterprises operating across regions face varying regulatory requirements. White-label platforms must support configurable policies for different jurisdictions.
This flexibility allows organizations to scale without rebuilding compliance frameworks for each deployment.
Compliance requirements shape how tele-cardiology platforms are built, deployed, and governed. When embedded into architecture and workflows, compliance strengthens trust and scalability.
How We Build WL Tele-Cardiology Platforms Like Auxira
Building a white-label tele-cardiology platform is not about assembling features. It is about designing a system that can carry clinical responsibility, scale safely, and integrate into existing enterprise operations. At Intellivon, we approach this as a long-term infrastructure decision, not a short-term digital rollout.
Our process reflects how cardiology actually works at scale and how enterprise healthcare systems make technology investments.
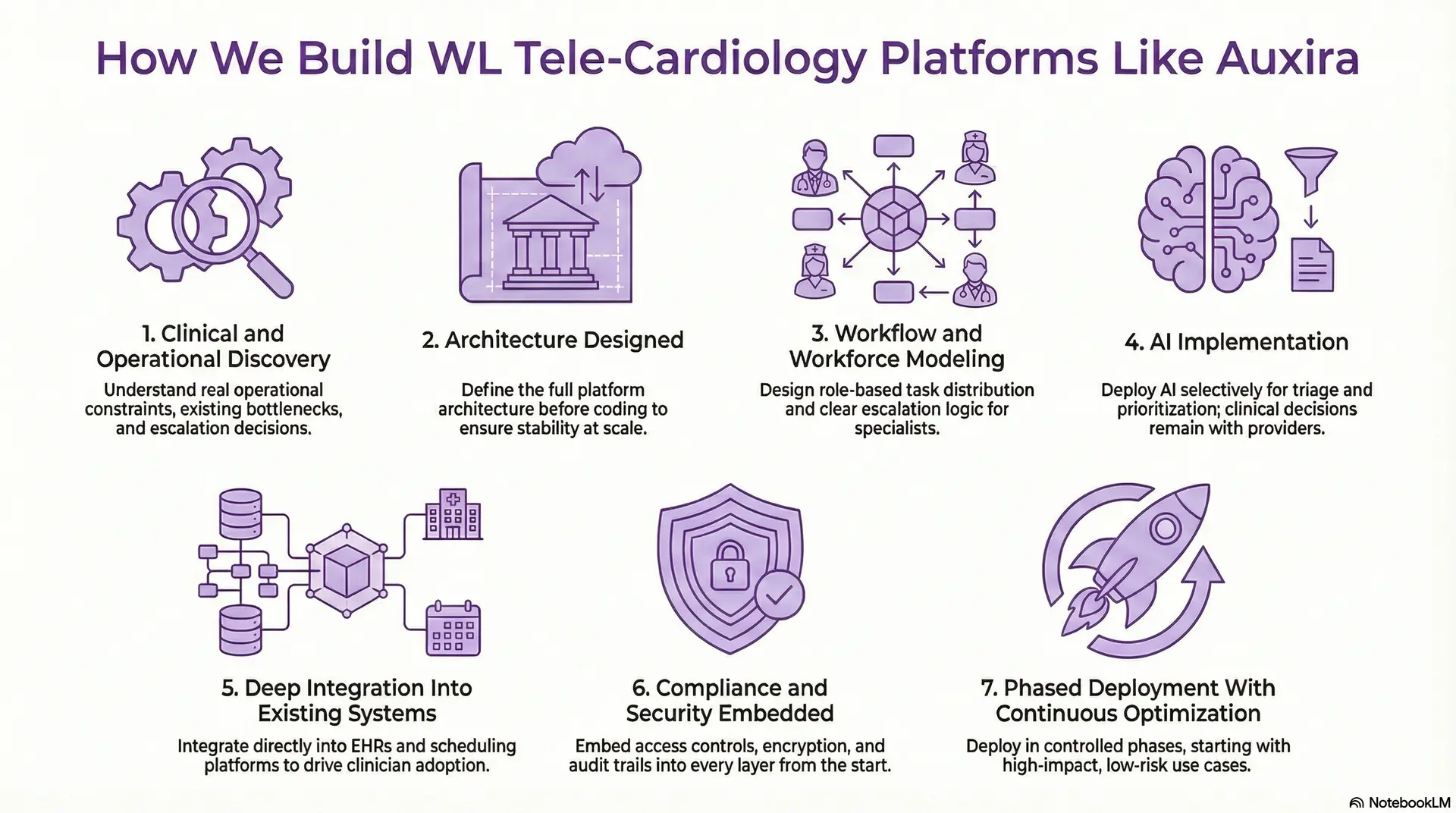
1. Clinical and Operational Discovery
We begin by understanding how cardiology work is performed today across clinics, hospitals, and remote settings. This includes how follow-ups are managed, how inbox load accumulates, where delays occur, and how escalation decisions are currently made.
We analyze specialist availability, case mix, risk distribution, and existing bottlenecks. This discovery phase ensures the platform is designed around real operational constraints, not assumptions. It also helps define which workflows should move into virtual care first and which must remain tightly controlled.
2. Architecture Designed
Before writing code, we define the full platform architecture across ingestion, processing, AI support, workflow orchestration, integration, and governance layers. Each layer has a clearly defined responsibility.
This prevents the common enterprise failure of building for pilot success and then re-architecting under scale. By designing for peak cardiac volumes and multi-entity deployments from the start, the platform remains stable as adoption grows.
3. Workflow and Workforce Modeling
Technology does not solve capacity problems unless workflows change. We design role-based task distribution models that reflect the scopes of practice for cardiologists, APPs, nurses, and medical assistants.
Escalation logic ensures specialists engage only when clinical thresholds are met. Routine tasks, follow-ups, and inbox management are routed to appropriate roles. This mirrors Auxira-style virtual pod models and allows enterprises to expand services without increasing physician burnout.
4. AI Implementation
We deploy AI selectively and intentionally. Models support triage, prioritization, signal quality assessment, and trend detection across large data volumes.
Clinical decision-making always remains with licensed providers. Every AI output is contextualized, traceable, and governed. This approach builds clinician trust and ensures alignment with regulatory expectations around decision support.
5. Deep Integration Into Existing Systems
We integrate tele-cardiology workflows directly into existing EHRs, scheduling platforms, messaging systems, and reporting tools. Clinicians continue working inside familiar environments without duplicating documentation.
This depth of integration is critical for adoption. Tele-cardiology becomes part of daily operations rather than an external tool that competes for attention.
6. Compliance and Security Embedded
Compliance is not treated as a post-build checklist. We embed access controls, encryption, audit trails, and governance mechanisms into every layer of the platform.
This allows enterprises to scale across regions and service lines without revisiting compliance design. It also supports internal audits, clinical review, and long-term regulatory readiness.
7. Phased Deployment With Continuous Optimization
We deploy platforms in controlled phases, starting with high-impact, low-risk use cases. Early feedback informs workflow tuning, performance optimization, and AI calibration.
As volume grows, we continuously monitor system behavior, clinician adoption, and operational outcomes. This ensures the platform improves over time without introducing instability.
Intellivon builds white-label tele-cardiology platforms like Auxira by aligning enterprise architecture with clinical reality. Through disciplined discovery, scalable design, governed AI, and deep integration, we help organizations launch platforms that deliver real operational impact today and remain resilient as cardiac care demands evolve.
Cost to Build a WL Tele-Cardiology Platform Like Auxira
For healthcare enterprises starting with one or two high-impact cardiology workflows, such as post-visit follow-ups, remote ECG review, or low-acuity virtual cardiology visits, a white-label tele-cardiology platform can be built within a controlled, enterprise-ready budget. The determining factor is not ambition, but how intentionally the platform is phased.
At Intellivon, we structure tele-cardiology cost models around leadership budget cycles, clinical risk, and near-term operational ROI. Rather than attempting to digitize all cardiology services at once, we focus on building a cardiology-native core that integrates cleanly with existing EHR systems and scales safely as adoption grows.
Estimated Phase-Wise Cost Breakdown
| Phase | Description | Estimated Cost (USD) |
| Clinical & Operational Discovery | Cardiology pathway mapping, follow-up, and RPM use-case prioritization, workflow analysis,and regulatory scoping | 10,000 – 18,000 |
| Architecture & Interoperability Blueprint | Tele-cardiology architecture, ECG/RPM ingestion design, FHIR/HL7 workflows, security framework | 15,000 – 28,000 |
| Core Tele-Cardiology Platform Development | Virtual cardiology visits, care pod workflows, task routing, scheduling logic | 30,000 – 55,000 |
| EHR Integration & Cardiology Data Sync | ECG data write-back, chart context, orders, documentation, inbox integration | 20,000 – 35,000 |
| AI-Assisted Triage & Signal Processing | ECG prioritization, risk stratification, data quality checks (non-autonomous AI) | 15,000 – 30,000 |
| Security, IAM & Compliance Controls | Role-based access, encryption, audit trails, consent management | 12,000 – 20,000 |
| Clinical Analytics & Operational Reporting | Utilization dashboards, turnaround times, cardiologist workload metrics | 8,000 – 15,000 |
| Testing, QA & Compliance Validation | Workflow testing, device validation, security testing | 10,000 – 16,000 |
| Pilot Deployment & Clinical Training | Live rollout, clinician onboarding, workflow optimization | 12,000 – 20,000 |
Total Initial Investment Range: USD 130,000 – 220,000
This range supports a secure, white-label tele-cardiology platform deployed for a single cardiology service line in a live clinical environment, integrated with existing EHR workflows and cardiologist operations.
Annual Maintenance and Optimization
Ongoing costs typically include infrastructure management, EHR and device integration upkeep, security monitoring, AI model tuning, and platform support.
12–20% of the initial build cost annually
Approx. USD 16,000 – 44,000 per year
Costs remain predictable when cardiology-specific workflows, interoperability, and compliance are engineered correctly from the beginning.
Hidden Costs Healthcare Organizations Should Plan For
Even well-architected tele-cardiology platforms introduce expansion-related cost variables over time:
- Scaling to additional cardiology subspecialties or clinics
- Onboarding new ECG or RPM device vendors
- EHR upgrades or interoperability changes
- Increased cloud usage from continuous cardiac data streams
- AI model validation and governance updates
- Clinician training and workflow change management
Planning for these early stages prevents budget pressure during regional or service-line expansion.
Best Practices to Stay Within the USD 130K–220K Range
Healthcare enterprises that successfully control tele-cardiology platform costs typically:
- Start with one clearly defined, high-volume cardiology use case
- Limit multi-region and multi-EHR complexity in phase one
- Use modular, layered architecture for incremental expansion
- Embed compliance and governance from day one
- Track adoption, turnaround times, and workload reduction in the first 90 days
This ensures the platform proves both clinical and financial value before broader capital deployment.
Talk to Intellivon’s healthcare platform architects to receive a phased cost estimate aligned with your cardiology growth strategy and enterprise roadmap.
Common Mistakes When Building WL Tele-Cardiology Platforms
At enterprise scale, tele-cardiology initiatives rarely fail because of missing features. They fail because of architectural shortcuts, governance gaps, or misalignment with how cardiology actually operates. These mistakes often surface months after launch, when scale, compliance, or clinician adoption becomes difficult to sustain.
The following challenges consistently appear in large health systems and enterprise care networks.
1. Treating Tele-Cardiology as a Generic Telehealth Extension
Many enterprises attempt to layer cardiology workflows onto existing telehealth platforms. These systems are built for episodic video visits, not continuous cardiac data, time-sensitive escalation, or specialist-driven decision flows.
As volume grows, teams struggle with fragmented ECG reviews, unclear escalation paths, and overloaded cardiologists. The platform technically works, but operationally collapses under real cardiac demand.
How Intellivon Solves This:
Intellivon designs tele-cardiology platforms as cardiology-first systems from the ground up. Workflows, data pipelines, and interfaces are built specifically around ECG review, RPM signals, and cardiologist-led escalation. This ensures the platform scales with clinical complexity rather than fighting it.
2. Underestimating EHR Integration Depth
Enterprise teams often assume basic EHR connectivity is sufficient. In reality, shallow integrations force clinicians to document in multiple systems, manually reconcile data, or manage parallel inboxes.
Over time, this increases administrative burden and reduces adoption, even if the tele-cardiology capabilities themselves are strong.
How Intellivon Solves This:
We prioritize deep, workflow-native EHR integration. Tele-cardiology actions, documentation, and follow-ups occur inside existing clinical systems. This preserves continuity, reduces duplication, and accelerates clinician buy-in across departments.
3. Over-Reliance on AI Without Governance
AI is often deployed aggressively to demonstrate innovation. Without clear boundaries, enterprises risk creating systems that blur responsibility, confuse clinicians, or raise regulatory concerns.
When AI outputs are not contextualized or governed, trust erodes quickly, especially in high-risk cardiac care.
How Intellivon Solves This:
Intellivon implements AI with strict human-in-the-loop controls. Models support triage, prioritization, and data quality, while clinical decisions remain with licensed providers. Governance, auditability, and model transparency are built into the platform from day one.
4. Ignoring Workforce and Workflow Design
Technology alone does not solve cardiology capacity constraints. Many platforms fail because they do not redesign how work is distributed across APPs, nurses, and specialists.
Without role-based workflows, cardiologists continue to absorb inbox load, follow-ups, and low-acuity tasks, negating the value of tele-cardiology.
How Intellivon Solves This:
Our experts build platforms that support pod-based, role-aligned care models similar to Auxira. Task routing, escalation logic, and dashboards are designed around real scopes of practice, allowing enterprises to rebalance workload without adding physician headcount.
5. Building for Pilot Scale
Many tele-cardiology platforms are designed to succeed in pilots but struggle under network-wide rollout. Performance issues, data bottlenecks, and brittle integrations appear as volume increases.
This forces expensive re-architecture after deployment.
How Intellivon Solves This:
Intellivon engineers tele-cardiology platforms using cloud-native, modular architectures that scale elastically. From ingestion to analytics, each layer is built to handle enterprise-level load without redesign, protecting long-term investment.
6. Treating Compliance as Post-Launch Concern
Some enterprises delay compliance hardening until after launch to move faster. In regulated cardiac care, this creates risk exposure and limits expansion across regions or service lines.
Retrofitting compliance is costly and disruptive.
How Intellivon Solves This:
Intellivon embeds compliance into architecture and workflows from the start. Security, auditability, and clinical accountability are foundational layers, not add-ons. This enables faster expansion without regulatory friction.
Enterprise tele-cardiology platforms fail when strategy, architecture, and clinical reality fall out of alignment. The most successful systems are built with scale, governance, and workflow redesign in mind from the outset. By addressing these enterprise-level challenges directly, Intellivon enables organizations to build white-label tele-cardiology platforms that remain stable, trusted, and effective as demand grows.
Conclusion
White-label tele-cardiology platforms represent a structural shift in how cardiac care is delivered, governed, and scaled. What platforms like Auxira demonstrate is not simply the feasibility of remote cardiology but the operational advantage of owning the care model, the workflows, and the underlying technology. For enterprises, this is no longer a question of innovation, but of strategic readiness.
When built correctly, these platforms reduce specialist overload, shorten response times, and extend cardiology services across regions without increasing clinical risk. More importantly, they create a foundation for long-term growth by aligning clinical outcomes with operational efficiency and financial sustainability.
Build Your White-Label Tele-Cardiology Platform With Intellivon
At Intellivon, we build white-label tele-cardiology platforms that operate as a core part of cardiology service delivery, not as add-on telehealth tools. Our platforms integrate directly into cardiology practices, hospitals, and enterprise care networks, enabling remote ECG review, virtual follow-ups, RPM-driven interventions, and specialist coordination through a single governed system.
Each solution is engineered for enterprise healthcare environments. Platforms are cardiology-native, compliant by design, resilient under continuous cardiac data load, and built to deliver measurable clinical, operational, and financial ROI as cardiology services expand across regions and care settings.
Why Partner With Intellivon?
- Cardiology-first platform design aligned with real-world specialist workflows, virtual care pods, and enterprise care delivery models
- Deep interoperability expertise across EHRs, ECG and RPM devices, HL7, FHIR, and secure enterprise APIs
- Compliance-first architecture supporting HIPAA, role-based access, audit trails, AI governance, and clinical accountability
- AI-enabled operational intelligence for cardiac triage, prioritization, workload balancing, and performance analytics
- Scalable, cloud-native delivery with phased rollout control, resilience planning, and continuous optimization
Book a strategy call to explore how a white-label tele-cardiology platform like Auxira can expand cardiac capacity, improve specialist utilization, and support long-term enterprise growth with Intellivon as your delivery partner.
FAQs
Q1. What is a white-label tele-cardiology platform?
A1. A white-label tele-cardiology platform is a customizable remote cardiac care system that enterprises deploy under their own brand. It integrates ECG review, virtual cardiology visits, RPM data, and EHR workflows into a single governed platform.
Q2. How is tele-cardiology different from general telehealth platforms?
A2. Tele-cardiology supports cardiac-specific workflows such as ECG interpretation, heart failure monitoring, medication titration, and risk-based triage. General telehealth platforms lack the data pipelines, escalation logic, and specialist workflows required for cardiology at scale.
Q3. How much does it cost to build a white-label tele-cardiology platform like Auxira?
A3. Building an enterprise-grade white-label tele-cardiology platform typically costs between USD 130,000 and 220,000 for an initial service line. Costs depend on EHR integration depth, AI capabilities, compliance requirements, and phased rollout strategy.
Q4. Can white-label tele-cardiology platforms integrate with existing EHR systems?
A4. Yes. Enterprise tele-cardiology platforms are designed to integrate directly with EHRs using standards such as FHIR and HL7. This allows documentation, orders, messages, and cardiac data to flow into existing clinical workflows.
Q5. Is AI allowed in tele-cardiology platforms for cardiac decision-making?
A5. AI can be used for triage, prioritization, signal quality assessment, and trend detection. Clinical decisions must remain with licensed providers, with AI operating under human-in-the-loop governance and clear regulatory boundaries.



