
Key Takeaways:
- AI revenue cycle automation connects registration, coding, claims, denials, payments, and analytics into one system.
- EHR integration, HL7/FHIR R4, and EDI 837/835 handling are foundational technical requirements for RCM automation.
- Payer-rule logic, predictive denial models, and MLOps keep the platform accurate as policies change.
- Custom builds range from $80,000 to $350,000, depending on AI depth and enterprise scale.
- How Intellivon builds revenue cycle automation as production infrastructure, not isolated point-solution automation tools.
Hospital networks and RCM teams typically run revenue operations across six to eight disconnected systems. Within this network, the EHR doesn’t talk to the clearinghouse, and the clearinghouse doesn’t talk to the denial management tool. At the same time, every handoff is a place where revenue leaks, silently, at scale, across every billing cycle.
That fragmentation is exactly the problem an AI revenue cycle automation platform is built to solve. By unifying front-end access, mid-cycle coding and claims, and back-end denial and payment workflows into a single orchestrated system, it closes the gaps that disconnected point solutions leave open. As a result, denial patterns become predictive signals rather than reactive work queues, and underpayments surface automatically instead of aging in AR.
Rather than correcting individual failures one cycle at a time, a well-architected platform drives clean claim rate improvements that build on themselves over successive billing cycles.
Intellivon builds these systems for hospital networks, RCM companies, and healthcare SaaS platforms, and the architecture decisions here come directly from that production experience. With that context established, this post covers platform architecture, AI model selection, EHR integration, HIPAA compliance engineering, phased development costs, and the build vs. buy decision framework.
Why Are Healthcare Enterprises Adopting AI RCM Platforms?
Healthcare automation is shifting from isolated department-level pilots into core enterprise infrastructure. Hospitals, payers, RCM companies, and healthcare SaaS platforms all face severe economic pressures. They need measurable workflow efficiency, faster cash movement, lower administrative burdens, and clear operational visibility.
Because of this, the strongest technology opportunities now sit in administrative workflows where an AI revenue cycle automation platform can prove direct ROI within 6 to 18 months.
1. Key Takeaways From the Healthcare Automation Market
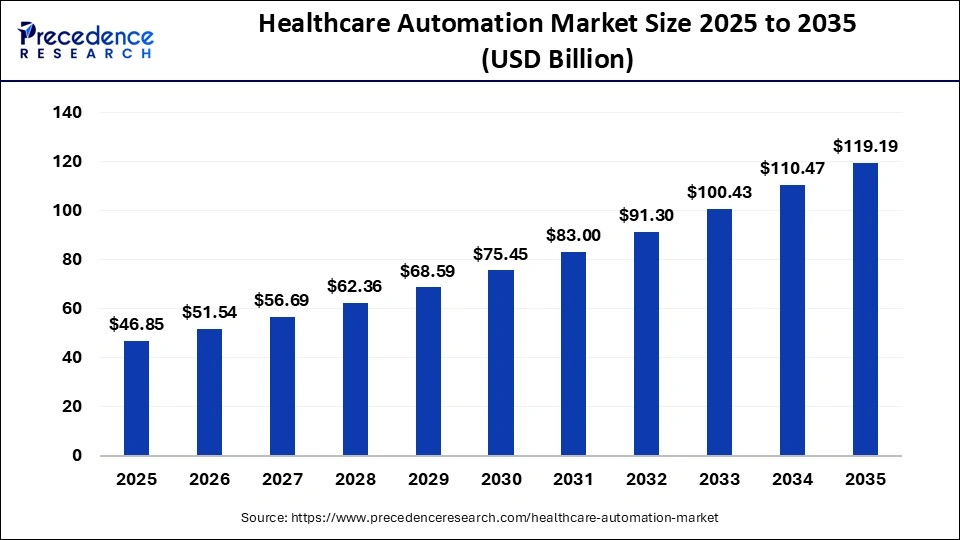
This massive scaling proves that enterprise buyers are moving away from isolated software bots and toward unified orchestration platforms. These modern platforms seamlessly connect EHRs, payer systems, documentation workflows, analytics, and compliance controls.
- Rapid Market Growth: The broader AI in healthcare market is expanding even faster, scaling from USD 36.67B in 2025 to USD 505.59B by 2033.
- Operational Pressure Over Innovation Hype: Growth is driven by thin hospital margins and staff shortages rather than experimental tech budgets, forcing a focus on immediate administrative workload reduction.
- Measurable Financial Targets: Revenue cycle operations are the preferred target for automation because every upgrade directly impacts financial performance metrics.
- Clear Performance Indicators: Systems prove their value rapidly by increasing clean claim rates, reducing days in AR, slashing denial rates, and lowering the total cost-to-collect.
2. Strategic Opportunities for Enterprises Entering This Market
Enterprises entering the AI RCM platform development space must focus on narrow, high-friction workflows before trying to build full-scale orchestration systems.
Software product leaders and hospital CTOs should prioritize workflows with measurable financial or operational ROI within a 6 to 18-month window.
By proving value with smaller deployments first, you secure the organizational alignment needed to expand into complete revenue workflow orchestration.
- Target High-Friction Gateways: Start with front-end and mid-cycle bottlenecks such as prior authorization, claim scrubbing, payment posting, or AR prioritization.
- Focus on Key Yield Metrics: Prioritize immediate denial prevention, automated documentation time reduction, and instant eligibility verification to accelerate cash collections.
- Build Dense Integration Layers: Engineer the software architecture around deep, native connections to EHRs, clearinghouses, and payer systems using modern data standards.
- Utilize Modern Standards: Implement native support for HL7 and FHIR R4 protocols to ensure smooth, secure communication across legacy healthcare networks.
- Bake Security Into the Core: Build strict HIPAA controls, detailed user auditability, role-based access governance, and PHI minimization rules from day one of development.
The rapid growth of AI-driven healthcare automation is driven forward by operational necessity, not market hype.
For enterprise builders and healthcare networks, this environment creates a rare, profitable alignment between market maturity, regulatory readiness, and measurable financial ROI.
Within the RCM sector specifically, companies that move early with a structured platform strategy will permanently reshape how revenue operations function across patient access, claims processing, denial management, payments, and financial analytics.
What Is an AI Revenue Cycle Automation Platform?
An AI revenue cycle automation platform is an integrated healthcare financial operations system that uses machine learning models, deterministic rule engines, data integrations, and automated workflows to manage the full lifecycle of a patient encounter.
Instead of automating a single administrative task in isolation, a true platform connects front-end, mid-cycle, and back-end revenue cycle management (RCM) workflows within a unified digital operating layer.
This comprehensive connectivity prevents structural data loss, eliminates communication silos between disparate software tools, and accelerates cash velocity by eliminating manual intervention points from patient intake to final payment resolution.
1. Unifying the End-to-End Billing Lifecycle
An enterprise-grade platform drives efficiency by dividing core operational workloads into three synchronized execution layers. These layers share real-time transaction tokens to pass context seamlessly across different billing teams and operational systems.
- Front-End Workflows: The system manages the initial patient access gateway by executing automatic patient registration, real-time eligibility verification, and prior authorization predictive checking.
- Mid-Cycle Workflows: The platform tracks active clinical documentation to run immediate charge capture, autonomous medical coding, and automated clinical documentation improvement (CDI) reviews.
- Back-End Workflows: The software performs precise claim scrubbing, automated claims submission, proactive denial prevention, electronic payment posting, and intelligence-driven accounts receivable (AR) management.
2. Platform Architecture vs. Isolated Point Solutions
Healthcare finance leaders often mistake basic billing utilities for comprehensive enterprise platforms.
To ensure clear product procurement and long-term engineering viability, CTOs and CFOs must evaluate how a full automation platform structurally differs from legacy billing software, standalone claim scrubbers, and narrow AI point tools.
| System Type | Architectural Scope | Data Processing Model | Primary Financial Impact |
| Legacy Billing Software | Back-end billing records only | Manual data entry with reactive batch uploads | Documents transactions without optimization |
| Standalone Claims Scrubber | Single clearinghouse checkpoint | Hardcoded, static payer edit rules | Catches formatting errors right before submission |
| AI Point Tool | Isolated workflow (e.g., Prior Auth) | One-off machine learning inference | Fixes a local bottleneck but creates a new data silo |
| AI Revenue Cycle Platform | Full end-to-end operational lifecycle | Multi-model agent orchestration via FHIR APIs | Lowers cost-to-collect and drops total days in AR |
3. Why Platform Orchestration Matters for CFOs and CTOs
For financial and technology executives, deploying a unified platform is a strategic imperative that directly impacts corporate margin performance and system interoperability.
Fragmented software tools require expensive custom middleware pipelines and create blind spots in operational data, which leads to avoidable revenue leakage.
A consolidated platform architecture allows healthcare enterprises to stabilize their cash flow by standardizing data structures and automating cross-departmental handoffs.
- Vendor Consolidation Economies: Eliminating disjointed software point tools slashes enterprise licensing overhead and simplifies annual compliance auditing workloads.
- Unified Financial Analytics: Consolidating workflows into a single system allows executive leaders to track real-time yield patterns and identify upstream leakage sources instantly.
By embedding machine learning models directly into an integrated data architecture, an enterprise platform allows healthcare networks to transition from reactive error correction to proactive revenue optimization.
This unified system strategy secures a sustainable financial foundation while reducing the administrative burden on operational staff.
Why Build Revenue Cycle Automation Software Instead of Adding Tools?
You choose to build healthcare revenue cycle automation software when commercial point tools fail to solve deep workflow fragmentation, shifting payer variability, and complex data ownership requirements.
A custom engineering approach becomes a necessity when your billing operations depend on a web of different EHRs, local clearinghouses, regional payers, and analytics platforms that off-the-shelf software cannot natively align.
This piecemeal strategy forces your engineering teams to construct expensive, fragile middleware pipelines to sync data between isolated applications, which ultimately increases your long-term technical debt.
1. Point Tools Deepen Workflow Fragmentation
Commercial point tools are engineered to target isolated slices of the billing cycle, such as medical coding, eligibility verification, denial management, or electronic payment posting.
While a single application might temporarily optimize a localized bottleneck, it forces staff to manually pass transaction contexts between different dashboards.
- The Coding Disconnect: Standalone autonomous coding utilities lack real-time access to the frontend eligibility engine, which prevents the system from matching clinical documentation directly to specific payer coverage limits.
- The Claim Scrubbing Gap: Isolated claim scrubbers operate reactively at the very end of the line, meaning they catch formatting errors but fail to inform upstream patient registration teams about recurring data entry mistakes.
2. Why Excess Dashboards Create Operational Drag
Forcing healthcare billing teams to manage multiple independent software platforms introduces severe operational fatigue and reduces daily workforce productivity.
When software product leaders and hospital networks continuously stack new AI vendor tools onto an existing billing stack, they create a fractured digital workspace that complicates staff training and tracking.
- The Multi-Login Bottleneck: Medical billing specialists spend a large percentage of their shifts logging into disparate interfaces and manually copying and pasting patient identifiers across conflicting windows.
- The Reddit Perspective: Healthcare practitioners frequently express frustration with this exact software setup, noting that independent AI RCM utilities often require “another platform and another webpage,” which drives up operational costs and causes staff adoption friction.
3. Aligning Enterprise RCM Systems for True Workflow Continuity
For technology and finance leaders at large hospital networks, RCM companies, and healthcare SaaS platforms, true efficiency requires end-to-end workflow continuity.
Off-the-shelf software tools cannot adapt to the unique, specialty-specific billing logic and proprietary database schemas that give enterprise providers their operational edge.
- Complete Data Autonomy: Retaining direct governance over your underlying operational data prevents vendor lock-in and allows you to build proprietary, long-term asset value.
- Custom Engine Tuning: A custom build lets your engineers optimize machine learning layers for complex clinical frameworks, such as high-acuity multi-specialty coding or specific regional payer guidelines.
By designing a unified financial operating environment, your organization can eliminate the systemic blind spots that lead to avoidable underpayment detection delays and claim rejections.
This foundational system control ensures that all frontend data flows naturally into backend collections without leaking cash along the way.
Core Automated Workflow By An AI Revenue Cycle Platform
An AI revenue cycle automation platform must orchestrate the workflows where financial risk originates early and compounds later across the billing lifecycle. Instead of operating as disconnected queues, your platform must share data fluidly across registration, eligibility, prior authorization, medical coding, claim validation, payment posting, and underpayment detection.
By linking these processes within a single data fabric, the system prevents data degradation, automates manual data handoffs, and eliminates the upstream errors that cause backend insurance denials.
1. Patient Registration Automation and Eligibility Verification
Patient registration automation and eligibility verification form the initial defensive layer against front-end revenue leakage.
The platform automatically ingests patient demographics from intake portals and insurance card images, checking them against real-time clearinghouse databases to confirm active plan coverage.
- Demographics Capture: Parses scanned driver’s licenses and intake documents to eliminate manual text entry mistakes during patient check-in.
- Insurance Plan Validation: Queries real-time X12 EDI 270 engines to instantly verify structural benefit details and active coverage status.
- Granular Benefit Extraction: Captures exact patient-responsibility variables, including remaining deductibles, co-insurance percentages, and co-payment thresholds.
- Front-End Error Prevention: Blocks dirty data from advancing by highlighting misspelled patient names or invalid policy ID numbers before clinical charting starts.
2. Prior Authorization and Medical Necessity Intake
Prior authorization automation evaluates scheduled procedures against dynamic payer rule networks to determine if a formal medical necessity approval is required.
The platform reads the initial clinical chart note, identifies the ordered procedure codes, and gathers the necessary documentation to submit an authorization packet to the payer.
- Procedure-Specific Verification: Cross-references scheduled CPT codes with active payer policy graphs to flag mandatory authorization rules.
- Documentation Capture: Automatically extracts relevant lab results and clinical history from the EHR to compile an audit-ready medical necessity packet.
- Payer Policy Mapping: Matches extraction targets to the shifting clinical trial criteria and documentation checklists enforced by individual commercial insurers.
- Regulatory API Compliance: Aligns with CMS mandates beginning in 2026, preparing system infrastructure for mandatory electronic prior authorization API requirements arriving in 2027.
3. Charge Capture and Autonomous Coding Support
Charge capture and autonomous medical coding systems use clinical Natural Language Processing (NLP) to read unstructured physician notes and translate them into compliant medical codes.
The platform processes Electronic Health Record documentation to suggest accurate clinical combinations for administrative review.
- Documentation Extraction: Scans provider progress notes, operative reports, and discharge summaries to find billable clinical activities.
- Multimodal Code Suggestion: Recommends specific, hierarchically accurate combinations of ICD-10-CM diagnosis codes, CPT procedure codes, and HCPCS Level II equipment codes.
- Confidence Scoring Model: Labels every suggested code combination with an objective percentage score to automatically route low-confidence charts to human coders.
- Specialty-Specific Logic: Adapts inference layers to handle unique documentation frameworks, such as complex multi-stage orthopedic surgeries or high-volume emergency medicine chart strings.
4. Claim Scrubbing and Denial Prevention
Claim scrubbing and predictive denial prevention microservices serve as the final validation checkpoint before electronic claims are transmitted to payers.
The system analyzes compiled bill data against historical clearinghouse records to identify hidden errors that lead to payment delays or flat rejections.
- Dynamic Rule Engine: Compares completed claims against millions of active payer edit rules, national bundling guidelines, and local coverage determinations.
- Pre-Submission Validation: Scans for structural alignment errors, missing subscriber modifiers, and mismatched diagnostic-to-procedure codes.
- Missing Data Checks: Flags missing operational fields, such as missing NPI provider numbers, invalid facility taxonomy codes, or incomplete rendering provider details.
- Predictive Denial Scoring: Scores every claim for rejection probability using machine learning models trained on your firm’s historical remittance codes.
5. Payment Posting and Underpayment Detection
Payment posting and underpayment detection engines automate cash reconciliation by parsing electronic remittance files and comparing settled amounts to contracted provider rate sheets.
This layer ensures that every processed insurance payment matches your exact legal contract agreements.
- Remittance File Ingestion: Processes incoming X12 EDI 835 electronic remittance advice files and matches them to historical patient encounters (Source: X12, 2026).
- Automated ERA/EOB Matching: Reconciles electronic payments directly against open accounts receivable balances without manual ledger cross-checking.
- Contracted-Rate Validation: Compares deposited insurance payouts against digitized payer contracts to spot systemic underpayments and silent payment shortfalls.
- AR Aging Prioritization: Updates active collection lists instantly, sorting outstanding uncollected claims by cash value and filing deadline constraints.
Once workflows are mapped, the architecture has to support them without breaking PHI control or revenue visibility.
AI Revenue Cycle Automation Platform Architecture
The architecture of an enterprise-grade AI revenue cycle automation platform must be structured across six decoupled functional layers: workflow orchestration, system integration, data normalization, AI decisioning, human review, and financial analytics. This modular design enables the platform to ingest and process complex clinical text, payer policies, claims documents, and bank payments simultaneously without creating system performance bottlenecks.
By separating core transaction processing from machine learning inference engines, engineering teams can guarantee that every single automated action remains fully traceable, explainable, and open to manual human override.
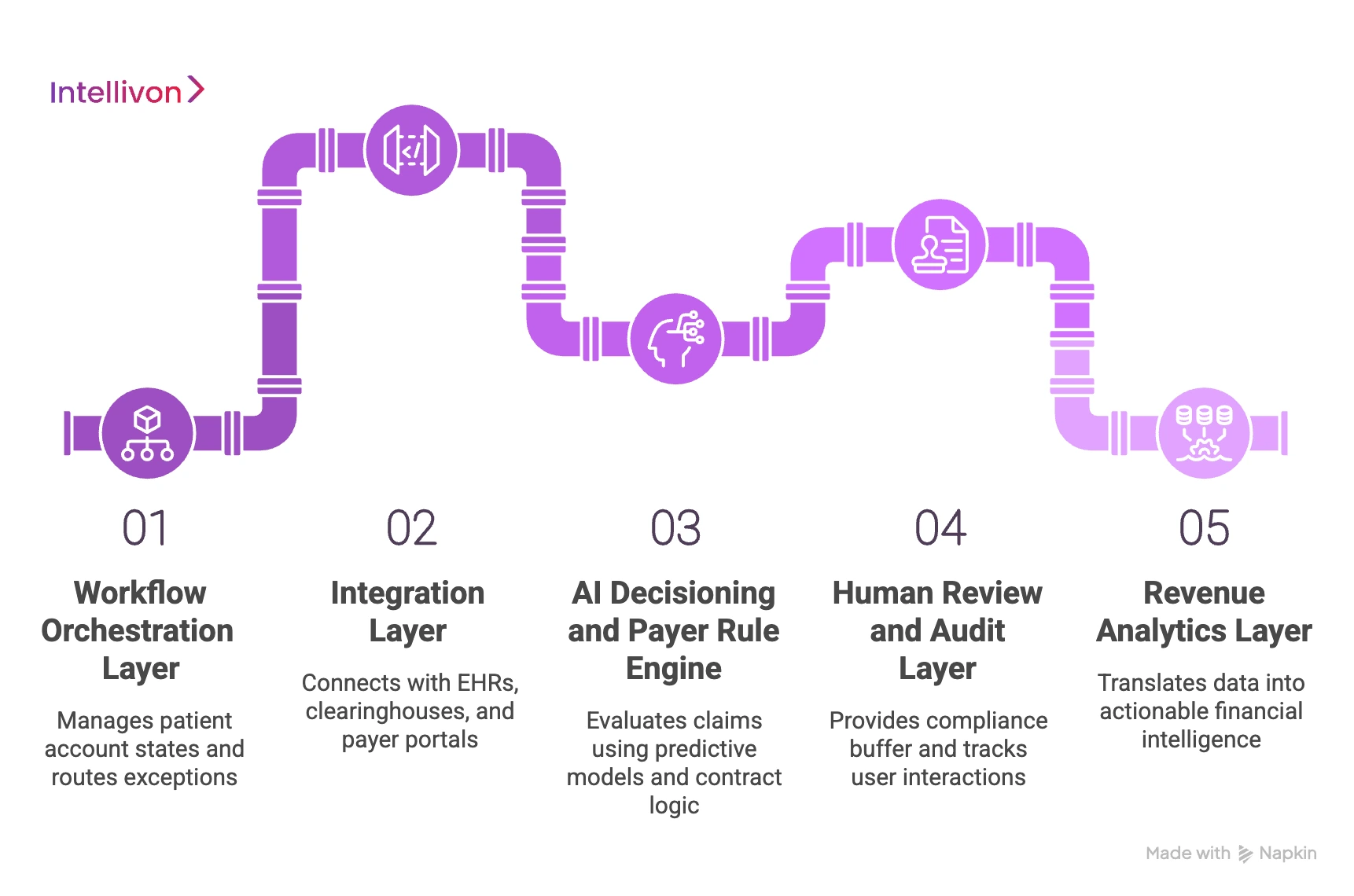
1. Workflow Orchestration Layer
The workflow orchestration layer acts as the primary traffic controller of the billing platform, managing the state of every patient account as it moves through the revenue cycle.
This microservice uses deterministic state-machine logic to monitor transaction queues and automatically route exceptions to the correct operational departments.
- Automated Case Queues: Organizes outstanding billing files into dynamic, worklist-prioritized streams based on financial value, payer deadlines, and claim complexity.
- Intelligent Task Routing: Evaluates employee performance histories to automatically assign high-complexity claim exceptions to specialized senior billing specialists.
- SLA Rule Enforcement: Monitors active processing windows to flag accounts that are approaching critical timely-filing limits or prior authorization deadlines.
- Structured Exception Handling: Isolates claims with processing errors or missing data points, keeping them out of the main transmission stream until corrected.
2. Integration Layer: EHR, HL7, FHIR R4, and EDI 837/835
The integration layer establishes bidirectional connections between your automation platform, core Electronic Health Records (EHRs), third-party clearinghouses, and direct payer portals.
This system layer translates traditional legacy clinical messaging formats into highly structured, modern database fields.
- Bidirectional EHR Connections: Syncs directly with practice management databases to update scheduling, demographics, and clinical data fields in real time.
- HL7 and FHIR Ingestion: Ingests traditional HL7 v2 messaging streams and converts them into standardized, queryable FHIR R4 JSON payloads.
- Clearinghouse Transaction Hub: Packages administrative data into compliant X12 EDI 837 claim files and parses incoming X12 EDI 835 remittance documents.
- CMS Interoperability Compliance: Deploys mandatory FHIR-based APIs for Patient Access, Provider Access, and Prior Authorization tracking in strict alignment with CMS-0057-F mandates (Source: CMS, 2026).
3. AI Decisioning and Payer Rule Engine
The AI decisioning and payer rule engine layer combines predictive machine learning models with a graph-based contract logic database to evaluate claims before submission.
This dual-engine setup allows the platform to perform advanced predictive analytics RCM assessments without relying solely on rigid, hardcoded billing rules.
- Predictive Denial Scoring: Scores every outgoing claim for rejection probability by evaluating historical payer remittance patterns against current claim attributes.
- Dynamic Payer Policy Graph: Maps individual insurance carrier rules and local coverage determinations to flag medical necessity errors prior to submission.
- Contracted Rate Validation: Cross-references active provider-payer contract terms to verify exactly what service codes are eligible for financial reimbursement.
- Automated Coding Selection: Scans clinical documentation strings to recommend highly accurate diagnostic combinations before the final claim is generated.
4. Human Review and Audit Layer
The human review and audit layer provides a necessary compliance buffer that keeps a human in the loop for low-confidence machine learning outputs.
This interface tracks employee interactions to ensure that the entire platform remains auditable and completely transparent.
- Confidence Threshold Gates: Evaluates machine learning output scores, automatically passing high-scoring files while routing low-confidence charts to manual review.
- Override Log Tracking: Records every instance where a human specialist alters an AI-generated code or eligibility flag to continuously retrain the model.
- Immutable Audit Trail: Logs all automated system actions, user edits, API calls, and payer transactions to satisfy SOC 2 Type II compliance standards.
- Escalation Priority Pathways: Triggers emergency manual reviews for high-value claims that have failed automated verification steps multiple times.
5. Revenue Analytics Layer
The CFO and revenue analytics layer translates raw transactional billing data into clear, actionable financial intelligence dashboards.
This data reporting layer allows healthcare executives to monitor system performance, track cash velocity, and identify areas of active revenue loss.
- Clean Claim Rate Tracking: Monitors the exact percentage of claims that successfully pass all payer edit checks on their very first submission.
- Days in AR Monitoring: Tracks the average time it takes for an insurance carrier to settle outstanding balances after a claim is filed.
- Revenue Leakage Alerts: Pinpoints the exact operational steps where claims are being downgraded, underpaid, or lost due to timely-filing errors.
- Denial Trend Aggregation: Groups claim rejections by specific payer codes to pinpoint root-cause registration or documentation mistakes.
Architecture gives the platform shape, but the build process determines whether it works in production.
How to Build an AI Revenue Cycle Automation Platform
Building an AI revenue cycle automation platform requires moving away from generic software engineering models and adopting a structured, healthcare-specific development framework. Successful production deployment depends on combining deterministic billing rules with adaptive machine learning pipelines that can connect directly with legacy medical systems.
By following a highly sequential engineering methodology, development teams can build scalable, compliance-ready platforms that eliminate operational errors, stop capital leakage, and lower long-term technical debt.
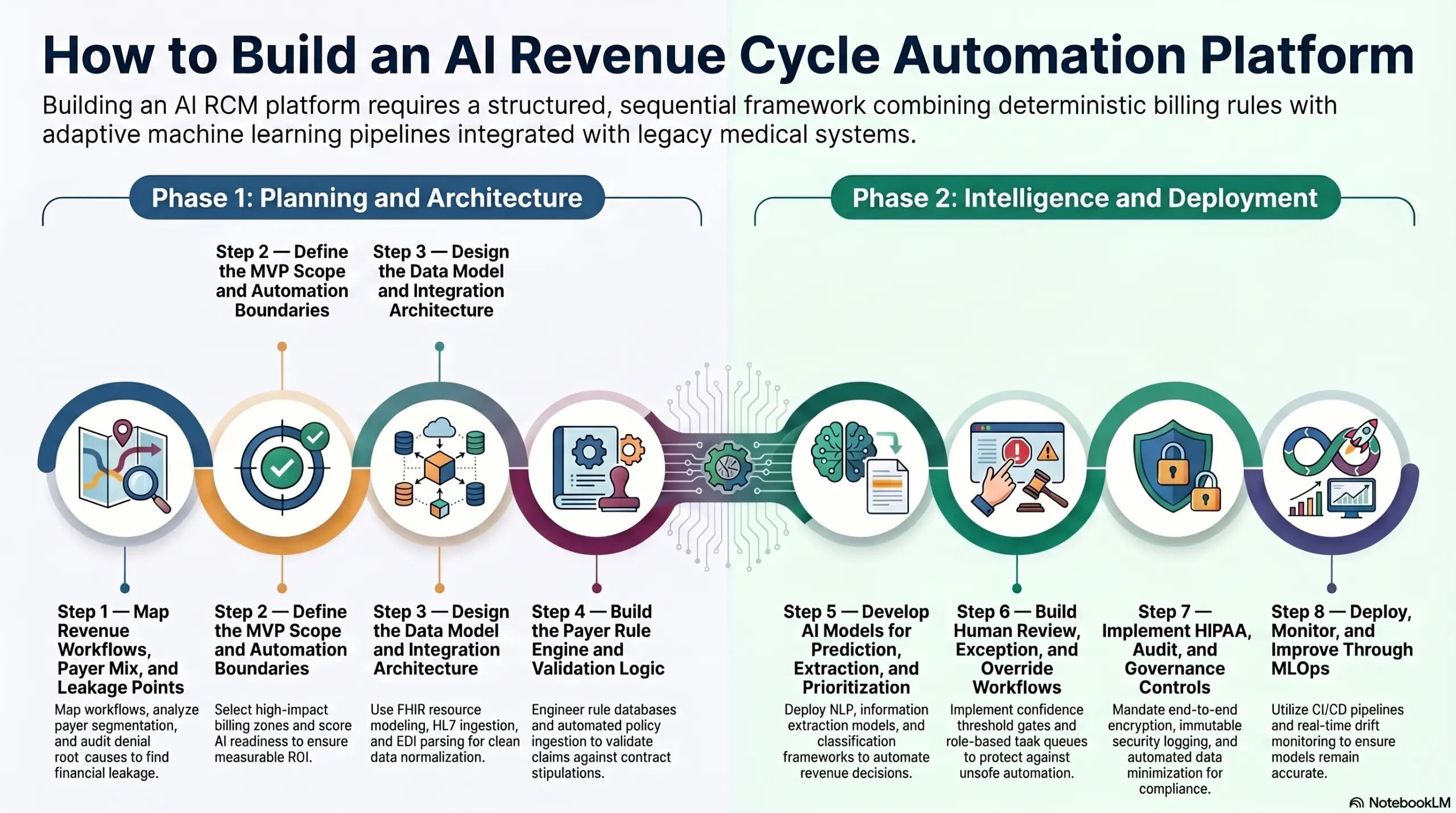
Step 1 — Map Revenue Workflows, Payer Mix, and Leakage Points
Building starts by mapping where revenue is created, delayed, denied, paid, or lost across the full RCM lifecycle. This initial planning step defines which specific billing workflows should be automated first, which commercial insurance payers create the most operational friction, and which financial performance metrics matter most for platform ROI.
- Workflow Discovery: Engineers must trace exactly how medical data moves from initial scheduling queues into active clinical documentation environments.
- Payer Segmentation: Analyze your historical billing files to group commercial carriers by clean claim thresholds, prior authorization response times, and specific edit rules.
- Denial Root-Cause Review: Audit legacy remittance advice files to categorize the common operational issues behind recursive claim cancellations.
- AR Aging Analysis: Evaluate outstanding uncollected balances to find the high-volume collections accounts that are currently approaching the timely-filing limits.
Intellivon’s approach: We systematically audit your front-end and back-end transaction data before writing any custom software code. By analyzing your historic payer remittance behaviors first, we ensure that every machine learning module is engineered to target your specific areas of maximum financial leakage.
Step 2 — Define the MVP Scope and Automation Boundaries
The Minimum Viable Product (MVP) should focus on the highest-value workflow cluster, not the entire revenue cycle at once. Most enterprise teams should start with eligibility, claim validation, denial prediction, or payment reconciliation before expanding into full end-to-end RCM automation.
- Module Selection: Choose a single high-impact billing zone—such as front-end patient registration or back-end claim scrubbing—to serve as the foundation of your initial release.
- User Flow Mapping: Design the precise software interaction boundaries that dictate when an automated background process should escalate an account to a human billing specialist.
- Data Dependency Analysis: Identify all specific clinical and administrative data elements required to run model inferences for your chosen MVP features.
- AI Readiness Scoring: Grade every prospective billing task by data availability to ensure the targeted workflow has enough clean historical training examples to sustain machine learning models.
Intellivon’s approach: We help you build a phased product roadmap focused on immediate, measurable revenue outcomes. By limiting your initial deployment scope to high-yield automation boundaries, we prove clear product ROI within months before expanding system capabilities across wider departments.
Step 3 — Design the Data Model and Integration Architecture
The platform needs a normalized data layer before AI can make reliable decisions. Patient, encounter, authorization, code, claim, payer, denial, payment, and remittance data must use consistent schemas across EHRs, clearinghouses, and finance systems.
- FHIR Resource Modeling: Map all inbound patient records, coverage definitions, and clinical encounters to standardized JSON schemas using the FHIR R4 framework.
- HL7 Message Ingestion: Establish high-speed WebSocket listeners to capture real-time ADT patient admission and SIU scheduling notification streams from legacy hospital networks.
- EDI Parsing Pipelines: Build custom data parsing engines to automatically extract structured values from raw X12 EDI 271 eligibility and EDI 835 remittance files.
- API Gateway Configuration: Deploy a secure, high-throughput gateway to manage data traffic between your machine learning microservices and third-party clearinghouses.
Intellivon’s approach: We plan your integration patterns early in the architecture phase, building high-availability data normalization pipelines that sit directly between your systems. This ensures your core AI models always ingest clean, predictable data structures regardless of the underlying EHR vendor software.
Step 4 — Build the Payer Rule Engine and Validation Logic
The payer rule engine turns policy, contract, and submission requirements into enforceable platform logic. It should validate coverage, authorization requirements, coding rules, claim completeness, modifier use, and payer-specific submission rules before claims reach clearinghouses.
- Rules Database Design: Engineer a high-performance graph database that maps current clinical billing codes to specific commercial insurance contract stipulations.
- Version Control Workflows: Implement strict branch tracking for all validation logic to allow instant system updates when a payer alters their medical coverage rules.
- Payer Policy Ingestion: Build automated monitoring tools that scan insurer documentation changes to flag updated pre-authorization requirements.
- Exception Rule Testing: Create an isolated simulation pipeline to test new billing rule alterations against historic claims before activating them in production.
Intellivon’s approach: We combine deterministic payer rule graphs with predictive machine learning risk scores to create a comprehensive validation stack. This hybrid architecture catches formatting errors through clear, hardcoded filters while simultaneously using predictive analytics to identify subtle contextual denial risks.
Step 5 — Develop AI Models for Prediction, Extraction, and Prioritization
AI models should support specific revenue decisions, not operate as vague automation features. The core models usually include document extraction, coding support, denial prediction, payment variance detection, AR prioritization, and workflow routing.
- Natural Language Processing: Deploy clinical NLP architectures fine-tuned on medical text to parse unstructured provider notes and operative progress summaries.
- Information Extraction Models: Utilize specialized Named Entity Recognition (NER) models to pull specific plan numbers, effective dates, and policy limits from scanned documents.
- Classification Frameworks: Train supervised classification networks to predict claim rejection risks by evaluating historic transaction sequences.
- LLM Summary Pipelines: Use secure Large Language Models to read hundreds of pages of complex payer denial letters and extract the exact actionable refusal reasons.
Intellivon’s approach: We train specialized, domain-specific machine learning models that deliver clear confidence metrics and explainable data features for every automated inference. This transparent approach ensures your team can easily trace the exact data variables that drove a particular billing decision.
Step 6 — Build Human Review, Exception, and Override Workflows
Human review protects the platform from unsafe automation in complex revenue decisions. Every low-confidence prediction, unusual payer response, high-value claim, disputed denial, and underpayment case should move into a clear exception workflow.
- Confidence Threshold Gates: Configure the system to automatically process high-scoring data files while instantly rerouting low-confidence charts to manual queues.
- Role-Based Task Queues: Segment exception worklists by specialization to ensure complex medical charts are handled by experienced senior coding experts.
- Override Log Tracking: Build an internal data tracking pipeline that logs every instance where a human specialist changes an AI-suggested code.
- Escalation Priority Pathways: Implement logic to automatically prioritize high-value claims that are approaching strict timely-filing deadlines.
Intellivon’s approach: We engineer unified, intuitive exception review interfaces directly into the platform architecture. By presenting clear AI recommendations alongside direct source documentation, we help your existing billing and coding teams process exception queues up to ten times faster.
Step 7 — Implement HIPAA, Audit, and Governance Controls
HIPAA controls must be engineered into the platform before production deployment. Revenue automation systems process ePHI, claim data, payer information, clinical documentation, and payment records, so access, auditability, encryption, and monitoring cannot be added later.
- Role-Based Access Governance: Restrict sensitive patient data fields using granular cryptographic access keys tied directly to verified corporate identities.
- End-to-End Encryption: Mandate TLS 1.3 encryption protocols for all data in transit alongside AES-256 storage encryption for all database volumes.
- Immutable Security Logging: Generate permanent, time-stamped system logs for every single transaction, data query, and record modification to satisfy SOC 2 Type II audit requirements.
- Automated Data Minimization: Sanitize clinical text fields by stripping out unneeded patient identifiers before sending payloads to machine learning inference instances.
Under the updated HIPAA Security Rule frameworks, healthcare business associates are required to enforce strict administrative, physical, and technical safeguards for all electronic protected health information (Source: HHS, 2026). Technical controls like multifactor authentication and network micro-segmentation are mandatory requirements rather than optional implementations.
Intellivon’s approach: We treat data security, user auditability, and regulatory compliance as foundational architectural requirements rather than an afterthought. We implement automated PHI masking and zero-trust data access patterns straight into your core data pipelines to ensure the platform passes enterprise compliance audits.
Step 8 — Deploy, Monitor, and Improve Through MLOps
Deployment is not the end of AI RCM development. The platform needs MLOps, model drift monitoring, payer-rule updates, performance dashboards, exception review, and release governance to stay accurate as payer behavior changes.
- Automated CI/CD Pipelines: Build isolated integration and deployment tracks to safely roll out validation logic upgrades without interrupting active billing operations.
- Model Registry Management: Track the performance, lineage, and training weights of every active machine learning architecture deployed across your network.
- Real-Time Drift Monitoring: Deploy continuous statistical tracking tools to spot when shifting payer denial patterns begin to degrade model prediction accuracy.
- Automated Rollback Safeguards: Configure instant, safe system recovery workflows to restore previous stable software versions if a new model update displays erratic behavior.
Intellivon’s approach: We build complete MLOps tracking suites straight into your custom platform roadmap from day one. This continuous monitoring framework ensures that your deployed machine learning models remain accurate, adaptive, and fully aligned with shifting industry billing rules over the years of production operation.
AI Models Used in Custom AI RCM Software
Custom AI revenue cycle management software uses a specialized mix of machine learning, NLP, document intelligence, LLMs, and predictive analytics.
This multi-model ensemble ensures that every automated decision is mathematically validated, transparent, and bounded by your existing payer contract logic.
A Specialized Ensemble for End-to-End Billing Tasks
Deploying distinct machine learning models across specific billing stages prevents a single model failure from disrupting your broader financial ecosystem.
Each architecture handles a narrow, dedicated transaction data type to ensure maximum speed and processing accuracy.
- OCR and Document AI: Extracts structured data fields from unstructured document types, including scanned Explanation of Benefits (EOBs), electronic referrals, paper intake forms, and physical insurance cards.
- Clinical NLP: Scans unstructured physician progress notes, operative summaries, and EHR discharge files to extract active diagnoses and verify medical necessity compliance.
- Autonomous Coding Support: Generates real-time validation suggestions for ICD-10-CM, CPT, and HCPCS Level II code combinations based on the extracted clinical text.
- Predictive Denial Models: Scores outgoing insurance claims for rejection risks prior to submission by evaluating current billing configurations against historical carrier remittance patterns.
- Underpayment Detection Models: Compares settled insurance payout amounts directly against digitized payer contract rate sheets to spot systemic payment variances and shortfalls.
- AR Prioritization Models: Sorts outstanding uncollected claims by cash value, historical probability of collection, and upcoming timely-filing deadlines.
- Agentic AI Workflows: Deploys goal-directed autonomous agents that continuously track claim statuses, verify clearinghouse receipts, and execute structured follow-up tasks without manual human prompts.
- Large Language Models (LLMs): Reads dense insurance denial letters to generate clear clinical summaries, populate missing administrative data points, and draft targeted appeal arguments.
Decision Support Over Labor Replacement
When developing custom billing software, enterprise technology teams must position machine learning tools as decision support and workflow acceleration engines. Attempting to completely automate human billers out of the loop creates immense operational risk during sudden payer policy shifts.
Medical billing professionals frequently highlight this risk on practitioner forums, asking whether newly deployed AI tools actually save time or simply create massive data rework around complex coordination of benefits (COB), secondary claims, and carrier-specific rule adjustments.
HIPAA-Compliant Revenue Cycle Automation Software Controls
Enforcing HIPAA-compliant revenue cycle automation software controls requires engineering strict data-handling practices directly into both your application layer and your active machine learning pipelines.
Because an AI revenue cycle automation platform continuously processes sensitive electronic protected health information (ePHI), compliance cannot function as a surface-level software patch. Security architects must design technical safeguards that protect patient data throughout the entire lifecycle of ingestion, model inference, human review, and long-term storage.
1. Core Safeguards for the Application and Machine Learning Layers
To safely process financial and clinical data streams, development teams must deploy a multi-layered security framework that satisfies the stringent administrative and technical requirements of the HIPAA Security Rule.
These foundational guardrails ensure complete data confidentiality and system traceability across all automated workflows.
- Role-Based Access Control (RBAC): Restricts data visibility by enforcing the principle of least privilege, ensuring employees access only the specific ePHI fields needed for their unique billing roles.
- End-to-End Cryptographic Encryption: Implements mandatory TLS 1.3 encryption protocols for all data transfers in transit alongside robust AES-256 storage encryption for all database volumes.
- Immutable Security Audit Logs: Generates permanent, time-stamped system logs tracking every user login, data query, API transaction, and record modification to satisfy SOC 2 Type II audit standards.
- Automated Input/Output Logging: Records all text payloads sent to machine learning models along with the corresponding model predictions to preserve a clear lineage for every automated billing decision.
2. Minimizing Risk Through Data Redaction and Governance Structures
Managing enterprise-grade healthcare automation requires establishing rigorous data minimization pipelines and formal legal agreements before exposing systems to live clinical data.
These protective structural layers isolate production environments and shield your organization from catastrophic data breach liabilities.
- Automated Data Redaction: Runs specialized named entity recognition (NER) models to strip out direct patient identifiers from clinical texts before data reaches machine learning training arrays.
- Human-in-the-Loop Safeguards: Routes all low-confidence model predictions and high-value financial claim exceptions to secure human review queues rather than allowing autonomous submission.
- Business Associate Agreements (BAAs): Establish signed BAAs with all underlying cloud hosting infrastructure firms, third-party API networks, and external clearinghouse services.
- Access Review Workflows: Deploys automated scheduling scripts that perform routine user access reviews and instantly terminate network credentials for offboarded employees.
For a deeper breakdown of compliance architecture, see our guide on How to Build a HIPAA-Compliant AI RCM Platform.
Implementing these comprehensive security controls provides a resilient foundation that shields sensitive patient details from exposure while maintaining peak transaction speed.
Build vs Buy AI RCM Platform: How to Make the Right Decision
Build an AI RCM platform when workflow ownership, payer-specific logic, integration depth, data control, or product differentiation matters. Buy when you need faster deployment, standard workflows, limited customization, and vendor-managed compliance. Most enterprise teams use a hybrid path before committing fully.
The Enterprise Strategic Decision Matrix
To protect your software development capital and maximize long-term return on investment, engineering product leads and hospital CFOs must evaluate their specific infrastructure needs.
This comparative decision framework matches your organizational profile to the correct software procurement model.
| Choose Build When | Choose Buy When |
| You operate across multiple complex clinical specialties with highly variable payer mixes. | Your financial clearance and back-end claims workflows follow standardized regional processing lines. |
| Your long-term business model requires complete ownership of your platform’s intellectual property. | Your operational strategy prioritizes immediate market deployment speed over direct system control. |
| You want to train, deploy, and refine custom machine learning models on your own historical data. | Standard off-the-shelf vendor models are sufficient to meet your basic automated billing needs. |
| You require deep, bidirectional integration with highly proprietary EHR, EDI, and FHIR databases. | Existing vendor cloud application connections successfully cover your entire current software stack. |
| You need to generate unique software features to drive differentiated SaaS product revenue. | Your internal motivation is focused solely on improving baseline back-office staff efficiency metrics. |
Selecting the correct procurement model ensures that your technology investment actively reduces your cost-to-collect without introducing system architecture bottlenecks.
Once the custom build path makes clear strategic sense, the development budget must be mapped across distinct, milestone-driven engineering phases.
Top Examples of AI Revenue Cycle Automation Platforms
An AI revenue cycle automation platform is not limited to a single administrative task like claim scrubbing or payment posting. The strongest enterprise systems automate interconnected workflows across patient access, clinical coding, claims transmission, prior authorization tracking, and back-end denial appeals.
By deploying multi-model ensembles and containerized automation layers, these market leaders demonstrate how advanced machine learning models, deterministic rule frameworks, and automated system scripts scale to support high-volume enterprise healthcare billing operations.
1. UiPath
UiPath demonstrates how enterprise robotic process automation (RPA) combined with Document AI can orchestrate high-volume healthcare administration and transactional revenue cycle workflows.
Its specialized healthcare automation suite provides structural support for cross-system document extraction, clearinghouse communication loops, automated insurance appeals, and back-office financial reconciliation.
- Enterprise Administrative Scale: Currently deployed across 75% of the top 100 U.S. health systems and utilized by more than 400 healthcare organizations to eliminate manual data entry.
- Quantifiable Operational Velocity: A large-scale deployment by Omega Healthcare saved more than 15,000 employee operational hours per month while reducing documentation cycles by 40%.
- Processing Precision Outcomes: Achieved a 50% acceleration in transaction turnaround times alongside a verified 99.5% accuracy rate in automated document processing workflows.
2. AKASA
AKASA serves as an ideal example of an AI-native revenue cycle operating infrastructure built specifically for the clinical environment.
Its core platform architecture unifies generative AI frameworks with dedicated financial data models to automate complex front-end and mid-cycle tasks, including prior authorization monitoring, clinical documentation improvement (CDI), and compliant medical coding support.
- Native Generative Architectures: Uses deep generative AI models trained specifically on complex billing rules and clinical text strings rather than generic, general-purpose LLM interfaces.
- Proactive Authorization Tracking: Features an intelligent prior authorization microservice that executes background status inquiries and auto-populates required medical necessity forms.
- Front-End Delay Mitigation: Target-scans incoming registration entries to capture approval tokens days before services are rendered, eliminating downstream back-end delays.
3. Waystar n
Waystar represents an enterprise-grade execution of automated financial clearance and payment integrity tracking within a unified cloud environment.
The platform focuses heavily on processing efficiency, predictive claims analytics, automated denial remediation, advanced Medicare workflows, and patient out-of-pocket financial responsibility modeling.
- Predictive Submission Analytics: Evaluates outgoing claims data streams against a dense library of historical remittance files to assign clear payment probability scores prior to submission.
- Automated Reconsideration Generation: Uses specialized text extraction models to read incoming payer rejection notifications and auto-populate precise, contract-backed appeal arguments.
- Front-End Denial Prevention: Embeds real-time eligibility and authorization accuracy checking directly into patient check-in screens to catch errors before data moves to billing departments.
4. Notable
Notable highlights the critical technical relationship between front-end patient intake precision and back-end claims collection performance.
By deploying specialized digital AI agents at the point of scheduling and registration, the platform automates demographic verification, co-pay estimation, real-time eligibility parsing, and prior authorization routing.
- Front-End Error Interception: Instructs autonomous AI agents to scan scanned insurance card images and instantly match the extraction targets against active payer coverage definitions.
- Patient Responsibility Calculation: Computes accurate out-of-pocket patient cost estimates during intake to minimize backend bad debt and reduce payment friction.
- Downstream Rejection Avoidance: Mitigates the structural registration errors that account for a high percentage of subsequent back-end claim rejections and timely-filing delays.
5. Commure
Commure represents the cutting edge of agentic healthcare automation, showcasing the industry transition from passive text copilots to goal-directed autonomous systems.
Its enterprise-grade infrastructure operates across a multi-EHR footprint to execute billing tracking, clinical documentation, and practice management actions independent of human prompts
- High-Scale Autonomous Execution: Completes over 85% of complex revenue cycle and payment tracking operations entirely without manual human intervention.
- Massive Enterprise Footprint: Actively deployed across more than 500 enterprise healthcare networks and 3,000 distinct clinical care locations nationwide.
- Bidirectional Integration Density: Integrates natively with over 60 distinct Electronic Health Record systems to process tens of billions of dollars in annual claims.
Evaluating these dominant enterprise platforms shows that successful healthcare automation requires combining deep data extraction pipelines, dynamic payer rule engines, and reliable exception review frameworks.
For software engineers and technology leaders designing an internal system, the architectural mandate is clear: your platform must unify the complete end-to-end financial workflow rather than automating isolated back-office tasks.
Why Build AI-Powered RCM Systems With Intellivon
Intellivon builds AI-powered RCM systems around real revenue workflows, secure healthcare integrations, payer-rule logic, explainable AI, and measurable operating outcomes.
The goal is to build a controlled revenue infrastructure layer that healthcare teams can trust in production.
A. Help You Define The Right RCM Automation Scope
A successful AI RCM build starts with the right scope. Intellivon helps healthcare teams define whether they need an MVP, an internal automation platform, or a SaaS-ready product for multiple clients.
This includes workflow prioritization across front-end, mid-cycle, and back-end revenue operations. We map eligibility verification, prior authorization, coding support, claim scrubbing, denial prevention, payment posting, and AR follow-up based on where automation can create a measurable ROI first.
B. Design The Platform Architecture Before Development
AI RCM platforms need a strong architecture before development begins. Intellivon plans the workflow engine, data model, integration layer, audit layer, analytics layer, and user roles before writing production code.
This includes FHIR R4 and HL7 strategy, EHR connectivity, EDI 837/835 processing, clearinghouse integrations, payer workflows, and secure data exchange. As a result, the platform does not become another disconnected tool inside the revenue stack.
C. Build AI Around Reviewable Revenue Decisions
RCM AI should support decisions that teams can review, explain, and improve. Intellivon builds AI workflows for denial prediction, claim scrubbing, coding support, payment variance detection, underpayment alerts, and revenue worklist prioritization.
Each workflow includes confidence scoring, human review queues, exception handling, and audit trails. This helps revenue teams act faster without losing control over high-value claims, payer disputes, or compliance-sensitive decisions.
D. Keep Compliance And MLOps In The Build Plan
AI-powered RCM systems process PHI, payer data, claim records, clinical documentation, and payment information. Intellivon builds HIPAA controls, secure PHI handling, role-based access, audit logs, model monitoring, and model drift checks into the platform plan from the beginning.
Payer rules, denial patterns, and revenue workflows change often. So, the platform also needs MLOps, rule updates, and performance monitoring after launch.
Plan Your AI RCM Platform Roadmap With Intellivon.
Conclusion
An AI revenue cycle automation platform is not a superficial chatbot, isolated claims scrubber, or passive management dashboard. It functions as a deeply integrated financial infrastructure system that unifies front-end registration, mid-cycle clinical coding, back-end collections, dynamic payer logic, and automated compliance controls into a single data fabric.
Deploying this architecture allows healthcare organizations to secure their cash flows, minimize costly administrative burdens, and eliminate structural payment leakage across all care facilities.
Things To Know About AI Revenue Cycle Automation Platforms
Q3. How much does an AI revenue cycle automation platform cost?
A1. An AI revenue cycle automation platform usually costs $80,000 to $350,000+ to build. A focused MVP sits near the lower range, while enterprise systems with EHR integration, FHIR R4, EDI 837/835, denial prediction, payment posting, HIPAA controls, and SaaS readiness move toward the higher range.
Q2. How long does AI RCM platform development take?
A2. AI RCM platform development usually takes 4–6 months for an MVP, 7–12 months for an enterprise platform, and 12–18 months for a commercial SaaS product. The biggest timeline drivers are EHR access, payer integrations, data quality, AI validation, and compliance review.
Q3. Can AI revenue cycle automation software be HIPAA compliant?
A3. Yes. AI revenue cycle automation software can be HIPAA compliant when it includes administrative, physical, and technical safeguards, secure PHI workflows, access controls, audit logs, encryption, human review, and vendor governance. HHS states the HIPAA Security Rule requires safeguards that protect ePHI confidentiality, integrity, and availability.
Q4. What AI models are required for custom AI revenue cycle management software?
A4. Custom AI revenue cycle management software usually needs OCR, NLP, classification models, denial prediction, coding support, payment variance detection, AR prioritization, and LLM-assisted summarization. It should also include deterministic payer rules because AI alone should not decide every claim, denial, or payment case.
Q5. Can agentic AI healthcare workflows handle RCM without human review?
A5. No. Agentic AI healthcare workflows can handle structured follow-ups, claim status checks, task routing, and documentation collection, but high-value claims, payer disputes, coding uncertainty, and appeal decisions still need human review.



