GLP-1 did not enter healthcare through a grand strategy. It came in quietly, driven by increasing prescriptions, rising patient demand, and telehealth programs that expanded faster than they were updated. Initially, a virtual consult and a prescription seemed enough. As demand grew, the shortcomings began to appear.
GLP-1 telehealth platforms have established a system that changes how care is delivered and how digital platforms respond under stress. A genuine GLP-1 telehealth platform determines who qualifies for treatment, how therapy progresses, how exceptions are managed, and how outcomes are tracked over time. Platforms like Found Health achieved scale by treating GLP-1 as a regulated clinical infrastructure from the beginning, rather than just adding features on top of telehealth.
At Intellivon, we collaborate with healthcare organizations dealing with this shift in real time. Our teams create GLP-1 platforms where clinical governance, automation, and enterprise systems work together seamlessly, rather than as separate tools. In this blog, we explain how we build these platforms from the ground up, where enterprises encounter difficulties after the platform launch, and how we solve them while maintaining clinical and financial control.

Why Invest In GLP-1 Telehealth Platforms Right Now
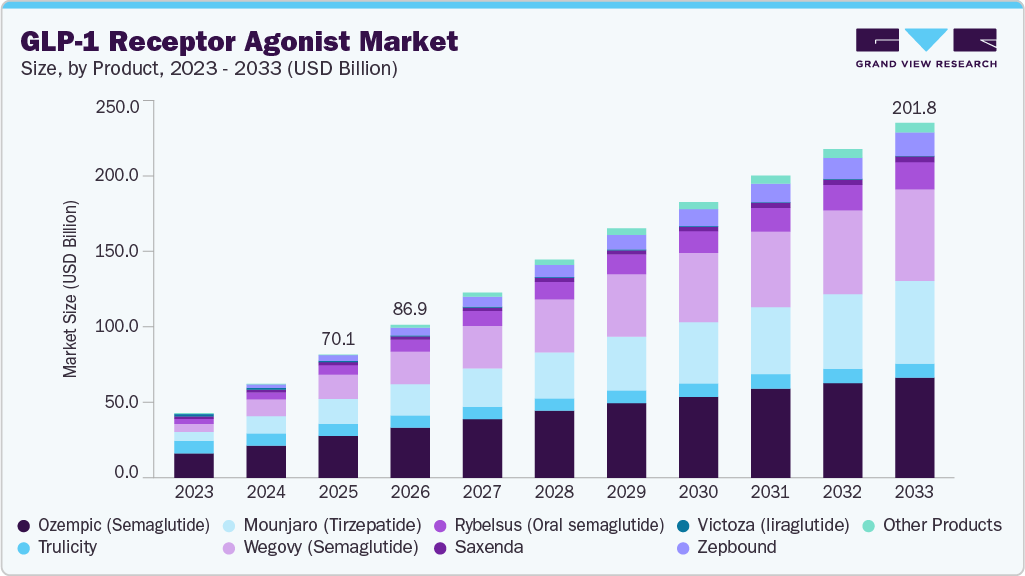
This shift is also reflected in the scale of investment flowing into GLP-1 therapies. The global market for GLP-1 receptor agonists has already crossed the $70 billion mark in 2025 and is expected to more than triple over the next decade, reaching well over $200 billion by the early 2030s.
Market Expansion Signals
- Obesity-focused GLP-1 revenue is expected to grow from $8B in 2025 to nearly $40B by 2030, with projections crossing $65B by 2035, representing an 8× expansion over a decade.
- This growth is being driven by a steady pipeline of new formulations, broader obesity indications, and rising long-term adoption.
Demand and Clinical Momentum
- Nearly 900 million adults globally live with obesity, positioning GLP-1s as a core component of emerging obesity care strategies.
- Obesity is projected to cost the global economy ~$2.7T in lost productivity by 2050, increasing pressure on healthcare systems to intervene earlier.
- GLP-1 prescriptions grew at an estimated ~38% annually between 2022 and 2024, supported by evidence of 15–20% sustained weight loss and reduced cardiovascular risk.
Employer and Payer Economics
- Economic modeling suggests broad GLP-1 coverage could increase employer health premiums by 5–14% at current drug prices, depending on eligibility, adherence, and cost-sharing design.
- Scenario analyses indicate that if monthly GLP-1 costs fall toward $200, premium impact could moderate to 1–4%, accelerating payer and employer adoption.
- These dynamics explain growing interest in utilization controls, outcomes-linked reimbursement, and care management overlays.
Strategic and Commercial Outlook
- Financial models project global GLP-1 sales across obesity and diabetes reaching $100–140B by 2030, with continued double-digit growth beyond that point.
- Expansion is expected to accelerate with oral formulations, dual and triple agonists, and new therapeutic indications, including NASH, sleep apnea, cardiovascular disease, and neurodegenerative conditions.
As a result, life sciences, payers, and employers are rethinking delivery models, moving toward integrated virtual care, outcomes-based contracts, and tighter utilization management.
What is the GLP-1 Telehealth Platform Found Health?
Found Health started as a virtual weight-care provider and quickly became one of the most visible GLP-1 telehealth platforms in the U.S., delivering tailored clinical care rather than just scripted medications. It combines licensed medical oversight with ongoing coaching and real-world behavior support, so patients aren’t left alone after a prescription.
One of its distinctive features is insurance navigation. Found works with carriers and conducts coverage checks to reduce out-of-pocket costs, helping patients access brand-name GLP-1 medications more affordably. The platform offers a broad toolkit of prescription options, including GLP-1s and other metabolic agents, with tailored treatment plans and app-based tracking.
Clinically, Found has treated hundreds of thousands of users and reported strong engagement and outcomes in its internal follow-up data. For enterprise leaders evaluating digital care, its model shows how structured clinical workflows and insurance integration can translate high demand into measurable revenue and sustained engagement.
Difference Between Weight-Loss Apps and GLP-1 Care Platforms
At first glance, consumer weight-loss apps and GLP-1 telehealth platforms can look similar. However, the difference lies in how risk is handled, how care is governed, and how accountability is enforced.
For healthcare enterprises, confusing the two leads to operational, legal, and financial exposure.
Consumer Apps vs Regulated GLP-1 Platforms
| Aspect | Consumer Weight-Loss Apps | Regulated GLP-1 Care Platforms |
| Primary purpose | Habit tracking and lifestyle motivation | Clinical delivery of GLP-1 therapy |
| Medical oversight | Minimal or none | Licensed providers with defined accountability |
| Prescribing authority | Not applicable | Governed prescribing and titration workflows |
| Side-effect handling | Self-reported, non-clinical | Monitored, triaged, and escalated clinically |
| Compliance posture | Wellness or lifestyle category | HIPAA-compliant regulated healthcare |
| Pharmacy integration | None or informational | E-prescribing, fulfillment, and refill control |
| Revenue model | Low-cost subscriptions or ads | Clinical subscriptions and care-based revenue |
| Risk exposure | Limited product risk | High clinical, regulatory, and financial risk |
Consumer apps can succeed with loose controls because the downside is limited. Regulated GLP-1 platforms do not have that luxury.
This is why successful GLP-1 platforms are designed as clinical systems, and not as engagement products. They prioritize governance, automation, and observability over surface-level experience.
What Revenue and Business Models Make Found Successful?
Found’s success is not tied to a single pricing trick or medication wave. It comes from how the platform aligns clinical delivery, user commitment, and predictable revenue into a repeatable operating model. Instead of treating GLP-1 as a transactional service, Found built its business around continuity of care and long-term engagement.
That distinction matters. Enterprises that struggle with GLP-1 often do so because revenue and care delivery are misaligned. Found avoids that by designing both together.
Business Models of Found Health
Found operates as a virtual care company first, not a prescription marketplace. Its business model centers on managing obesity as an ongoing clinical condition rather than a short-term intervention.
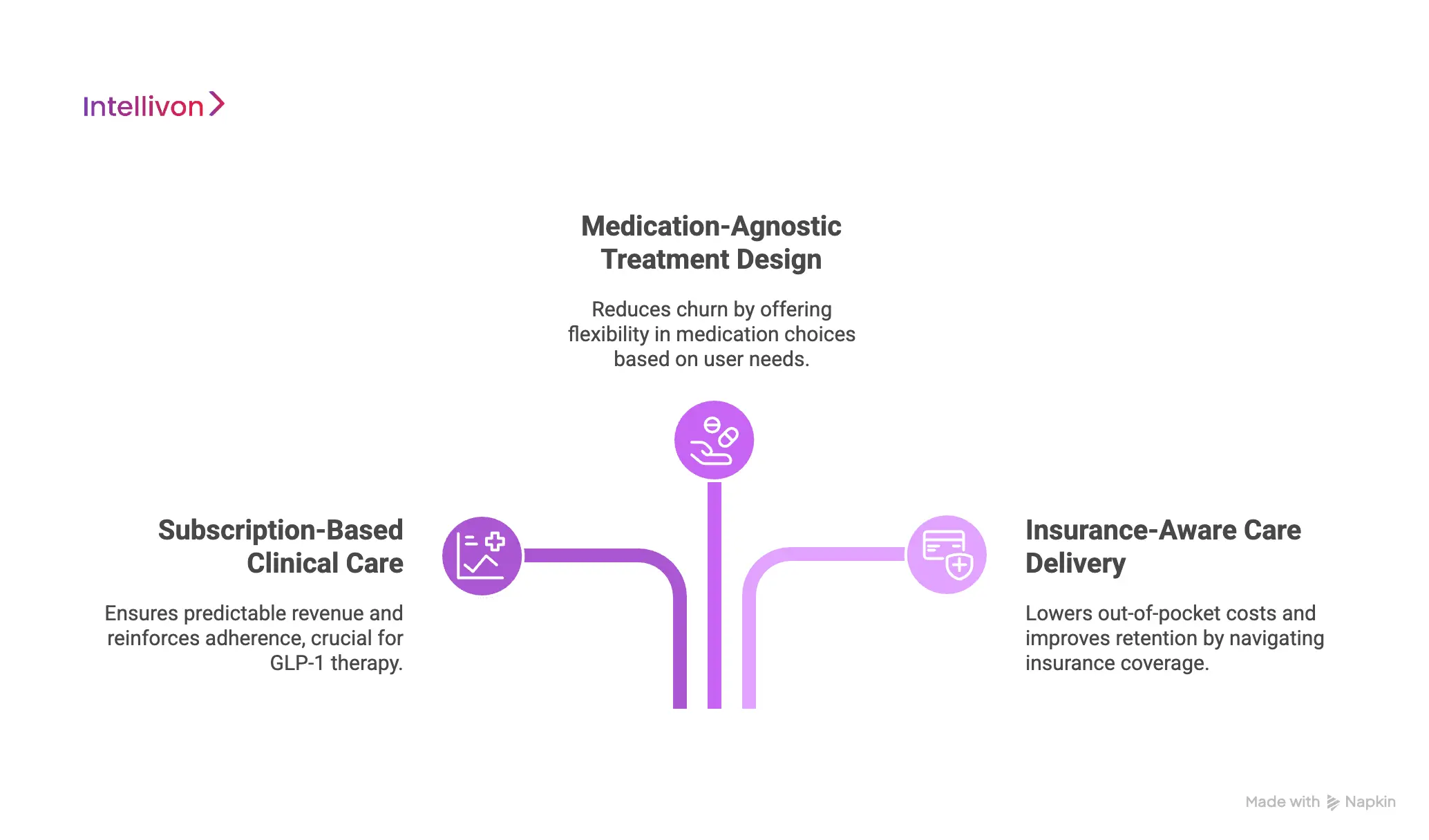
1. Subscription-Based Clinical Care
Found charges a recurring membership fee that covers medical oversight, care coordination, and ongoing support. This creates predictable revenue while reinforcing adherence and follow-up, which are essential in GLP-1 therapy.
2. Medication-Agnostic Treatment Design
Rather than locking users into a single GLP-1 drug, Found positions itself as medication-flexible. Clinicians can prescribe GLP-1s or alternative metabolic therapies based on eligibility, tolerance, and coverage. This reduces churn driven by supply shortages or affordability issues.
3. Insurance-Aware Care Delivery
Found actively incorporates insurance checks and coverage navigation into its workflows. This lowers out-of-pocket friction for users and improves retention, while protecting the platform from revenue volatility caused by sudden cost barriers.
The business model keeps users engaged beyond the initial prescription and aligns clinical outcomes with financial sustainability.
Revenue Models of Found Health
Found’s revenue model is layered, which helps it scale without relying on a single income stream.
1. Recurring Membership Revenue
Monthly subscription fees form the foundation. This revenue is stable, forecastable, and less sensitive to short-term prescribing fluctuations.
2. Clinical Services Revenue
Provider consultations, follow-ups, and care adjustments are embedded into the platform’s value, supporting clinical revenue tied directly to regulated care delivery.
3. Medication-Driven Lifetime Value Expansion
While Found does not bundle medication costs into its subscription, GLP-1 usage significantly increases user lifetime value through longer engagement cycles and higher willingness to stay enrolled.
Revenue grows with engagement quality and not only volume. That makes the model more resilient as scrutiny around GLP-1 pricing and utilization increases.
Found’s success shows that GLP-1 platforms scale best when revenue models reinforce responsible care delivery. Subscription-led design, medication flexibility, and insurance-aware workflows turn high demand into durable returns.
GLP-1 Based Telehealth Platforms Generate $190M in One Quarter
GLP-1 programs are no longer experimental initiatives. For healthcare enterprises running telehealth platforms, they have become a serious revenue driver.
When deployed with the right clinical, operational, and compliance infrastructure, GLP-1 platforms are now capable of generating nine-figure quarterly revenue. Recent earnings disclosures and claims-based studies offer clear, primary evidence of this shift.
They also reveal a critical truth, that GLP-1 profitability depends far more on platform design than on demand alone.
1. Public Operator Data Confirms GLP-1 as a Revenue Multiplier
In Q2 2025, Hims & Hers Health reported that its GLP-1 offerings generated approximately $190 million in online revenue in a single quarter. In the first half of the year, GLP-1 revenue crossed $420 million.
For enterprise leaders, this data confirms three important realities:
- GLP-1 programs can scale rapidly within telehealth delivery models
- Revenue impact is visible at the P&L level, not just engagement metrics
- GLP-1 can become a core growth engine, not a supporting service
2. GLP-1 Programs Increase ARPU
Revenue growth is only part of the story. GLP-1 programs also change unit economics.
Hims & Hers disclosed that monthly online revenue per average subscriber increased from $57 to $74 year over year, with GLP-1 adoption cited as a key driver.
This ARPU lift has direct ROI implications:
- Higher ARPU supports higher customer acquisition spend
- Subscription-based GLP-1 care creates predictable recurring revenue
- Longer clinical engagement increases lifetime value per patient
For enterprise telehealth platforms, GLP-1 monetization extends far beyond one-time consultations.
3. Clinical GLP-1 Subscriptions Create a New Revenue Line
In FY2024, WeightWatchers reported $78.0 million in clinical subscription revenue, up from $30.5 million in FY2023. GLP-1 programs were a primary driver. In Q4 2024 alone, clinical subscriptions reached $20.5 million, representing 57.9% year-over-year growth.
This demonstrates that GLP-1 platforms can:
- Create standalone clinical subscription revenue streams
- Offset declines in legacy wellness or engagement products
- Anchor monetization around regulated healthcare delivery
Why ROI Depends on Platform Design
Revenue potential alone does not guarantee profitability. Primary payer data highlights the risk of poor execution.
Prime Therapeutics reported that without strict utilization controls, new GLP-1 initiators increased total cost of care by $7,132 in the first year, with no immediate medical offset.
The implication is clear that the GLP-1 profitability must be engineered.
Platforms that perform well financially tend to:
- Enforce eligibility and prescribing rigor
- Monitor adherence and persistence continuously
- Automate prior authorization and coverage workflow
- Detect misuse and early disengagement signals
This is why platforms like Found Health are moving beyond isolated GLP-1 features. They are investing in full-stack platforms with governance, automation, and observability designed from day one.
Integrating GLP-1 Platforms Into Enterprise Health Systems
Integration is where most GLP-1 initiatives either mature into enterprise platforms or quietly stall. On paper, adding GLP-1 care to an existing health system looks straightforward. In practice, it touches nearly every operational layer, from clinical systems to finance and compliance.
A GLP-1 telehealth platform cannot operate in isolation for long. To scale responsibly, it must fit into the enterprise health ecosystem rather than sit alongside it.
Why integration matters more than features
Enterprises already run complex environments, where EHRs manage clinical records, pharmacy systems handle fulfillment, payer systems control authorization and reimbursement, and identity platforms govern access and auditability.
If a GLP-1 platform does not integrate cleanly into these systems, teams are forced into manual workarounds. That leads to delayed care, higher operational costs, and compliance risk. Over time, leadership loses visibility into what the platform is actually doing.
Core Systems GLP-1 Platform Must Integrate With
Most enterprise GLP-1 deployments require tight integration across a few critical domains:
- Electronic Health Records (EHRs) to sync patient history, diagnoses, labs, and care notes
- Pharmacy and fulfillment systems to manage prescribing, refills, and medication status
- Insurance and prior authorization systems to validate coverage and reduce manual denials
- Identity and access management to ensure secure, role-based clinical access
- Analytics and reporting layers to track outcomes, utilization, and financial performance
Each integration reduces friction. Together, they determine whether the platform feels native or bolted on.
How Integration Should Look
- Successful organizations treat integration as an architectural decision, and not a connector checklist.
- Data needs to move reliably, securely, and in near real time.
- Failures must be visible, not silent.
- Clinical workflows should not break when one system slows down.
This is why many enterprises move toward API-first, event-driven architectures for GLP-1 platforms. It allows systems to communicate without hard dependencies and makes future expansion easier.
Where Intellivon fits in
At Intellivon, we design GLP-1 platforms to integrate into enterprise health systems from day one. Our teams focus on interoperability, data governance, and resilience, so GLP-1 care operates as part of the broader healthcare infrastructure.
The result is a platform that scales with the organization, supports compliance, and gives leadership clear visibility into clinical and financial performance.
Platform Architecture for GLP-1 Telehealth Platform Like Found
A GLP-1 telehealth platform that scales does not rely on a single system. It operates as a layered architecture, where each layer has a clear responsibility, and failure in one layer does not collapse the whole platform. This is how platforms like Found move from early traction to sustained enterprise scale.
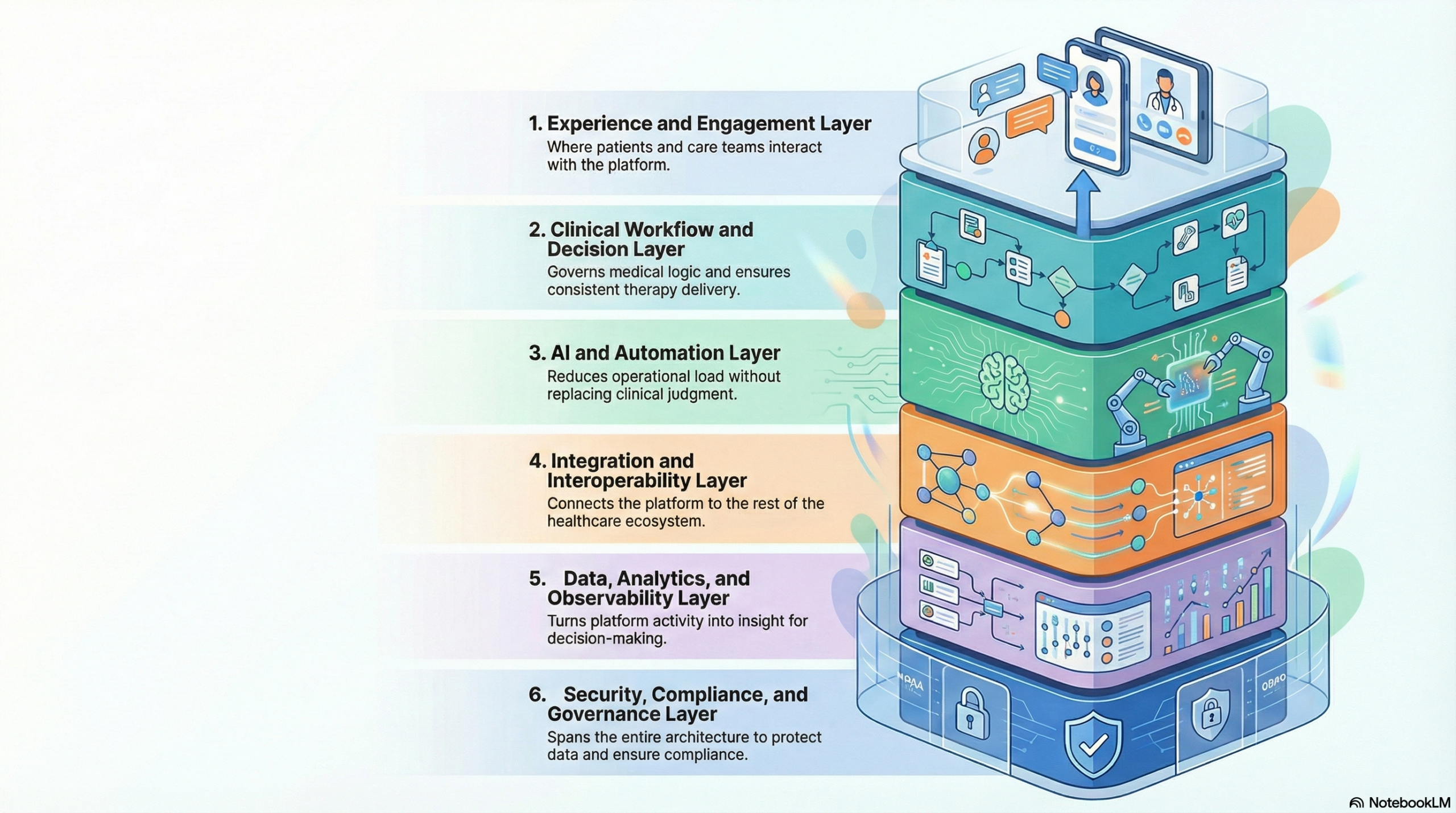
1. Experience and Engagement Layer
This is where patients and care teams interact with the platform. It includes onboarding, assessments, follow-ups, messaging, and progress tracking. The goal at this layer is clarity and consistency. Patients need to understand what happens next. Care teams need clean, structured inputs they can act on.
This layer is also where engagement is shaped. Poor design here leads to drop-offs that ripple through clinical and financial outcomes later.
Common technologies and tools
- Web and mobile frameworks such as React, Next.js, Flutter
- Secure messaging using Twilio or similar communication APIs
- Form and intake orchestration using custom workflows or tools like Form.io
- Authentication via OAuth 2.0, OpenID Connect, and SSO integrations
2. Clinical Workflow and Decision Layer
This layer governs medical logic. It handles eligibility checks, prescribing rules, dose titration schedules, follow-ups, and escalation pathways. It ensures that GLP-1 therapy is delivered consistently, regardless of provider or volume.
At scale, this layer prevents clinical drift. It embeds guardrails so unsafe actions simply cannot proceed without review.
Common technologies and tools
- Clinical workflow engines built on BPMN frameworks
- Rules engines for eligibility and contraindication logic
- FHIR-based clinical APIs for structured health data
- Provider dashboards built with role-based access controls
3. AI and Automation Layer
This layer reduces operational load without replacing clinical judgment. AI is used to prioritize work, flag risk, and surface insights, not to make autonomous medical decisions.
It is especially important once patient volumes grow. Without automation here, provider and operations teams become bottlenecks.
Common technologies and tools
- Machine learning models for risk scoring and adherence prediction
- NLP for symptom analysis and intake normalization
- Workflow automation using event-driven services
- AI governance tooling for explainability and audit trails
4. Integration and Interoperability Layer
This layer connects the GLP-1 platform to the rest of the healthcare ecosystem. It ensures data flows cleanly between systems instead of being copied or manually reconciled.
When this layer is weak, teams rely on spreadsheets and workarounds. When it is strong, the platform feels native to the enterprise environment.
Common technologies and tools
- FHIR and HL7 APIs for EHR integration
- Pharmacy and e-prescribing APIs such as Surescripts
- Payer and prior authorization APIs
- API gateways, message queues, and event brokers
5. Data, Analytics, and Observability Layer
This layer turns activity into insight. It tracks outcomes, utilization, adherence, and financial performance across the platform. Leadership relies on this layer for visibility and decision-making.
It is also critical for compliance. Every action must be traceable and auditable.
Common technologies and tools
- Cloud data warehouses such as Snowflake or BigQuery
- Streaming and batch pipelines for real-time analytics
- BI tools for dashboards and reporting
- Logging, monitoring, and alerting systems
6. Security, Compliance, and Governance Layer
This layer spans the entire architecture. It controls access, protects patient data, and ensures the platform remains audit-ready at all times.
Without this layer, GLP-1 platforms accumulate risk silently until it surfaces through incidents or regulatory scrutiny.
Common technologies and tools
- Encryption at rest and in transit
- Role-based access control and identity management
- Audit logging and immutable event trails
- Compliance frameworks aligned with HIPAA and regional regulations
Why this layered approach matters
Each layer isolates complexity. Clinical logic does not break when integrations change. Engagement updates do not disrupt compliance. AI improvements do not bypass governance.
For healthcare enterprises, this architecture enables controlled growth. It supports higher patient volumes, tighter regulation, and evolving business models without constant re-engineering.
That is the difference between a GLP-1 platform that works today and one that remains reliable as it becomes core infrastructure tomorrow.
Which GLP-1 Workflows Can Be Safely Automated With AI?
AI has a role to play in GLP-1 telehealth platforms, but only when it is applied with restraint. The goal is to remove friction, surface risk early, and help teams operate at scale without losing control.
In successful GLP-1 platforms, AI works quietly in the background. It handles volume, prioritization, and pattern detection, while clinicians remain responsible for medical decisions. When this boundary is respected, automation becomes a safety layer rather than a liability.
1. Intake Triage and Eligibility Pre-Screening
The first place AI adds value is before a clinician ever sees the case. GLP-1 programs generate large volumes of intake data, much of it repetitive and structured.
AI can safely review intake responses, flag missing information, and pre-score eligibility based on predefined clinical criteria. This does not mean approving or rejecting patients. It means preparing cleaner, more complete cases for clinical review.
In practice, this reduces back-and-forth, shortens review time, and ensures providers focus on decision-making rather than data cleanup.
2. Risk Flagging During Ongoing Treatment
Once patients start GLP-1 therapy, the challenge shifts to monitoring. Side effects, adherence issues, and contraindications rarely appear as single signals. They emerge as patterns over time.
AI is well-suited to detect those patterns. It can analyze symptom trends, engagement gaps, and weight changes to flag cases that require attention. What it does not do is intervene directly.
Instead, the system routes flagged cases to the appropriate clinical or care team queue, with context attached. This keeps responses timely without removing human oversight.
3. Operational Routing and Workload Prioritization
As GLP-1 platforms scale, operational bottlenecks become a risk. Manual queues fill up. Urgent cases compete with routine follow-ups. Response times suffer.
AI can safely automate task routing by urgency, complexity, and role. For example, it can distinguish between a routine refill request and a case showing early signs of intolerance. It can also balance workload across care teams to prevent burnout.
This type of automation improves efficiency without touching clinical decisions.
4. Adherence and Drop-Off Risk Detection
One of the biggest threats to GLP-1 outcomes and ROI is silent disengagement. Patients stop checking in, delay refills, or abandon therapy without formal closure.
AI can monitor engagement signals and identify early signs of drop-off. When those signals appear, the platform can trigger reminders, outreach tasks, or care team review.
This approach protects outcomes while respecting patient autonomy. No automated medical action is taken without review.
5. Prior Authorization and Documentation Support
AI can also support administrative workflows that slow GLP-1 programs down. Prior authorization, documentation completeness, and resubmission preparation are time-consuming but rule-driven.
Here, AI can pre-fill forms, highlight missing fields, and assemble documentation packets based on payer requirements. Final submission still remains a human action.
The result is faster turnaround without introducing compliance risk.
Where AI Must Remain Assistive
There are clear boundaries that successful platforms do not cross.
- AI should not approve prescriptions, adjust dosages, or make clinical determinations.
- It should not override provider judgment or bypass established workflows.
When AI operates within defined guardrails, it strengthens the system. When it attempts to replace clinical authority, it creates risk.
How We Build GLP-1 Telehealth Platforms Like Found Health
Building a GLP-1 telehealth platform is not just about launching quickly. It is about maintaining stability once volume, scrutiny, and real-world variability come into play. Every step below is important because we know what can go wrong if we skip it.
At Intellivon, we treat these platforms as living systems, not one-time products. The process is organized, but our thinking is practical.
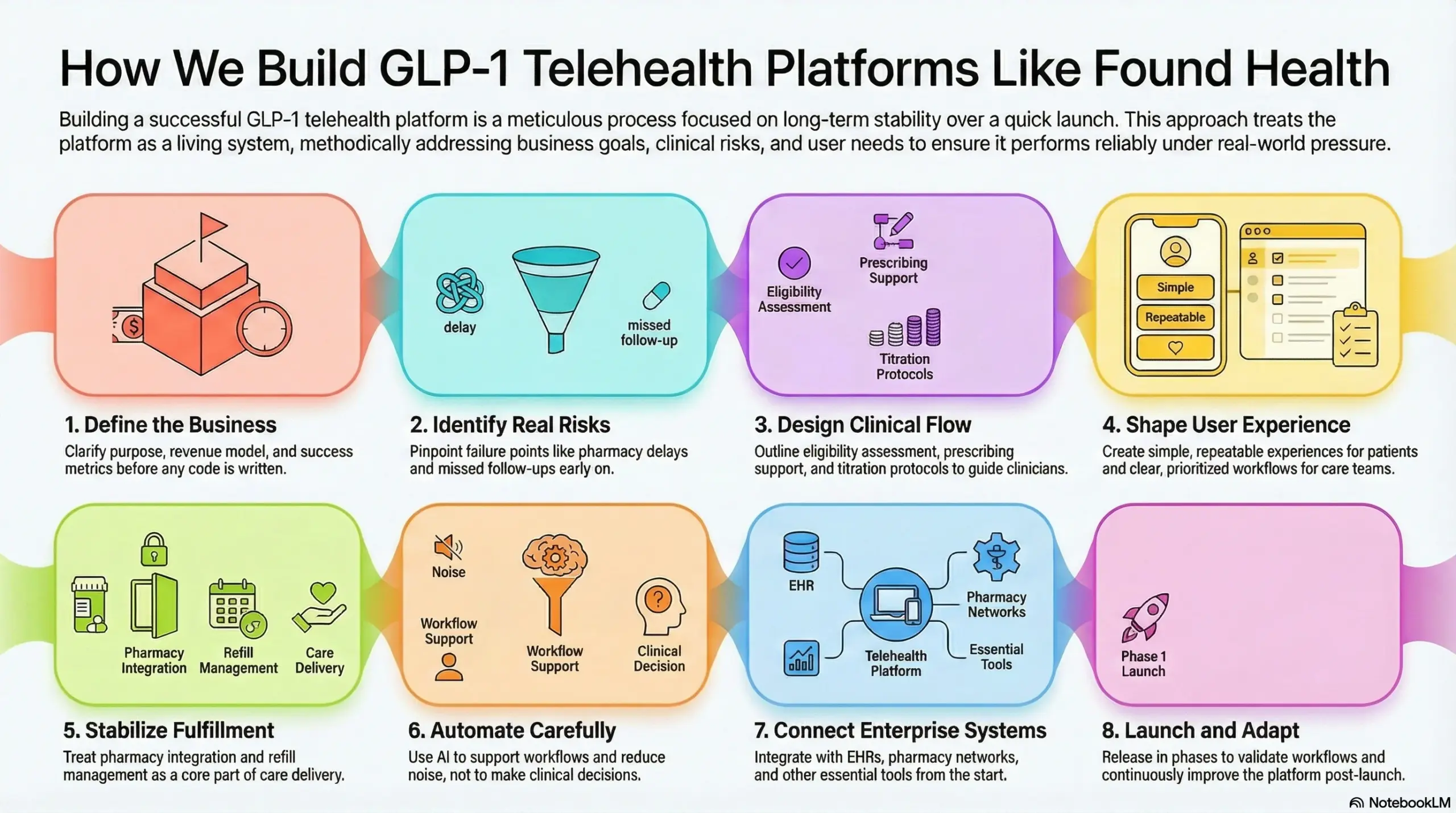
1. Define the business
Before we design or write code, we clarify the purpose of the platform. A GLP-1 program linked to payer savings operates very differently from one based on direct subscriptions.
We identify who the platform serves, how it generates revenue, and what success looks like six and twelve months after launch. This approach prevents us from building something that performs well in demos but fails in practice.
2. Identify real risks
GLP-1 platforms often fail weeks after launch due to missed follow-ups, inconsistent eligibility decisions, or pharmacy delays.
We pinpoint these failure points early on. We look at how GLP-1 programs perform at scale. Each risk becomes a platform control rather than just a policy document.
3. Design clinical flow
This step shapes the foundation of the platform. We outline how to assess eligibility, support prescribing decisions, and ensure titration and follow-ups are followed.
The platform guides clinicians without taking away their judgment. It standardizes care while allowing for flexibility where it’s medically necessary.
4. Shape user experience
We create experiences that prioritize repetition over novelty. Patients need to complete check-ins, request refills, and understand next steps easily.
Care teams require clear queues, context-rich views, and defined priorities. When user experience design is effective, everything downstream operates more smoothly.
5. Stabilize fulfillment
Access to medication affects outcomes. We view pharmacy integration and refill management as part of care delivery rather than an outside handoff.
The platform monitors prescription status, identifies delays, and raises issues before patients disengage. This reliability protects both outcomes and revenue.
6. Automate carefully
We only introduce AI after stabilizing the workflows. We use it to minimize unnecessary noise rather than to make decisions.
This includes cleaning up intake, prioritizing tasks, detecting adherence risks, and managing operations. Clinicians retain control while automation quietly supports them.
7. Connect enterprise systems
GLP-1 platforms cannot function in isolation for long. We integrate with EHRs, identity systems, pharmacy networks, and analytics tools early on.
We also ensure our integrations are resilient so that vendor changes or slowdowns do not disrupt care delivery.
8. Launch and adapt
We do not launch everything at once. Early groups help validate workflows. Automated checks track drift, delays, and anomalies.
When something goes wrong, the platform reacts. It prevents unsafe actions, notifies teams, and raises issues. Our developers remain active after launch to improve and enhance the system as usage increases.
This process produces GLP-1 platforms that hold up under pressure. Clinical quality remains consistent. Operations stay manageable. Leadership gets visibility into performance. Most importantly, GLP-1 becomes a sustainable growth platform rather than a short-term revenue spike.
If you are building a GLP-1 telehealth platform and want it designed for scale, governance, and long-term ROI, Intellivon can help you do it right from the start.
Cost to Build a GLP-1 Telehealth Platform Like Found Health
Building a GLP-1 telehealth platform like Found Health does not require a massive, all-at-once investment. Most healthcare enterprises begin with a focused, compliant foundation that supports core clinical workflows, prescribing governance, integrations, and monitoring, then scale in controlled phases.
At Intellivon, we structure GLP-1 platform costs around clinical maturity and operational readiness, not feature overload. This approach allows organizations to launch safely, validate ROI early, and expand without introducing avoidable regulatory or operational risk.
Estimated Cost Breakdown (USD 70,000–180,000)
| Cost Component | What It Covers | Estimated Range |
| Discovery & Platform Design | Care model alignment, GLP-1 workflow mapping, compliance planning, architecture | $10,000 – $18,000 |
| Clinical Workflow Engine | Eligibility checks, prescribing logic, titration flows, follow-ups, escalation rules | $15,000 – $30,000 |
| Telehealth & Care Experience | Patient onboarding, assessments, messaging, care team dashboards | $12,000 – $25,000 |
| Pharmacy & Fulfillment Integration | E-prescribing, refill workflows, status tracking, exception handling | $10,000 – $20,000 |
| Prior Authorization & Coverage Logic | PA workflows, documentation rules, and denial handling | $8,000 – $15,000 |
| AI-Assisted Automation (Safe Scope) | Intake triage, task routing, and adherence risk detection | $8,000 – $18,000 |
| Enterprise Integrations | EHRs, IAM, analytics, payer systems | $10,000 – $22,000 |
| Security & Compliance Controls | HIPAA safeguards, RBAC, audit trails, logging | $7,000 – $15,000 |
| Testing, Launch & Stabilization | QA, pilot cohorts, post-launch fixes, monitoring | $6,000 – $15,000 |
Typical Investment Ranges
- Lean MVP (Controlled Launch): $70,000 – $100,000 (Supports core GLP-1 prescribing, monitoring, and fulfillment with basic integrations)
- Enterprise Phase-1 Platform: $120,000 – $180,000 (Adds automation, deeper integrations, analytics, and post-deployment safeguards.)
What drives costs up or down
GLP-1 platform costs vary based on a few key decisions:
- How strictthe eligibility and prescribing controls need to be
- Whether prior authorization is manual or automated
- Depth of EHR and pharmacy integration
- Volume expectations in the first 6–12 months
- Level of AI-assisted operational automation
Enterprises that rush to “feature completeness” often overspend early. Those that phase intentionally tend to reach stability faster.
GLP-1 Platform Deployment Challenges and How We Solve Them
Most GLP-1 platforms don’t collapse on launch day. They start wobbling later, once demand spikes, patients behave unpredictably, and teams discover that “telehealth + prescription” is only a small part of the actual operating model. That’s when minor inconsistencies become safety exposure, quick fixes turn into permanent workflows, and missing data quietly becomes an audit problem.
This is the reality we build at Intellivon. We assume post-deployment stress from day one, then we design the platform to stay steady under volume, scrutiny, and change, so you’re not constantly reacting once the program becomes core to the business.
1. Clinical Safety Drift at Scale
After launch, variation creeps in almost naturally. One provider interprets eligibility slightly differently, another handles titration timing with a bit more flexibility, and soon the platform is delivering different care depending on who is on shift and how busy the day is.
Intellivon prevents this by converting your care protocol into a guided workflow. Eligibility capture is structured, critical checkpoints are enforced, and titration follow-ups are standardized, so clinicians still decide, but the safe path remains the easiest path. We also design progression logic to pause when prerequisites are missing, which keeps quality consistent as volume grows instead of letting risk accumulate quietly.
2. Side-Effect Escalation Gaps
Side effects rarely show up as a single dramatic moment. More often, they appear as a pattern. In many platforms, those signals sit buried in chat threads and form responses, waiting for someone to notice them at exactly the right time, which is not a reliable strategy once you scale.
We treat symptom monitoring like an operational workflow, not a passive data capture exercise. We structure check-ins, track symptom intensity over time, and route cases into triage queues based on urgency so the right team sees the right work at the right time.
Response timelines are enforced at the platform level, and if a high-risk case isn’t acknowledged within SLA, escalation triggers automatically, which keeps response predictable even during peak demand.
3. Fulfillment and Refill Failures
Fulfillment failures usually start small and become expensive. A prescription is sent but never acknowledged, a refill request sits in a queue too long, a supply issue delays delivery, and patients often don’t tell you until they’re already frustrated. The downstream impact hits quickly: adherence drops, outcomes become noisy, churn increases, and support tickets pile up, which drains operations and erodes margins.
Our experts track prescription states end-to-end, monitor refill timing continuously, and build exception handling so delays are surfaced early and handled deliberately. The platform should detect trouble before the patient feels it.
We also add observability so leadership can see refill latency, failure rates, and pharmacy performance in real time, preventing “silent failure” from becoming the default operating mode.
4. Prior Authorization and Coverage Volatility
Prior authorization is where GLP-1 platforms quietly lose time and money. It often begins manageable, then volume rises and payer behavior changes, denials spike, cycle times stretch, and ops teams end up chasing missing fields and resubmitting packets all day. Every manual step multiplies under scale, and what looked like a process detail becomes a bottleneck that slows growth.
Intellivon reduces that drag by designing PA as a structured workflow that runs on validated clinical data. The platform captures the right fields early, checks completeness automatically, and assembles payer-ready documentation rather than relying on manual compilation.
When denials occur, cases move into defined resubmission paths instead of ad hoc handling. We also track payer volatility across plans and reason codes so leadership sees trends early, before margins erode and teams burn out.
5. Provider Capacity Overload
GLP-1 operations don’t scale linearly. Every new cohort generates follow-ups, titration checks, refill requests, symptom reviews, and authorization work, and if humans have to route and prioritize everything manually, queues fill fast, and urgent cases get buried behind routine tasks.
Intellivon uses workflow orchestration to keep capacity under control. Tasks are routed by role, urgency, and complexity, where routine work flows to the right teams automatically, while clinical tasks surface with context rather than noise.
Automation decides what needs attention first, clinicians decide what action to take, and that boundary keeps the platform scalable without diluting clinical accountability.
6. Compliance and Audit Exposure
Compliance gaps rarely announce themselves early. They show up months later during audits, incident reviews, or payer disputes: missing consent artifacts, incomplete visit documentation, audit logs that can’t explain who did what and when. In GLP-1 care, those gaps translate into enterprise risk because prescribing, escalation, and coverage decisions must always be defensible.
We embed governance into the architecture so compliance is continuous rather than reactive. We enforce role-based access, maintain immutable event trails, and capture consent and documentation inside normal workflows, not as a separate reporting exercise.
The system stays audit-ready by default, which matters because teams rarely have time to reconstruct history after something goes wrong.
Automated Checks on Platform Post-Deployment
Automation only helps when it reflects real failure patterns. We design automated checks as operational controls with clear triggers, defined responses, and escalation paths, with one simple goal: when something starts drifting, the platform catches it early and pulls it back into control.
- Clinical safety triggers fire when eligibility data is incomplete, contraindications appear, or dose escalation is requested without a required follow-up.
- Side-effect monitoring triggers activate when symptom trends suggest intolerance, post-titration risk patterns emerge, or high-priority check-ins are missed.
- Fulfillment and pharmacy triggers detect stalled prescription states, overdue refills, or repeated delivery failures.
- Insurance and PA triggers surface when denial rates exceed thresholds, PA cycle times breach targets, or payer-specific rejection patterns appear.
- Identity, misuse, and fraud triggers activate when duplicate identity signals, unusual consult patterns, or misuse indicators cross thresholds.
Human Escalation When Automation Reaches Its Limits
Automation shouldn’t pretend to solve everything. Some issues need humans quickly, especially complex clinical cases, new payer rules, integration failures, and security anomalies.
Intellivon designs tiered escalation lanes from the start so clinical ops, compliance, and engineering have clear responsibilities, SLAs, and incident playbooks.
Post-incident reviews feed back into the platform as improved controls, better alerts, and tighter workflows, which is how the system gets stronger over time rather than just busier.
Conclusion
GLP-1 telehealth is no longer an emerging opportunity. It is becoming a core capability for healthcare enterprises that want to grow responsibly while managing cost, risk, and clinical quality. The difference between platforms that scale and those that stall is not demand. It is how well the platform is designed to operate under real-world pressure.
At Intellivon, we build GLP-1 platforms as enterprise infrastructure, with governance, automation, and visibility engineered in from the start. If you are looking to move beyond pilots and build a platform that delivers sustained ROI, our teams can help you design, launch, and scale it with confidence.
Build Your GLP-1 Telehealth Platform With Intellivon
At Intellivon, we build GLP-1 telehealth platforms as enterprise operating systems, not lightweight prescribing tools layered onto telehealth workflows. Our platforms function as governed clinical and operational infrastructure, unifying eligibility enforcement, prescribing guardrails, monitoring, fulfillment, automation, and compliance into one controlled system.
Each solution is engineered for healthcare enterprises moving beyond pilot GLP-1 programs. Platforms are infrastructure-first, safety-led, and built to support long-term metabolic care, subscription-based clinical models, and payer-aligned programs while delivering predictable operations, controlled risk, and measurable ROI as demand scales across regions and populations.
Why Partner With Intellivon?
- GLP-1 platform architecture aligned with clinical governance, prescribing control, and post-deployment risk prevention
- Deep interoperability expertise across EHRs, pharmacy networks, payer systems, IAM, and enterprise analytics stacks
- Compliance-by-design platforms supporting HIPAA, audit readiness, role-based access, and defensible clinical decision trails
- Safe AI automation for intake triage, workload routing, adherence risk detection, and operational efficiency
- Enterprise delivery model with phased rollout, KPI-driven optimization, and long-term platform scalability
Talk to Intellivon’s healthcare platform architects to explore how an enterprise-grade GLP-1 telehealth platform can move beyond point solutions, strengthen clinical and financial control, and support scalable, responsible GLP-1 care with confidence.
FAQs
Q1. What is a GLP-1 telehealth platform?
A1. A GLP-1 telehealth platform is an enterprise clinical system designed to deliver GLP-1 therapy safely at scale. It manages eligibility assessment, prescribing guardrails, dose titration, monitoring, pharmacy coordination, and compliance within a single governed workflow. Unlike consumer telehealth tools, these platforms are built to withstand regulatory scrutiny, high patient volumes, and long-term clinical engagement.
Q2. How long does it take to build a GLP-1 telehealth platform like Found Health?
A2. Most healthcare enterprises can launch a controlled GLP-1 platform in approximately 10 to 14 weeks. This initial phase typically includes core clinical workflows, prescribing controls, fulfillment integration, and compliance foundations. Additional automation, advanced analytics, and payer-specific workflows are added in phased releases, allowing teams to validate performance and ROI without overcommitting early.
Q3. How do GLP-1 platforms stay compliant with healthcare regulations?
A3. Compliance is enforced through platform architecture rather than manual oversight. Enterprise GLP-1 platforms implement role-based access, consent capture, immutable audit trails, and governed clinical workflows from the outset. Every action, from prescribing to escalation, is traceable and defensible. This approach keeps the system audit-ready continuously, reducing regulatory risk as scale increases.
Q4. Can AI be safely used in GLP-1 telehealth platforms?
A4. Yes, when applied within strict boundaries. AI is most effective when used for intake normalization, task prioritization, adherence risk detection, and operational routing. Clinical decisions such as prescribing and dose adjustments remain human-led. This balanced approach allows platforms to scale efficiently while maintaining patient safety and regulatory integrity.
Q5. What is the ROI of building a GLP-1 telehealth platform?
A5. ROI comes from multiple sources, including recurring clinical subscriptions, higher patient lifetime value, improved adherence, and lower operational cost per patient. Well-designed platforms also support payer-aligned and employer-funded care models by improving outcomes and reducing downstream utilization. Over time, GLP-1 platforms can evolve into durable growth engines rather than short-term revenue plays.