

Key Takeaways:
- AI RCM platforms connect patient access, coding, claims, denial prevention, payments, and analytics together.
- Production builds require EHR integrations, HL7/FHIR R4 data exchange, and EDI 837/835 workflows.
- NLP, predictive denial models, rules engines, and MLOps monitoring keep enterprise RCM platforms accurate.
- Development costs range from $70,000 to $270,000, depending on integrations, AI depth, and scale.
- Intellivon builds AI RCM platforms as a compliant revenue infrastructure designed for large health systems.
The market for AI revenue cycle tools has grown faster than most health systems can evaluate them. Three separate AI tools, for eligibility, coding, and denial management, do not make a platform. Instead, they make a more expensive version of the integration problem you were already managing.
The gap shows up in rework. The AHA’s 2025 Cost of Caring report found hospitals spent $43 billion chasing insurer payments in 2025, which is nearly $18 billion of that overturning denials that were eventually paid anyway. A unified enterprise AI revenue cycle management system can bridge this gap.
An enterprise AI revenue cycle management platform is a coordinated system, connecting eligibility verification, prior authorization, computer-assisted coding, claims scrubbing, denial prediction, and payment reconciliation. The system is built on a shared payer rules engine and EHR integration, feeding every module from a single source.
At Intellivon, we build enterprise AI systems for hospital networks and health systems where claims logic, clinical NLP, and compliance architecture need to function as one coordinated platform. This blog draws on that experience and covers what building that platform actually requires, so you leave with the technical clarity to make a confident build or vendor decision.
What Is AI Revenue Cycle Software for Hospitals?
AI revenue cycle software for hospitals is an intelligent system that completely automates how a medical network gets paid by insurance companies. It takes over the heavy lifting of billing by reading doctor notes, finding the right price codes, and fixing errors before submission.
Instead of staff manually chasing claims or fixing rejections, the software catches billing mistakes early and predicts insurance denials. This platform keeps large health networks financially stable by turning messy paperwork into fast, accurate payments.
AI Revenue Cycle Software vs Traditional RCM Software
Traditional legacy platforms focus entirely on workflow digitization, creating static electronic work queues, manual billing workflows, and retrospective reporting that require human eyes to spot errors.
Conversely, an enterprise RCM platform uses predictive modeling and real-time document intelligence to execute anomaly detection and proactive denial management before a claim ever leaves the hospital network.
| Technical Capability | Traditional RCM Software | AI Revenue Cycle Platform |
| Core Architecture | Hard-coded logic engines and static database tables | Machine learning models, predictive scoring, and autonomous agents |
| Claim Modification | Manual review via staff work queues after a rule triggers | Real-time claims scrubbing and automated payment posting execution |
| Clinical Comprehension | Regular expression parsing and basic regex keyword lookups | Deep NLP clinical documentation extraction for ICD-10/CPT codes |
| Operational Focus | Retrospective reporting and post-submission tracking | Forward-looking predictive denial prevention and risk management |
While predictive machine learning models can find hidden leakage patterns, your system must combine this intelligence with a deterministic payer-specific rules engine to securely handle hard validation limits like EDI 837 formatting and concrete contract terms.
Because of this architectural reality, hospital engineering teams must deploy hybrid architectures that use structured code to enforce rigid rules while reserving neural networks for complex tasks like reading clinical charts and predicting claim denials.
Where AI Should Not Make Final Decisions
LLMs excel at reading doctor notes. However, they must never have the final say on high-risk medical necessity validation or complex appeal submissions. Operating without human guardrails invites severe regulatory friction and revenue risk.
To maintain strict revenue integrity, large healthcare systems must isolate autonomous models from final execution across several touchpoints:
- Medical Necessity Validation: AI can flag documentation gaps. However, it must defer to a clinician to finalize an appeal argument.
- Prior Authorization Automation: Models can compile clinical evidence. Even so, an expert must review the package before submission to avoid penalties.
- Unsupervised Code Assignment: Natural language processing can suggest intricate code. A credentialed coder must verify the final output.
Organizations that fail to implement these human-in-the-loop guardrails risk running into serious compliance issues under HIPAA. They also face a high volume of unexpected billing errors.
[For a deeper breakdown of how to build reliable guardrails for production systems, see our guide on Healthcare AI App Development.]
Why Hospital Networks Are Consolidating RCM Point Tools Into Enterprise AI Platforms
Hospital networks are consolidating RCM point tools because fragmented systems make it harder to improve clean claim rate, first-pass resolution rate, days in AR, denial recovery, and net collection rate at scale. A unified AI RCM platform gives finance, access, coding, and billing teams shared data, shared rules, and shared accountability.
A coordinated platform reduces that friction by connecting eligibility, coding, claims, and denial workflows through a shared data layer.
Grand View Research valued the global AI RCM market at $20.63 billion in 2024. That figure is projected to reach $70.12 billion by 2030, a 24.16% CAGR across five years. The growth reflects health systems actively shifting budgets away from manual billing operations and into AI infrastructure.
Enterprise AI platforms are becoming the preferred model because they connect workflow, analytics, and decisioning in one layer, which is where the market now sees the highest ROI.
A. What Enterprises Gain From Adopting AI RCM Platforms
Moving to a unified platform unlocks complete visibility over the financial health of your health system.
Instead of reacting to rejections, hospitals use predictive denial prevention to catch errors beforehand. This automation securely boosts the first-pass resolution rate and drives down total days in AR.
B. Major Healthcare Players in the Market
The enterprise environment features several massive technology providers. Large systems often evaluate the following market options:
- Optum (Change Healthcare): Uses immense data scale to run its integrated platform.
- R1 RCM: Delivers comprehensive full-cycle managed services and autonomous coding.
- Waystar: Excels at enterprise-scale automated claim scrubbing across multi-payer environments.
- Innovaccer: Offers a unified data operating layer to bridge clinical and financial operations.
When these standard market tools fail to fit complex, custom hospital billing rules, technical leaders often build tailored software layers.
[For a deep look at designing proprietary intelligence, see our guide on AI Agent Development Services.]
Payer-Rule Drift: The Hidden Reason AI RCM Platforms Lose Accuracy
AI revenue cycle software for hospitals loses its accuracy over time because insurance rules change constantly. This problem is called payer-rule drift. When an insurance company changes its rules, the artificial intelligence model continues to operate on old data.
Consequently, the platform begins to experience errors, which causes immediate claims rejections.
1. Payer Policies Change
Insurance companies alter their coverage rules every single week. If your system relies on static training data, the AI will miss these updates entirely.
This gap causes your clean claim rate to drop fast. To fix this, your platform must connect directly to payer portals to pull live text updates.
2. Prior Authorization Criteria Shift
What required no permission last month might require official medical necessity validation today. When authorization rules shift, the AI software will submit claims without the correct approval codes.
This lack of updated data leads to automatic insurance rejections. At Intellivon, we address this issue by building automated web scrapers that flag changes instantly.
3. Contract Terms Update
Hospitals negotiate new reimbursement rates and payment terms with insurance payers every single year. If the billing engine uses outdated contract terms, underpayment detection tools fail to spot when an insurance company pays less than agreed.
The system must update its core contract database instantly to protect your revenue integrity.
4. Denial Patterns Evolve
Insurance companies use their own AI platforms to find new reasons to reject hospital claims. As their denial patterns evolve, your predictive models must adjust their risk scoring calculations to match.
Without this continuous loop, your front-end claims scrubbing tools become completely blind to new types of rejections.
5. Model Performance Drops Without Monitoring
An AI model will slowly decay if engineers do not actively watch its real-time outputs. This drop in performance means the system starts missing simple coding errors and processing invalid CPT codes.
Technical teams must use continuous MLOps model monitoring to catch accuracy drops before they impact your daily cash flow.
6. Rules Engines Need Versioning
Software teams cannot simply overwrite billing rules without keeping track of older copies. Because claims can take months to process, the system must know exactly which rule was active on the specific day of a medical procedure.
Using software versioning prevents your billing and coding platform from breaking during retroactive audits.
7. RCM Leaders Need Ownership of Rule Updates
Hospital billing directors cannot wait around for weeks for IT departments to update basic software code. Instead, non-technical managers must have clear ownership of rule updates through an easy-to-use, visual dashboard.
This approach gives operational teams control, allowing them to adjust rules across entire hospital networks instantly.
Payer-rule drift can cause a hospital platform’s accuracy to drop by 14% in less than six months if the system does not receive continuous updates.
For a deeper breakdown of how to build reliable data pipelines that fight rule decay, see our guide on Enterprise AI App Development.
Where AI Fits Across the Hospital Revenue Cycle
AI fits across the hospital revenue cycle wherever teams need faster validation, better prediction, cleaner documentation, stronger routing, or earlier exception detection.
The highest-value use cases usually sit in eligibility verification, patient financial clearance, coding support, claims scrubbing, denial prediction, underpayment detection, payment posting, and AR prioritization.
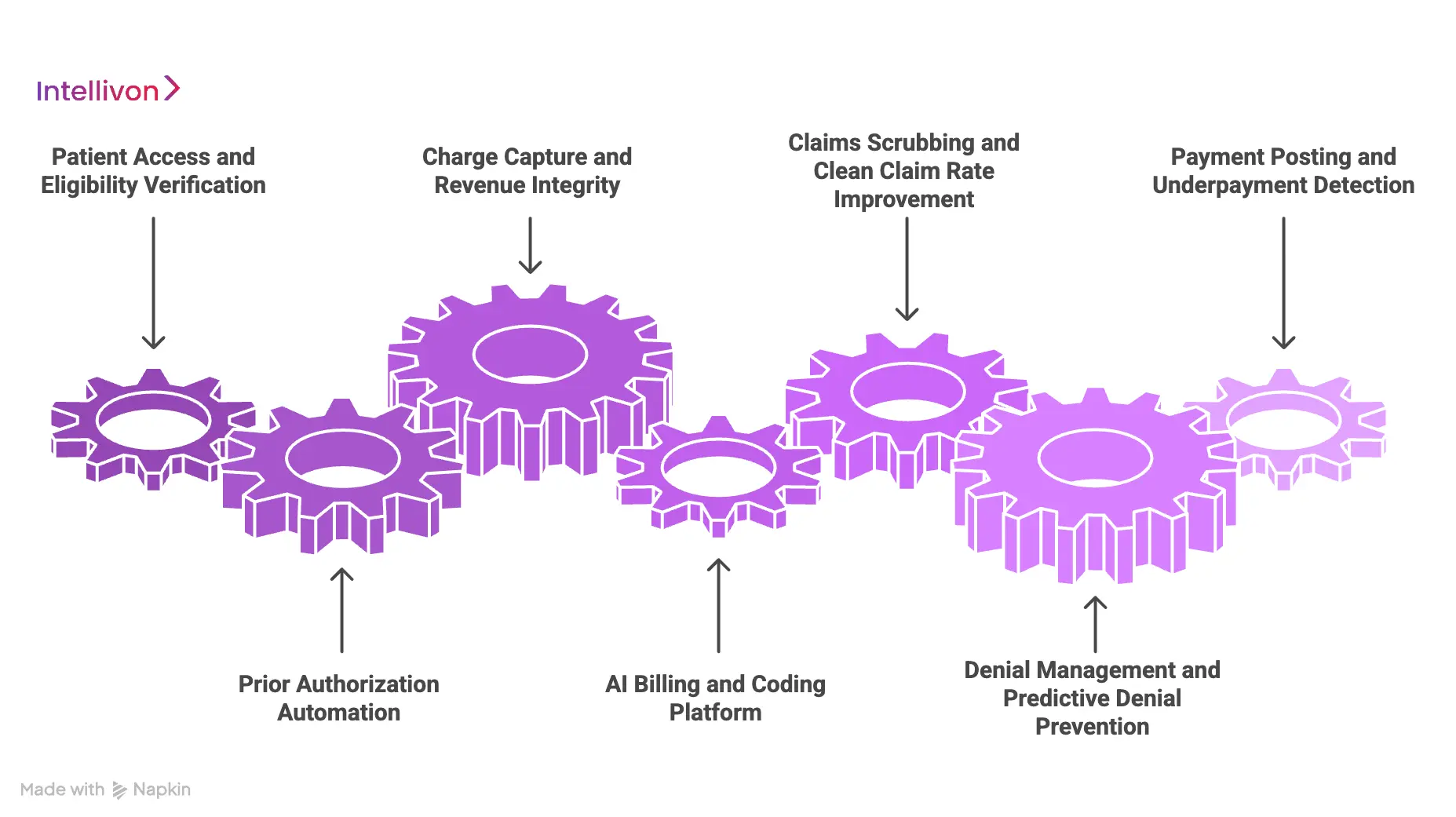
1. Patient Access and Eligibility Verification
Front-end mistakes account for a massive share of ultimate insurance rejections. To solve this, automated tools instantly scan patient demographics and check current coverage status against real-time benefits discovery engines.
This early confirmation improves patient financial clearance. It blocks invalid claims at registration, driving down expensive downstream processing errors across your entire network.
2. Prior Authorization Automation
Gathering clinical documentation to satisfy complex payer criteria traditionally drains administrative hours. CMS finalized the Interoperability and Prior Authorization rule, requiring faster decisions by January 1, 2026, and strict API integrations by January 1, 2027.
Advanced platforms meet this timeline by reading clinical records, running medical necessity validation, and tracking authorization status automatically.
3. Charge Capture and Revenue Integrity
Hospitals frequently lose track of expensive clinical services rendered during complex patient encounters. Intelligent software loops through EHR logs to spot missed charges, flag duplicate entries, and maintain strict chargemaster alignment.
By checking actual medical service documentation against final records, the system fixes billing gaps before the files are transferred to the coding team.
4. AI Billing and Coding Platform Enterprise Workflows
Managing the assignment of complex ICD-10-CM, CPT, and HCPCS codes requires high operational precision. Natural language processing models analyze physician documentation to suggest highly accurate codes while adjusting for HCC risk categories.
This automation keeps your coding accuracy rate high. It protects revenue integrity and successfully prevents common coding-related denials.
5. Claims Scrubbing and Clean Claim Rate Improvement
Standard claim validation often misses custom, payer-specific edits that trigger rejections. Enterprise platforms review electronic claims data before assembling the final EDI 837 transaction file for submission.
This thorough scrubbing checks every document against live insurance guidelines. It maximizes your first-pass resolution rate and ensures a high clean claim rate.
6. Denial Management and Predictive Denial Prevention
Waiting for a denial to arrive before taking corrective action creates massive backlogs. Predictive systems use real-time denial risk scoring to analyze claims data before submission, clustering potential errors by root cause.
By learning distinct payer-specific denial patterns, the platform routes high-risk cases to specialists for human review before any revenue leaks out.
7. Payment Posting and Underpayment Detection
Processing electronic remittance advice files often hides hidden payment variances. The platform consumes EDI 835 files to automate payment posting workflows while matching incoming cash against payer contract management systems.
If an insurance company pays less than the expected reimbursement, the software flags the variance and flags zero-balance accounts for audit.
After mapping these clear use cases, your technology leadership team must focus directly on the core system architecture that makes them work together.
HIPAA Compliance, PHI Security, and Human Review
AI revenue cycle management software must protect PHI through security controls that govern data access, model inference, workflow actions, audit logging, and vendor responsibilities. HIPAA compliance should be engineered into the platform through RBAC, encryption, access monitoring, audit trails, secure deployment, and human-in-the-loop review.
The Department of Health and Human Services mandates physical, technical, and strict administrative safeguards to protect all electronic patient data securely.
1. Implementing RBAC and ePHI Guardrails
Large hospital networks process millions of sensitive financial records containing electronic protected health information daily.
To secure these endpoints, developers must implement strict role-based access control (RBAC) layers that restrict record visibility based on specific administrative roles.
- The Minimum Necessary Rule: Administrative staff should only view the absolute minimum clinical text required to validate a claims file.
- Granular Field-Level Masking: Database pipelines should dynamically strip out patient social security numbers and personal addresses during the automated coding phase.
- MFA Network Access: Forcing multi-factor authentication across every system entry point blocks credential-stuffing attacks
Skipping strict identity controls exposes your organization to accidental insider disclosures and massive data leaks. If an unauthorized user accesses unmasked clinical charts, your health system faces severe regulatory audits.
Intellivon builds custom security layers into our database pipelines from day one. We isolate your training data from public networks to ensure your information remains confidential and fully protected.
2. Securing Model Inference and Continuous Audit Logging
Deploying predictive neural networks means that protected information continuously feeds into active machine learning pipelines. Engineering teams must encrypt all data streams using AES-256 for data at rest and TLS 1.3 for data in active transit across networks.
- On-Premise Private Deployments: Run your models entirely within your secure virtual private cloud to prevent data leakage to external APIs.
- Immutable Database Logs: Log every single model inference, human modification, and data export to an unalterable storage layer.
- Automated Security Scanning: Use continuous vulnerability scanning tools to monitor your system containers for package defects.
When engineering teams use basic, unencrypted third-party APIs for processing text, they lose complete control over data residency. This architectural mistake violates core business associate requirements and creates severe long-term liabilities.
Intellivon sets up self-contained model deployment pipelines that process high-volume files without sending records outside your firewall. We write rigorous code that keeps your financial operations secure, visible, and fully auditable.
RCM KPIs That Prove Enterprise Revenue Cycle Optimization
Enterprise revenue cycle optimization should be measured through operational, financial, and compliance KPIs.
The most important metrics include clean claim rate, first-pass resolution rate, days in AR, denial rate, appeal success rate, cost per claim, net collection rate, underpayment recovery, and coder review accuracy.
| KPI | What It Measures | Why It Matters | AI Platform Impact |
| Clean claim rate | Claims accepted without edits or rejection | Shows front-end and coding quality | Pre-bill validation and payer-rule checks |
| First-pass resolution rate | Claims paid without rework | Measures submission accuracy | Denial prediction and documentation alerts |
| Days in AR | Time to collect receivables | Shows cash velocity | AR prioritization and status automation |
| Denial rate | Claims denied by the payer | Shows preventable leakage | Predictive denial prevention |
| Net collection rate | Collectable revenue captured | Shows financial performance | Underpayment and variance detection |
| Cost per claim | Administrative cost per transaction | Shows automation ROI | Workflow automation and exception routing |
| Coding accuracy rate | Code quality and compliance | Reduces coding-related denials | NLP and coder review support |
| Underpayment recovery | Missed reimbursement found | Protects payer contract value | EDI 835 and contract variance detection |
Industry studies show that running manual claim status inquiries consumes massive amounts of provider time and increases transaction expenses. Specifically, transitioning from manual inquiries to automated tracking saves health system staff up to 18 minutes per transaction.
Because of these steep operational costs, hospital financial leaders must use hard data to build their automation ROI models. Tracking these baseline metrics allows management to identify financial leakages across multi-facility networks easily.
How to Build AI Revenue Cycle Software for Hospitals
To build AI revenue cycle software for hospitals, start with workflow discovery, then design the data architecture, build the rules engine, develop AI models, integrate EHR and payer systems, add compliance controls, pilot high-value workflows, and scale through MLOps monitoring.
Each step should reduce measurable revenue friction.
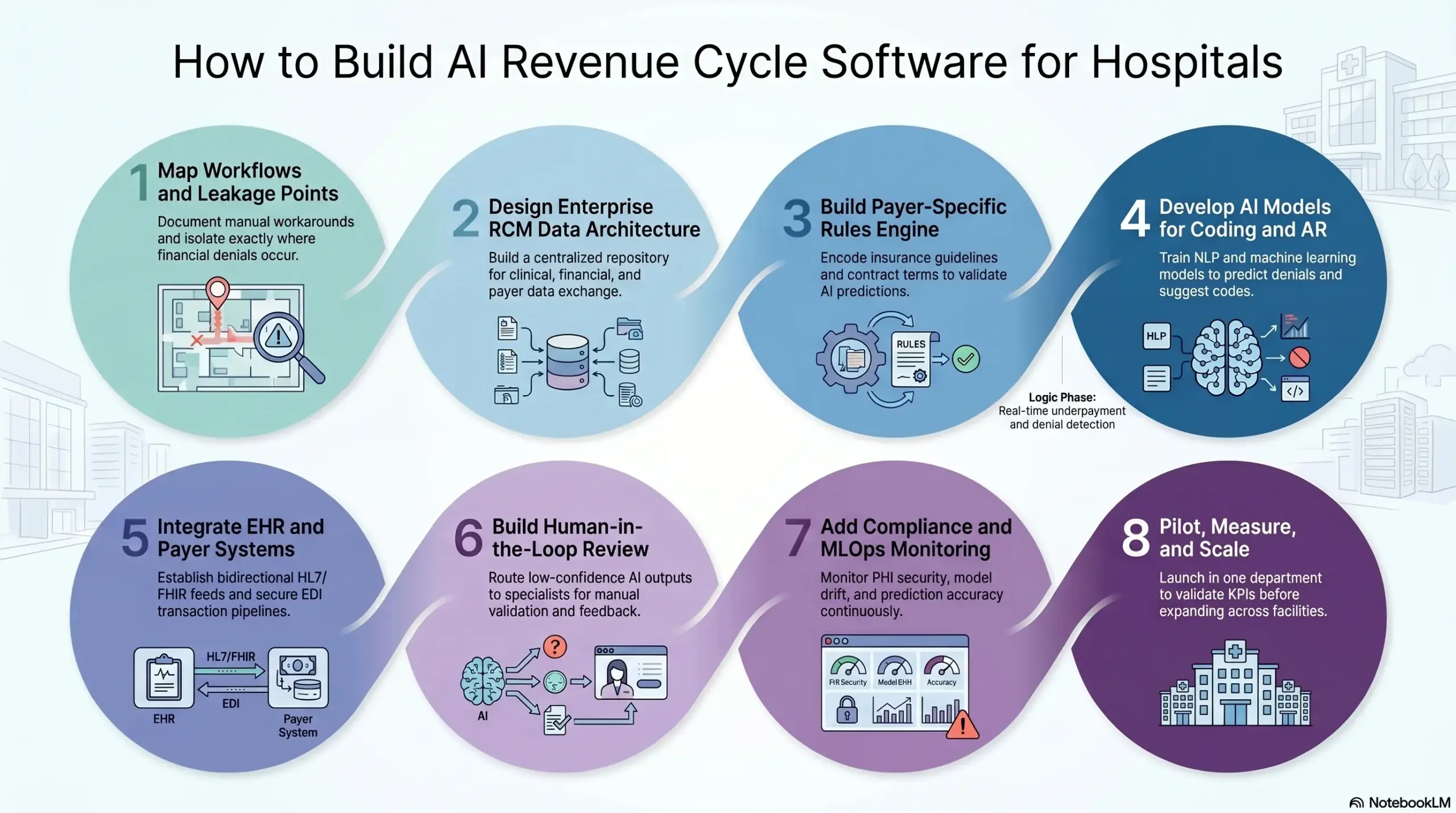
Step 1 — Map the Revenue Cycle Workflows and Financial Leakage Points
Start by mapping every revenue cycle workflow from patient access to zero-balance accounts. This gives your team a practical view of where delays, denials, underpayments, coding errors, authorization gaps, and manual rework occur. Without this map, the platform risks automating workflows that do not move financial KPIs.
- Workflow Interviews: Conduct detailed sessions with front-end staff, coders, and billing specialists to document actual manual workarounds.
- System Inventory: Map out every legacy point tool, database, and clearinghouse connection currently operating across your hospital network.
- Denial Root-Cause Review: Analyze historical remittance data to isolate exactly why specific payers reject high-value claims.
- Current KPI Baseline: Capture clean baseline metrics for your current clean claim rate, days in AR, and net collection rate.
| Assessment Layer | Technical Target | Primary Objective |
| Operational Mapping | Legacy workflow state discovery | Isolate manual processing bottlenecks |
| Financial Audit | Historical denial data extraction | Identify high-frequency leakage points |
| Technical Inventory | System dependency mapping | Document integration constraints and silos |
Intellivon starts by translating operational pain points into clear platform modules, precise integration priorities, and measurable revenue outcomes. We ensure every line of custom code targets an explicit financial friction point. Once the workflows are clear, the platform needs a reliable data foundation.
Step 2 — Design the Enterprise RCM Data Architecture
The data architecture defines how clinical, financial, payer, contract, and workflow data move through the platform. It should support real-time data exchange where needed and batch processing where appropriate.
Poor architecture creates duplicate records, incomplete claim context, weak AI predictions, and unreliable KPI reporting.
- Data Lake Construction: Build a centralized repository capable of securely storing structured billing codes and unstructured clinical text.
- Patient Identity Matching: Deploy deterministic and probabilistic matching algorithms to link disparate encounters to a single master index.
- EHR Ingestion Pipelines: Set up high-frequency data pipelines to stream real-time clinical notes directly from your primary health record systems.
- FHIR R4 Schema Mapping: Normalize incoming data structures into standardized, interoperable healthcare schemas to ensure smooth downstream processing.
| Data Pipeline Stage | Data Source Type | Processing Mode |
| Clinical Ingestion | EHR documentation & clinical notes | Real-time streaming (HL7/FHIR) |
| Financial Ingestion | Chargemaster & practice management data | Scheduled batch processing |
| Payer Ingestion | EDI 835 / EDI 837 transaction logs | Event-driven file processing |
We design the data layer before AI development so model outputs remain traceable, auditable, and usable by RCM teams. At the same time, we prioritize clean pipeline mechanics to give models a pristine foundation. After data design, payer logic must be formalized before AI decisions enter production.
Step 3 — Build the Payer-Specific Rules Engine
The payer-specific rules engine validates claims against known payer policies, contract terms, coding edits, authorization requirements, and medical necessity rules.
This layer protects the platform from treating AI predictions as the final truth. If skipped, the software may generate confident but non-compliant recommendations.
- Rules Library Encoding: Translate complex, paper-based insurance guidelines into a highly structured, programmatically queryable rules library.
- Contract Logic Validation: Code exact fee-for-service schedules and value-based reimbursement terms to verify incoming payment accuracy.
- Medical Necessity Cross-Checks: Map CPT codes directly against active LCD/NCD guidelines to catch medical necessity validation failures early.
- Rule Versioning Systems: Implement strict timestamping for every policy to ensure old claims use rules active during the patient encounter.
| Rule Category | Verification Method | System Execution Target |
| Formatting Validation | Deterministic syntax checking | Pre-submission EDI 837 syntax scrubbing |
| Contractual Compliance | Database fee schedule matching | Real-time underpayment detection |
| Clinical Alignment | Code-to-guideline intersection | Pre-billing medical necessity validation |
Intellivon separates deterministic payer logic from AI inference so hospitals can audit exactly why a claim was flagged. This keeps the platform stable, legally compliant, and completely predictable. With rules in place, AI models can support decisions without replacing control.
Step 4 — Develop AI Models for Coding and AR
AI model development should focus on bounded RCM tasks: documentation extraction, coding support, denial prediction, claim risk scoring, underpayment detection, and AR prioritization.
Each model needs training data, labels, validation logic, confidence scores, and review thresholds. Skipping this discipline creates unreliable automation and low user trust.
- Clinical NLP Customization: Train deep natural language processing models to read unstructured charts and extract valid CPT and ICD-10 codes.
- Denial Risk Classifiers: Build supervised machine learning models to analyze pre-submission claims and assign an explicit denial probability score.
- Variance Detection Models: Deploy anomaly detection models to flag subtle payment variances that violate historical payer behaviors.
- Explainability Layer Integration: Attach transparent evidence links to every model prediction so coding teams can see the exact source text.
| Model Archetype | Core Algorithm Class | Primary Output Metric |
| Coding Assistant | Named Entity Recognition (NLP) | CPT / ICD-10 code suggestions |
| Denial Predictor | Gradient-boosted decision trees | Pre-submission denial probability score |
| AR Prioritizer | Multi-variable ranking models | Work-queue liquidity optimization score |
Our experts build AI models with evidence links, confidence thresholds, and human review queues for high-risk financial decisions. We build models that reveal their reasoning so human operators can trust their choices. The models need hospital-system integrations before teams can use them in daily operations.
Step 5 — Integrate EHR and Contract Systems
Integration connects the AI RCM platform to the systems where revenue data already lives. The core integration stack usually includes EHRs, practice management systems, clearinghouses, payer APIs, EDI 837/835 files, contract systems, and analytics warehouses. Weak integration forces teams back into manual reconciliation.
- Bidirectional HL7 Feeds: Establish secure, two-way data streaming to keep financial states synchronized across all administrative systems.
- Secure FHIR R4 Integration: Use standardized web APIs to securely pull patient access data and clinical documentation on demand.
- EDI Transaction Handling: Build processing layers to parse outbound EDI 837 claims and ingest incoming EDI 835 remittance files.
- Clearinghouse API Connections: Connect directly to regional clearinghouses to track real-time claim status and receive instant error responses.
| Integration Endpoint | Protocol/Standard | Transmission Type |
| Electronic Health Record | FHIR R4 / HL7 v2 | Bidirectional real-time sync |
| Clearinghouse Gateways | RESTful JSON APIs | Event-driven request-response |
| Payer Remittance Engines | EDI 835 / EDI 837 | Scheduled batch secure SFTP |
Intellivon plans integrations early because RCM automation depends on reliable clinical, financial, and payer data movement. We eliminate data silos by engineering deep, bidirectional system connections. Once integrations work, the platform needs workflow controls for real users.
Step 6 — Build Human-in-the-Loop Review
Human-in-the-loop review keeps AI revenue cycle automation safe, explainable, and operationally useful. The system should route high-risk claims, low-confidence codes, authorization gaps, payment variances, and appeal drafts to the right specialists.
Without review queues, teams either distrust automation or approve risky outputs too quickly.
- Role-Based Work Queues: Route flagged files automatically to specialized coders or denial managers based on corporate access permissions.
- Confidence Score Thresholds: Set strict operational bounds where low-confidence AI choices demand mandatory human validation before submission.
- Immutable Audit Tracking: Capture every human modification, override, and comment to maintain a flawless record for future compliance checks.
- Active Feedback Loops: Route human corrections directly back to the MLOps pipeline to continuously improve model performance over time.
| Work Queue Type | Trigger Condition | Assigned Staff Persona |
| Coding Discrepancy | AI confidence drops below 85% | Certified Medical Coder |
| High-Risk Denial Preview | Predicted rejection risk above 70% | Denial Management Specialist |
| Contractual Variance | Underpayment flag detected | Payer Contract Auditor |
Intellivon designs review workflows around actual revenue-cycle roles, including coders, billers, denial teams, auditors, and finance leaders. We ensure the software mirrors real hospital operations perfectly. The same discipline should extend into compliance and model governance.
Step 7 — Add Compliance Controls and MLOps Monitoring
Compliance and MLOps controls make the platform safe to operate after launch. The system should monitor PHI access, model drift, prediction accuracy, rule changes, user actions, and exception outcomes. If this layer is weak, the platform may perform well during launch but degrade as payer behavior changes.
- Role-Based Access Control: Restrict visibility into protected health information to verified, authorized users based on corporate profiles.
- End-to-End Encryption: Protect all financial and clinical data using strict encryption layers both at rest and during active transit.
- Automated Drift Detection: Set up continuous monitoring alerts to catch instances where model prediction accuracy begins to degrade.
- Immutable Security Logs: Maintain comprehensive, unalterable system logs detailing exactly who accessed or altered financial data.
| Governance Layer | Monitoring Focus | Operational Safety Guard |
| Data Compliance | PHI access & audit trail tracking | Strict HIPAA regulatory alignment |
| Model Security | Data drift & prediction accuracy decay | Automated MLOps alerting triggers |
| System Auditability | Rule version updates & user overrides | Total transparency for external reviews |
Our experts treat post-launch monitoring as part of the initial build, not an afterthought. We build the infrastructure needed to keep your systems accurate, secure, and compliant for years. With controls in place, the rollout can start with measurable pilot workflows.
Step 8 — Pilot, Measure, and Scale Across Facilities
Start the rollout with a focused pilot tied to measurable RCM KPIs. Good pilot candidates include eligibility verification, denial prediction, coding review, underpayment detection, or AR prioritization. Scaling too broadly before validation creates adoption friction, integration overload, and unclear ROI.
- Pilot Site Selection: Deploy the initial software modules in a single, representative department to test system workflows safely.
- KPI Progress Capture: Monitor key operational targets like your first-pass resolution rate daily against historical data points.
- Staff Onboarding Audits: Review how effectively your billing teams adopt the new software queues during their daily routines.
- Phased Rollout Roadmaps: Expand the verified platform modules systematically across your remaining hospital facilities over time.
| Deployment Phase | Scope of Launch | Success Evaluation Criteria |
| Departmental Pilot | Single facility / bounded workflow | Technical stability & model validation |
| Regional Expansion | Multi-facility network deployment | Operational adoption & scale handling |
| Full Platform Scale | Total enterprise integration | Maximum net collection rate impact |
Intellivon structures rollout plans around measurable outcomes, then expands the module facility by facility. This methodical approach minimizes deployment risk and ensures clear operational validation at every stage. The build roadmap naturally leads into the cost model.
How Much Does AI Revenue Cycle Software for Hospitals Cost?
AI revenue cycle software for hospitals usually costs $70,000 to $270,000 to build, depending on platform scope, hospital size, AI model complexity, EHR integrations, payer connectivity, compliance depth, and rollout scale.
A focused MVP sits near the lower end, while a broader enterprise RCM platform with EDI workflows, payer rules, AI models, and HIPAA controls moves toward the higher end.
Cost Breakdown by Development Phase
| Development Phase | Estimated Cost Range | What It Covers |
| Discovery, RCM workflow mapping, and KPI baseline | $4,000–$10,000 | Workflow review, denial analysis, payer mix, system inventory, KPI targets |
| Product strategy and UX design | $4,000–$14,000 | Role-based dashboards, work queues, exception flows, and CFO views |
| Data architecture and normalization | $6,000–$22,000 | Data ingestion, patient matching, encounter mapping, data quality, and warehouse setup |
| Core backend and workflow engine | $8,000–$32,000 | Case routing, task queues, rule execution, claim workflow logic, and admin controls |
| EHR, HL7, FHIR R4, and clearinghouse integrations | $10,000–$40,000 | EHR feeds, FHIR APIs, HL7 messages, and clearinghouse connectivity |
| EDI 837/835 and payer transaction workflows | $6,000–$25,000 | Claims submission, remittance processing, claim status, and eligibility workflows |
| Payer-specific rules engine and contract logic | $5,000–$20,000 | Payer edits, contract terms, medical necessity, authorization requirements |
| AI model development | $8,000–$38,000 | NLP, denial prediction, coding support, AR prioritization, payment variance detection |
| Human-in-the-loop workflow development | $3,000–$12,000 | Review queues, approvals, escalations, audit notes, and feedback loops |
| HIPAA security and compliance controls | $4,000–$16,000 | RBAC, audit trails, encryption, PHI controls, logging, documentation |
| Analytics, KPI dashboards, and ROI reporting | $3,000–$10,000 | Clean claim rate, days in AR, denial rate, net collection rate, cost per claim |
| QA, pilot rollout, deployment, and training | $3,000–$11,000 | Testing, data validation, user training, pilot launch, monitoring |
| Scope buffer and implementation adjustments | $6,000–$20,000 | Integration changes, payer-rule updates, workflow refinements, launch support |
Total estimated development cost: $70,000–$270,000
HIPAA security controls should not be treated as a small add-on because the platform handles PHI across claims, payments, coding, and patient access workflows. HHS states that the HIPAA Security Rule requires administrative, physical, and technical safeguards for electronic protected health information.
Ongoing Maintenance Cost
Plan for 18%–30% of the initial build cost annually for cloud infrastructure, integration updates, payer-rule changes, model monitoring, security patches, support, and enhancement work.
For example, a $120,000 AI RCM platform may need $21,600–$36,000 per year in maintenance. A $270,000 platform may need $48,600–$81,000 per year, especially if it includes EHR integrations, EDI 837/835 workflows, payer contract logic, and predictive denial models.
Planning an AI revenue cycle software budget for a hospital network or health system? Intellivon can help you estimate cost based on platform scope, EHR integrations, EDI workflows, payer rules, AI models, compliance controls, and rollout timeline.
Build vs Buy: An Enterprise RCM Platform
Build custom AI RCM software when your hospital network has complex payer contracts, multi-facility workflows, unique integrations, or fragmented point tools that commercial platforms cannot unify.
Buy when your workflows match standard vendor patterns, your budget is limited, and your team needs faster deployment over control.
| Strategic Factor | Buying Off-the-Shelf RCM | Building Custom AI Platforms |
| Workflow Fit | Rigid; requires adapting hospital operations to software | High; built directly around proprietary billing rules |
| Data Residency | Shared information lives within the external vendor cloud | Absolute, full control over PHI data residency |
| Model Ownership | None; black-box algorithms remain vendor property | Complete; the hospital network owns and trains models |
| Time to Value | 3 to 9 months average deployment schedule | 12 to 24 months for complete production scale |
Build is Better When
- Multi-Facility Workflows: You operate multiple facilities with completely different operational workflows and infrastructure.
- Custom Payer Rules: You need custom payer-specific rules engines to handle niche reimbursement contracts.
- Deep Ingestion Integration: You require deep, bidirectional EHR and data warehouse integration layers.
- Algorithm Ownership: You want total ownership over your AI models and raw training data.
- Executive Dashboards: You need custom, live performance dashboards for CFOs and RCM leaders.
- Point-Tool Consolidation: You want to consolidate fragmented tools into one unified system.
Buy is Better When
- Narrow Function Needs: Your hospital network needs a narrow financial function deployed quickly.
- Limited Technical Bandwidth: You lack internal engineering or implementation bandwidth to support updates.
- Standard Workflow Alignment: You can easily adapt internal workflows to match standard vendor constraints.
- No Custom Modeling: You do not need proprietary or highly tailored AI models.
- Subscription-Based Pricing: You prefer predictable subscription pricing over upfront capital development costs.
Hybrid Model Options
Rather than choosing a single path, many health systems opt for a hybrid engineering strategy. Your technical team can use standard vendor tools for commodity tasks like regular electronic clearinghouse routing.
Then, build custom intelligence layers for advanced denial prediction, underpayment detection, and cross-system orchestration.
Conclusion
AI revenue cycle software for hospitals should be framed as enterprise infrastructure, not a feature upgrade. The strongest platforms connect patient access, coding, claims, denials, payments, payer contracts, compliance, and analytics into one governed operating layer.
For large health systems, the real decision is not whether AI can automate revenue cycle work. The better question is where AI should assist, where rules must control decisions, where humans must review exceptions, and where ROI should be measured first.
Intellivon’s role in this space is practical: build the architecture, integrations, AI workflows, compliance controls, and monitoring systems needed to make AI RCM work in production.
Build an AI Revenue Cycle Management Software Platform With Intellivon
At Intellivon, we help hospitals, health systems, RCM companies, healthcare SaaS teams, and enterprise healthcare businesses build AI revenue cycle software around real operational needs.
With 500K+ engineering hours, ex-MAANG engineers, and deep experience across AI, healthcare platforms, SaaS systems, API integrations, and enterprise software development, we help teams move from fragmented revenue workflows to scalable AI-powered RCM infrastructure.
A. Help You Define The Right Revenue Cycle Software Scope
Before development starts, we map your revenue cycle workflows, user roles, payer touchpoints, claim flow, denial patterns, coding needs, payment workflows, and integration requirements.
This helps us define what your platform should solve first.
We help you plan:
- Patient access workflows
- Eligibility verification needs
- Prior authorization automation scope
- Claims scrubbing requirements
- Denial prediction use cases
This keeps the first version focused, practical, and tied to measurable RCM outcomes.
B. Build AI Workflows Around Real Revenue Cycle Operations
AI should support revenue teams, not create another system they have to manage manually.
Intellivon builds AI workflows that help teams identify claim risks earlier, validate documentation, flag coding issues, detect denial patterns, route exceptions, and prioritize high-value revenue work.
Your platform can include:
- AI eligibility verification
- Prior authorization support
- NLP-based clinical documentation review
- AI-assisted coding workflows
- Claim validation rules
- Predictive denial scoring
- Smart work queues
- Exception routing
- Payment posting automation
- Underpayment detection
- Appeals support workflows
- Revenue cycle analytics
Every workflow is designed around how hospital billing, coding, finance, and RCM teams actually work.
C. Integrate With Healthcare, Payer, And Revenue Systems
AI revenue cycle software depends on accurate data movement across clinical, financial, and payer systems.
That is why Intellivon plans integrations early. We help connect your platform with the systems needed to verify coverage, process claims, validate coding, track denials, post payments, and measure revenue performance.
We support integrations across:
- EHR and EMR systems
- Practice management systems
- Clearinghouses
- Payer APIs
- EDI 837 and 835 workflows
- HL7 and FHIR interfaces
- Eligibility and claim status systems
- Coding and billing systems
- Payment systems
- ERP and finance platforms
- Data warehouses and BI tools
These integrations help your platform move revenue workflows from patient access to claims submission, denial prevention, payment tracking, underpayment recovery, and executive reporting.
D. Design AI RCM Platforms With Security From Day One
AI revenue cycle software handles PHI, payer data, financial records, claims history, coding data, payment files, and sensitive operational workflows. Security cannot be treated as a final-stage checklist.
Intellivon designs AI RCM platforms with healthcare-grade controls from the start.
This can include:
- PHI protection
- Data encryption
- Role-based access control
- Secure authentication
- Audit trails
- User activity tracking
- Admin permissions
- Human-in-the-loop review
- Secure cloud deployment
- Compliance-ready documentation
- Model monitoring controls
This helps your platform support hospital teams, enterprise buyers, payer-facing workflows, and regulated revenue cycle operations with confidence.
Ready To Build AI Revenue Cycle Software?
If you are planning to build AI revenue cycle software for hospitals, Intellivon can help you define the right roadmap before development begins.
We will help you identify the best AI use cases, map revenue cycle workflows, plan EHR and EDI integrations, design secure architecture, build AI models, and create a scalable platform around real RCM outcomes.
Ready to turn fragmented revenue workflows into a secure, AI-powered RCM platform? Contact Intellivon today to discuss your project.
Things To Know About Enterprise AI RCM Platforms
Q1. How much does AI revenue cycle software for hospitals cost?
A1. AI revenue cycle software for hospitals usually costs $180,000 to $1.2M+ to build. A focused MVP may cost $180,000 to $300,000, while a multi-facility enterprise platform with EHR, EDI, payer, AI, and compliance layers can exceed $750,000. At the same time, maintenance usually adds 18%–30% annually.
Q2. How long does an enterprise RCM platform take to build?
A2. A focused AI RCM MVP usually takes 4–6 months. A production platform for one hospital often takes 7–12 months. A multi-facility AI RCM platform for hospital networks can take 12–18 months because integrations, compliance, data validation, and adoption planning take real time.
Q3. Can AI revenue cycle management software be HIPAA compliant?
A3. Yes, AI revenue cycle management software can be HIPAA compliant when PHI controls are engineered from the start. The platform needs RBAC, encryption, audit logs, secure model inference, access monitoring, vendor agreements, and human review. Compliance cannot be added as a final QA checklist.
Q4. What AI models are required for an AI billing and coding platform enterprise workflows?
A4. Enterprise AI billing and coding platforms usually need NLP, document intelligence, classification models, coding recommendation models, denial prediction, payment variance detection, LLM-assisted summaries, and deterministic payer rules. AI should support coders and billers with evidence, not replace expert review for complex cases.
Q5. What integrations matter most for an AI RCM platform for hospital networks?
A5. The most important integrations are EHR, HL7, FHIR R4, EDI 837, EDI 835, clearinghouse, payer API, contract management, identity management, and analytics warehouse integrations. Without these, the platform cannot connect clinical documentation, claims, payments, payer rules, and revenue KPIs.



