

Healthcare systems face ongoing pressure to do more with fewer resources. Staffing shortages, rising patient needs, and uneven access to specialists continue to stretch operational models that were not built for today’s demands. Virtual care has emerged as a response, but many organizations quickly find that disconnected telehealth tools do not provide lasting results.
Caregility shows a clear direction for the market. Its infrastructure-first approach supports inpatient care, centralized command centers, and hybrid clinical teams without requiring organizations to change how they deliver care. This model treats virtual care as a permanent part of the healthcare system.
Creating a Caregility-like virtual care infrastructure requires careful planning across architecture, interoperability, and governance. At Intellivon, we have spent over a decade developing healthcare platforms that work within real hospital environments. In this blog, we explain how a virtual care infrastructure like Caregility’s should be designed, implemented, and expanded for modern healthcare systems.

Key Takeaways Of The Virtual Care Market
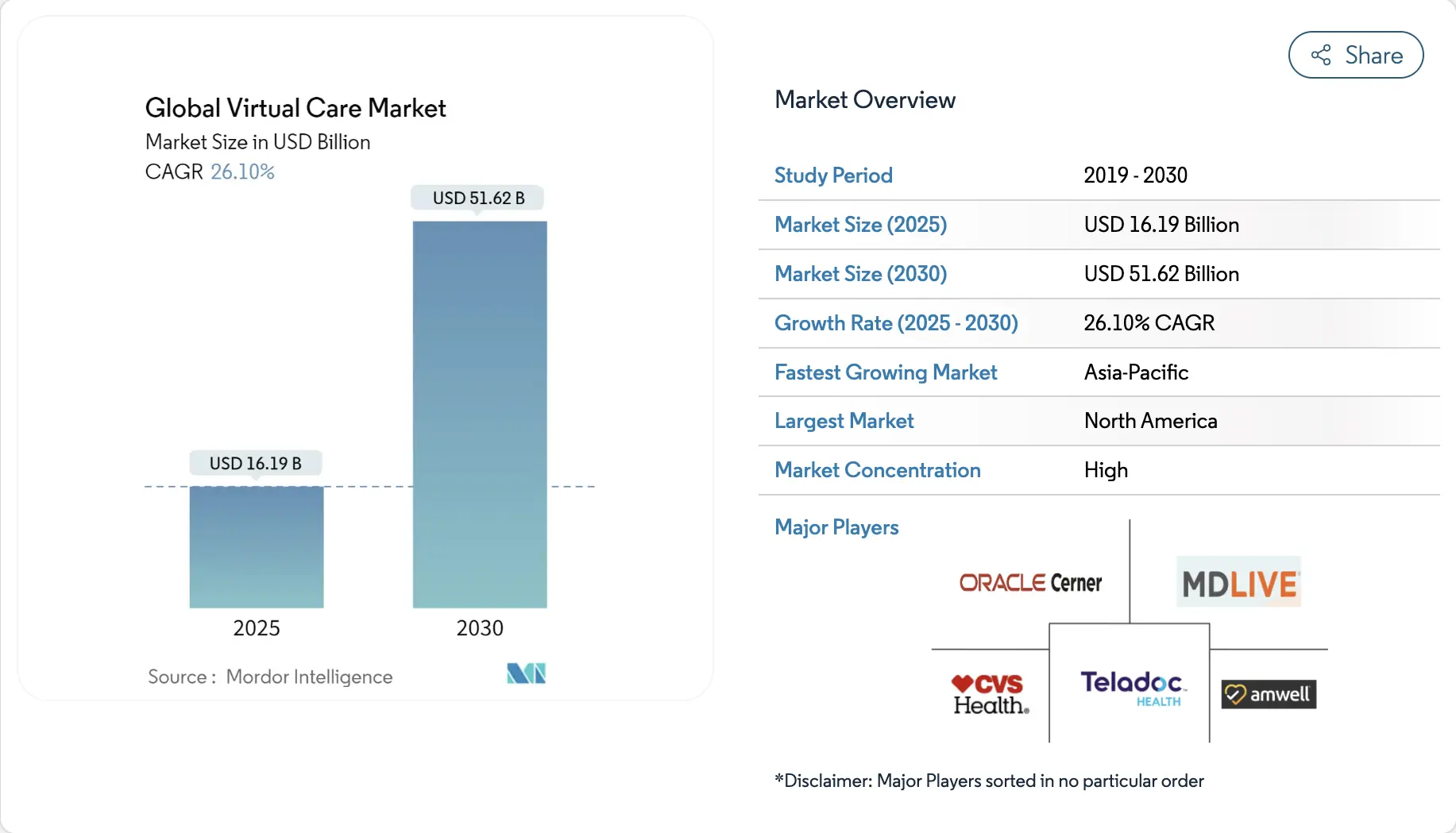
The virtual care market is already a multi-billion-dollar segment, valued at approximately USD 16.19 billion in 2025. Current projections indicate it will grow to nearly USD 51.62 billion by 2030, driven by a compound annual growth rate of about 26.1%.
Key Market Growth Drivers:
- The wider telemedicine sector is expected to reach roughly USD 112 billion in 2025 and continue expanding toward an estimated USD 335 billion by 2032, supported by an annual growth of 16.9 percent.
- Next-generation telehealth platforms that combine interoperability, hybrid care delivery, and enterprise integration are already valued at around USD 161.6 billion in 2024. Forecasts suggest this segment could approach USD 792.5 billion by 2034, signaling a clear move away from isolated tools toward infrastructure-level platforms.
- The global home healthcare market is also accelerating, projected to grow from approximately USD 309.9 billion in 2025 to nearly USD 473.8 billion by 2030. Remote monitoring and virtual care models play a central role in enabling this shift.
- Broader remote healthcare markets that combine telehealth, RPM, and virtual hospital capabilities are emerging rapidly. While current valuations sit in the lower tens of billions, long-term growth trajectories point to strong double-digit expansion through 2035.
Demand Drivers Shaping Virtual Care Adoption
- Rising chronic disease incidence, aging populations, and workforce shortages are pushing healthcare organizations to move routine and long-term care beyond traditional hospital settings.
- Industry research consistently highlights hybrid care models, blending in-person encounters with virtual touchpoints, as the dominant care delivery approach moving forward. This trend requires integrated platforms rather than standalone video visit software.
- Virtual nursing solutions alone are projected to grow into a market of approximately USD 14 billion by 2034. Hospitals account for more than half of projected revenue, reflecting accelerating adoption within inpatient environments.
- Virtual hospital infrastructure, including command centers and hospital-at-home models, is expected to expand from roughly USD 16.5 billion in 2024 to over USD 100 billion by 2034, growing at close to 20 percent annually.
What Is the Virtual Care Infrastructure Caregility?
Caregility is an enterprise virtual care infrastructure that embeds secure, device-agnostic video and remote clinical workflows directly into hospital operations, enabling inpatient, acute, and hybrid care delivery at scale.
At the platform level, Caregility provides a secure video and communication backbone that connects patient rooms, mobile carts, bedside devices, and centralized clinical teams. This enables use cases such as virtual rounding, continuous patient observation, specialist consults, and virtual nursing coverage within live care environments.
What distinguishes Caregility is its operational fit. The infrastructure aligns with clinical roles, access controls, and compliance requirements rather than forcing care teams into separate applications. Virtual care becomes an extension of hospital operations, not an external overlay.
How It Works
Caregility works by connecting patient-room endpoints to a secure virtual care network, routing sessions through role-based workflows, and logging activity for governance and clinical accountability.
1. Endpoints Get Deployed
Hospitals install in-room devices, mobile carts, or bedside-enabled displays. These endpoints become the “front door” for virtual interactions.
2. Connects Endpoints to Clinical Network
Caregility runs as a governed communication layer. It ensures encrypted video, authenticated access, and reliable connectivity across units and facilities.
3. Users Authenticate Through Roles
Clinicians, nurses, sitters, and specialists sign in through approved access methods. Role-based permissions control who can view, call, or monitor.
4. Workflows Trigger Virtual Care Sessions
Sessions start from operational needs, not ad-hoc calls. Examples include rounding schedules, observation protocols, consult requests, or escalation events.
5. Command Center Coordinates
Virtual nursing or centralized teams manage routing and workload. They assign calls, monitor queues, and ensure the right clinician joins at the right time.
6. Supports Live Collaboration
Remote clinicians can join a room session, bring in a specialist, or coordinate with bedside staff. This reduces handoff friction during time-sensitive care.
7. Documentation Stay Workflow-Aligned
Session metadata, timestamps, and notes can be aligned to documentation practices. This supports continuity without forcing duplicate work.
8. Governance and Audit Controls
The system records access logs, role actions, and operational metrics. This supports compliance, incident review, and performance improvement.
9. Performance Gets Optimized
Teams monitor uptime, utilization, response times, and workflow outcomes. The platform then expands unit-by-unit, facility-by-facility, with measurable control.
Caregility demonstrates how virtual care delivers the most value when it is engineered as infrastructure, not a point solution. For healthcare enterprises, this model turns virtual care into a scalable operational capability rather than a temporary workaround.
What Makes Caregility Infrastructure-First As A Platform
Caregility follows an infrastructure-first model by embedding virtual care directly into hospital operations, clinical workflows, and governance systems rather than delivering isolated telehealth functionality.
1. Built to Operate Inside Hospitals
Caregility is designed for inpatient and acute care settings where reliability is non-negotiable. The platform integrates with patient rooms, nursing units, and centralized command centers. This ensures virtual interactions occur within the same operational context as bedside care.
2. Workflow-Native, Not Visit-Centric
The platform aligns with how care teams actually work. Virtual sessions are triggered by rounding schedules, observation needs, or consult workflows rather than ad-hoc calls. As a result, clinicians adopt the system without changing their daily routines.
3. Device-Agnostic and Endpoint Flexible
Caregility supports a wide range of devices, from fixed in-room systems to mobile carts and remote clinician endpoints. This flexibility allows hospitals to scale virtual care across units without locking into a single hardware model.
4. Enterprise Governance Built In
Role-based access, session visibility, and audit logging are embedded into the platform. These controls support compliance, accountability, and clinical oversight without adding administrative burden.
5. Designed for Scale, Not Pilots
The infrastructure supports multi-unit, multi-facility deployments from day one. Performance monitoring, redundancy, and centralized management enable hospitals to expand virtual care confidently across their networks.
Caregility’s infrastructure-first design turns virtual care into a durable operational capability. By embedding virtual workflows into the fabric of hospital systems, the platform supports sustainable scale rather than short-term experimentation.
Virtual Care Reduces Inpatient Stay By 4 Days
Virtual care platforms are changing how acute care gets delivered beyond hospital walls. Evidence from all-virtual acute care at home programs shows that organizations can safely shorten inpatient stays without compromising outcomes. For enterprise leaders, this signals a shift from capacity expansion to smarter care orchestration.
1. Shorter Length of Stay Without Clinical Tradeoffs
All-virtual acute care models demonstrate an average reduction of nearly 4 inpatient days per episode. Patients transition earlier from hospital beds to home-based virtual care environments. Importantly, this reduction does not come with a higher mortality risk.
For health systems, this directly impacts bed availability, surge readiness, and throughput. Fewer inpatient days mean hospitals can treat more acute cases without adding physical capacity.
2. Emergency Department Returns Decline
The same data shows a reduction in 30-day emergency department return visits. Patients supported through virtual acute care pathways appear less likely to escalate back to emergency settings.
This suggests that continuous remote oversight and structured follow-up reduce uncertainty after discharge. Virtual teams can intervene earlier when symptoms change, preventing unnecessary ED utilization.
3. Follow-Up Demand Shifts, Not Disappears
While ED visits decline, follow-up care does not vanish. The data indicates roughly a one-third increase in 30-day urgent care visits. This reflects a redistribution of care rather than a failure of the model.
From an enterprise perspective, this shift is predictable and manageable. Urgent care is lower cost, easier to staff, and better suited for virtual triage and escalation than emergency departments.
These outcomes highlight why virtual care must be designed as infrastructure. Organizations need systems that manage discharge, monitoring, escalation, and follow-up as a single continuum. Fragmented tools cannot coordinate this level of care safely.
Core Components of a Caregility-Like Virtual Care Infrastructure
A Caregility-like virtual care infrastructure combines secure clinical video, device integration, workflow orchestration, interoperability, and governance into a single enterprise platform that operates inside hospital environments.
Each component must work together as part of a clinical operating layer that supports inpatient care, remote teams, and centralized oversight. When one element is missing or loosely integrated, virtual care quickly breaks down under real-world hospital conditions.
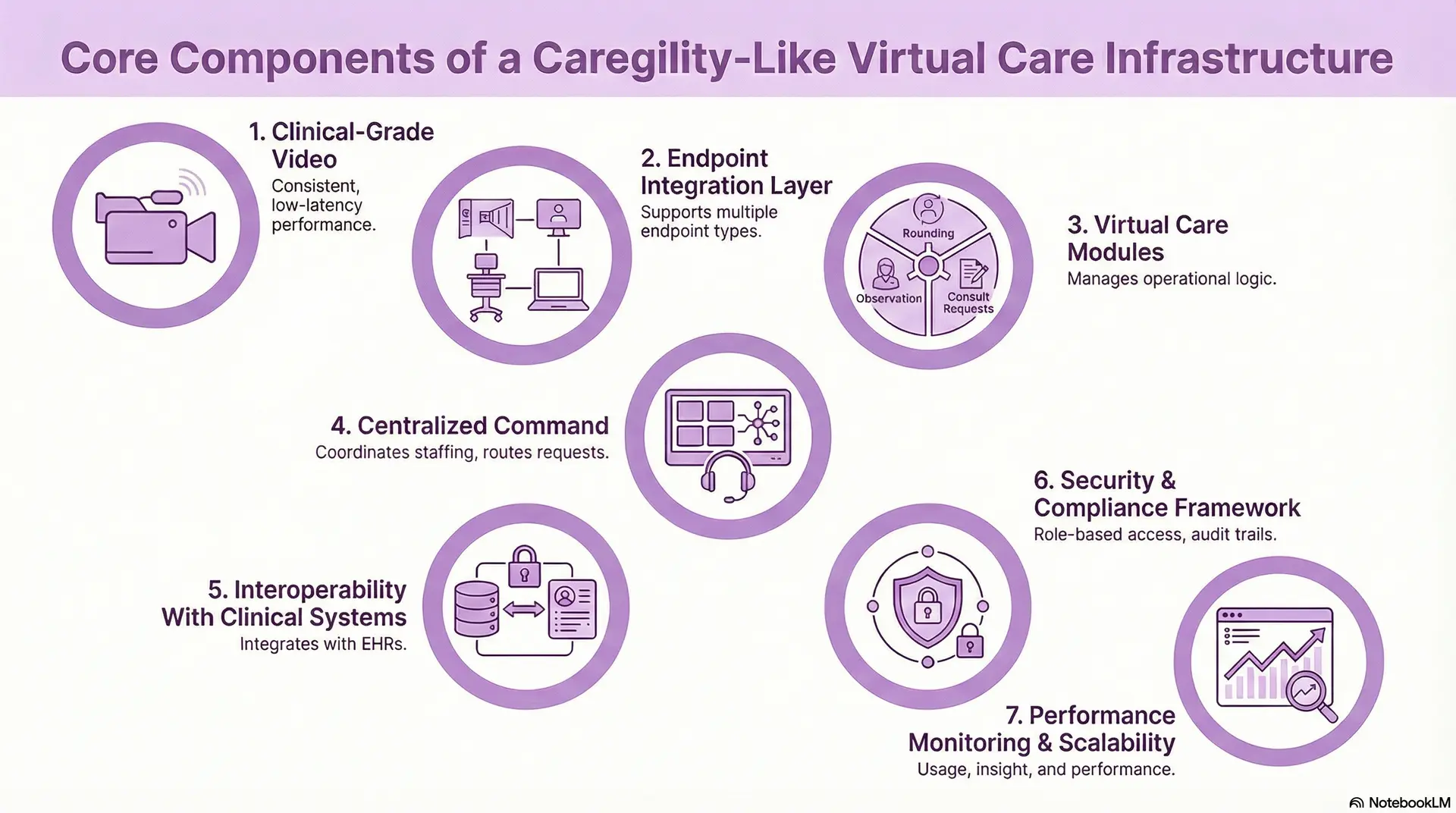
1. Clinical-Grade Video
This is the foundation of the entire infrastructure. The video layer must deliver consistent, low-latency performance across patient rooms, carts, command centers, and remote clinician devices. It must function reliably during peak usage, emergencies, and shift changes, without dropped sessions or degraded quality that erodes clinical trust.
2. Endpoint Integration Layer
A Caregility-like platform supports multiple endpoint types without forcing standardization on a single device vendor. Fixed room systems, mobile carts, bedside displays, and clinician laptops all connect through the same infrastructure.
This flexibility allows hospitals to scale the virtual care unit by unit while adapting to physical constraints.
3. Virtual Care Modules
Virtual care sessions should follow operational logic, not ad-hoc calling behavior. The platform must support scheduled rounding, continuous observation, consult requests, and escalation protocols.
These workflows ensure virtual care enhances coordination rather than creating parallel processes that clinicians must manage separately.
4. Centralized Command
Enterprise virtual care depends on visibility and control. Command centers coordinate staffing, route requests, and balance workload across remote clinicians.
This layer enables hospitals to extend scarce expertise across multiple units and facilities without overwhelming frontline teams.
5. Interoperability With Clinical Systems
Deep integration with EHRs and hospital systems is critical. Virtual care workflows should launch within existing clinical contexts, align with patient records, and support documentation practices.
Standards-based interoperability ensures the platform fits into enterprise IT architecture instead of operating in isolation.
6. Security and Compliance Framework
Role-based access, session logging, and audit trails must be native to the platform. These controls protect patient privacy while supporting clinical accountability.
When governance is embedded rather than bolted on, organizations can scale virtual care without increasing compliance risk.
7. Performance Monitoring and Scalability Controls
Enterprise deployments require continuous oversight. The platform must provide insight into usage, response times, uptime, and workflow performance.
These metrics guide optimization and support confident expansion across departments and locations.
A Caregility-like virtual care infrastructure succeeds because its components operate as a unified system. When video, workflows, governance, and interoperability are designed together, virtual care becomes a dependable part of hospital operations rather than a fragile add-on.
Virtual Care Use Cases Enabled by This Infrastructure
A Caregility-like virtual care infrastructure enables inpatient, acute, and hybrid care use cases by embedding virtual workflows directly into hospital operations and clinical decision-making.
1. Inpatient Virtual Rounding
Virtual rounding allows physicians and specialists to participate in daily inpatient rounds without being physically present on every unit. Through secure room-based video access, clinicians can assess patients, coordinate with bedside nurses, and make timely care decisions across multiple floors or facilities.
This model reduces rounding delays caused by physical movement or scheduling constraints. It also improves consistency in care delivery, especially in large hospitals where specialist availability is limited. Over time, virtual rounding helps standardize decision-making while preserving clinician oversight.
2. Continuous Remote Patient Observation
Remote observation enables centralized teams to monitor high-risk patients continuously for falls, confusion, or early signs of deterioration. Cameras placed in patient rooms connect to virtual observers who follow defined safety protocols and escalation rules.
This approach reduces reliance on one-to-one sitters while improving coverage consistency. It also allows hospitals to redeploy bedside staff to higher-value tasks. Most importantly, safety events are identified earlier, reducing adverse outcomes without increasing staffing costs.
3. Workforce Capacity Extension
Virtual nursing programs use remote clinicians to support bedside teams with admissions, discharges, medication education, and documentation tasks. These activities consume significant nursing time but do not always require physical presence.
By shifting these tasks to virtual nurses, hospitals relieve pressure on bedside staff and reduce burnout. This model also creates staffing flexibility during census spikes, overnight shifts, or periods of workforce shortage, without compromising patient experience.
4. On-Demand Specialty Consults
Virtual care infrastructure allows specialists to join patient care in minutes rather than hours. Neurology, psychiatry, infectious disease, and critical care teams can consult remotely, review patient context, and guide treatment decisions in real time.
This is especially valuable for smaller hospitals or rural facilities that lack full-time specialist coverage. Enterprise systems can centralize expertise and distribute it efficiently, improving outcomes while avoiding unnecessary patient transfers.
5. Centralized Command Centers
Command centers act as the operational nerve center of enterprise virtual care. From a single location, virtual teams oversee observation programs, consult requests, staffing allocation, and escalation workflows across multiple facilities.
This centralized visibility enables proactive intervention rather than reactive response. Leaders gain insight into capacity constraints, risk trends, and workflow performance, allowing faster decision-making at the system level.
6. Emergency and Surge Coverage
Virtual care infrastructure provides reliable clinical coverage during nights, weekends, and surge events. Remote clinicians step in when on-site staffing is limited, ensuring patients receive timely attention without requiring permanent staffing increases.
This capability helps hospitals maintain service levels during unpredictable demand. It also supports resilience planning, allowing systems to respond to emergencies without compromising safety or clinician well-being.
These use cases succeed because the infrastructure is designed for real hospital conditions. When virtual care is embedded into workflows, staffing models, and governance structures, it becomes a dependable extension of enterprise care delivery rather than a temporary workaround.
Architecture Of A Caregility-Like Virtual Care Infrastructure
A Caregility-like virtual care infrastructure uses a layered, enterprise architecture that combines endpoint devices, secure connectivity, workflow orchestration, interoperability, and governance to support inpatient and hybrid care at scale.
Below is how an infrastructure-first architecture is typically structured.
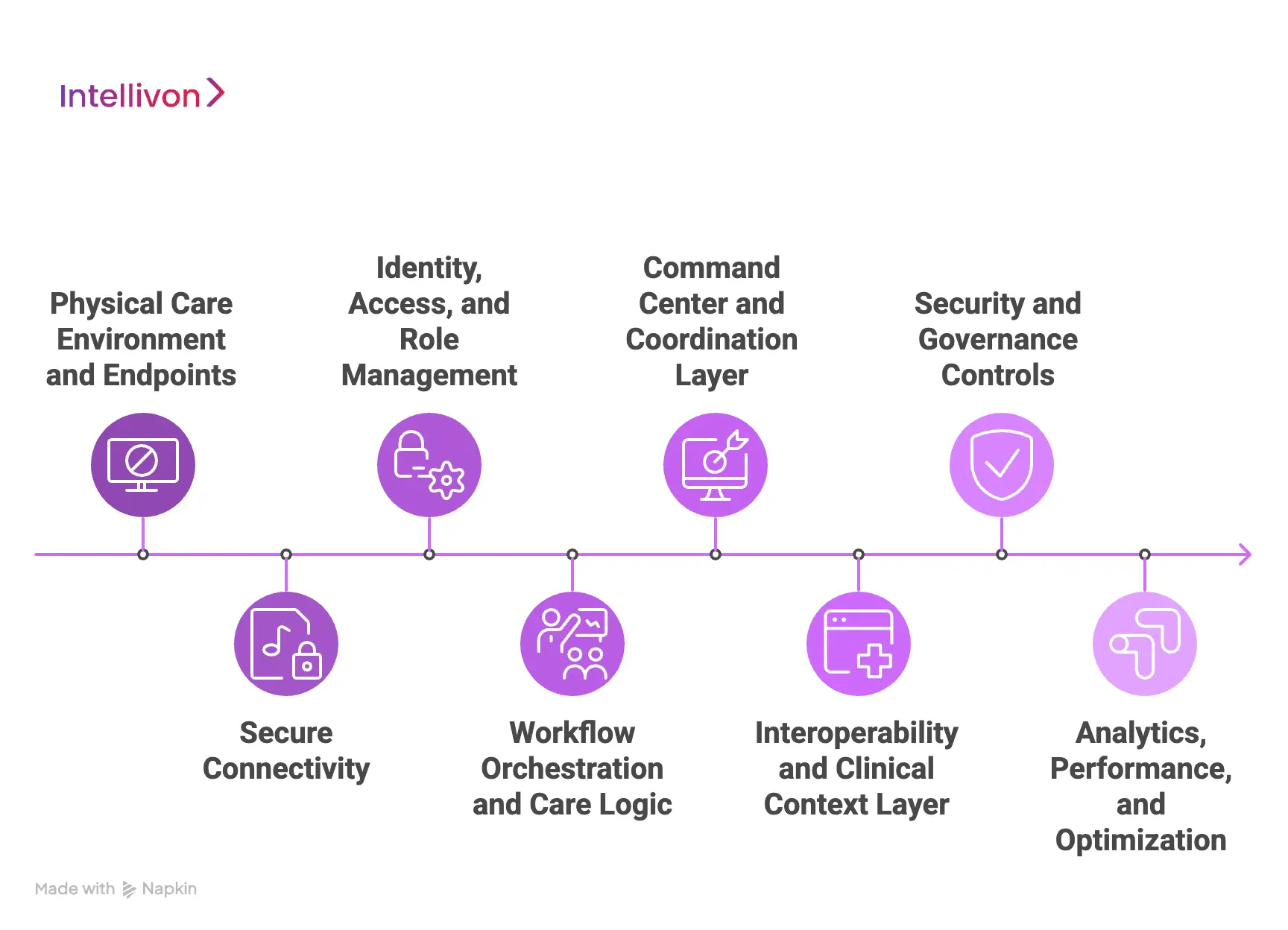
Layer 1: Physical Care Environment and Endpoints
This layer lives where care actually happens. It includes in-room cameras, microphones, bedside displays, mobile carts, and clinician devices. These endpoints are designed for continuous availability, not occasional use.
The key architectural principle here is flexibility. Hospitals deploy different device types based on unit needs, room layouts, and patient acuity. The infrastructure must support all of them without changing workflows or creating dependency on a single hardware vendor.
Layer 2: Secure Connectivity
Above the physical layer sits the secure communication fabric. This layer handles encrypted video, audio, and signaling between endpoints, command centers, and remote clinicians.
Low latency and high availability are critical. Sessions must remain stable during peak usage, shift changes, or emergency events. Redundancy, failover, and network optimization ensure that virtual care remains clinically reliable, not best-effort.
Layer 3: Identity, Access, and Role Management
This layer controls who can access what, when, and how. Clinicians, nurses, observers, and administrators authenticate through enterprise identity systems and are assigned role-based permissions.
Access rules align with clinical responsibilities. A virtual observer sees different information than a physician or specialist. This design protects patient privacy while maintaining operational clarity and accountability.
Layer 4: Workflow Orchestration and Care Logic
Workflow orchestration is where infrastructure becomes operational. This layer manages how virtual care sessions are triggered, routed, and escalated based on real clinical needs.
Rounding schedules, observation protocols, consult requests, and escalation rules are encoded into the system. As a result, virtual care follows predictable patterns that clinicians trust, rather than ad-hoc calls that create uncertainty.
Layer 5: Command Center and Coordination Layer
Command centers sit above individual workflows and provide system-wide visibility. Virtual teams monitor activity, assign coverage, manage queues, and intervene when thresholds are crossed.
This layer allows enterprises to centralize scarce expertise and distribute it across facilities. Leaders gain real-time insight into utilization, response times, and capacity constraints, enabling proactive management.
Layer 6: Interoperability and Clinical Context Layer
This layer connects virtual care to the rest of the hospital ecosystem. Integrations with EHRs, scheduling systems, and clinical applications provide patient context and workflow continuity.
Standards-based interoperability ensures that virtual interactions align with existing documentation and care processes. Virtual care becomes part of the clinical record rather than a parallel experience.
Layer 7: Security and Governance Controls
Governance runs across every layer. This includes session logging, access audits, data retention rules, and compliance reporting aligned with healthcare regulations.
By embedding governance into the architecture, hospitals can scale virtual care confidently. Risk does not increase as adoption grows, which is essential for enterprise deployment.
Layer 8: Analytics, Performance, and Optimization
The top layer focuses on insight and improvement. Usage patterns, response times, workflow outcomes, and operational metrics are tracked continuously.
These insights help organizations refine care models, justify investment, and guide expansion. Virtual care evolves based on evidence, not assumptions.
A Caregility-like virtual care infrastructure works because its architecture reflects real hospital operations. When layered correctly, the system delivers reliability, scalability, and governance together, turning virtual care into a durable enterprise capability rather than a fragile overlay.
AI Capabilities In A Caregility-Like Virtual Care Infrastructure
AI in a Caregility-like virtual care infrastructure supports routing, monitoring, and operational intelligence while keeping clinicians in control through governed, human-in-the-loop workflows.
1. Continuous Risk Detection
AI supports remote observation by identifying patterns that may signal patient risk. This includes prolonged inactivity, unusual movement, or deviations from expected behavior during observation windows.
Rather than triggering alarms automatically, the system flags situations for human review. Virtual observers and nurses validate the signal before escalation, preserving clinical judgment while enabling earlier intervention.
2. Context-Aware Virtual Care Triggers
AI models ingest signals from workflows, schedules, and monitoring systems to initiate virtual care interactions at the right moment. For example, a missed rounding window, delayed response, or repeated call requests can prompt proactive outreach.
This shifts virtual care from reactive to anticipatory. Care teams intervene before small issues escalate into clinical or operational problems.
3. Operational Intelligence
At the enterprise level, AI analyzes historical and real-time data to forecast demand for virtual care services. Leaders gain insight into expected observation load, consult volume, and staffing requirements.
These insights support smarter workforce planning and reduce reliance on last-minute staffing adjustments. Virtual care becomes more predictable and financially sustainable.
4. Clinical Decision Support
AI can surface relevant patient context during virtual interactions, such as recent vitals, risk scores, or care milestones. This information supports faster decision-making during consults or escalation events.
Critically, recommendations are advisory, not directive. Clinicians retain full authority, ensuring AI enhances care delivery without compromising accountability.
5. Governance and Model Oversight
Enterprise-grade AI requires continuous oversight. The platform monitors model performance, drift, and bias across patient populations and care settings.
Audit trails, override tracking, and periodic reviews ensure AI behavior aligns with clinical standards and regulatory expectations. This governance framework builds trust and supports long-term scalability.
AI strengthens virtual care infrastructure when it is applied with restraint and purpose. In a Caregility-like platform, AI improves coordination, visibility, and responsiveness while keeping clinicians firmly in control. This balance is what allows enterprises to scale virtual care safely and confidently.
How We Build A Caregility-Like Virtual Care Infrastructure
At Intellivon, we do not approach virtual care as a digital front end. We treat it as core healthcare infrastructure that must perform under real clinical pressure.
Our approach reflects how hospitals actually operate, how clinicians deliver care, and how enterprise systems scale without creating operational risk.
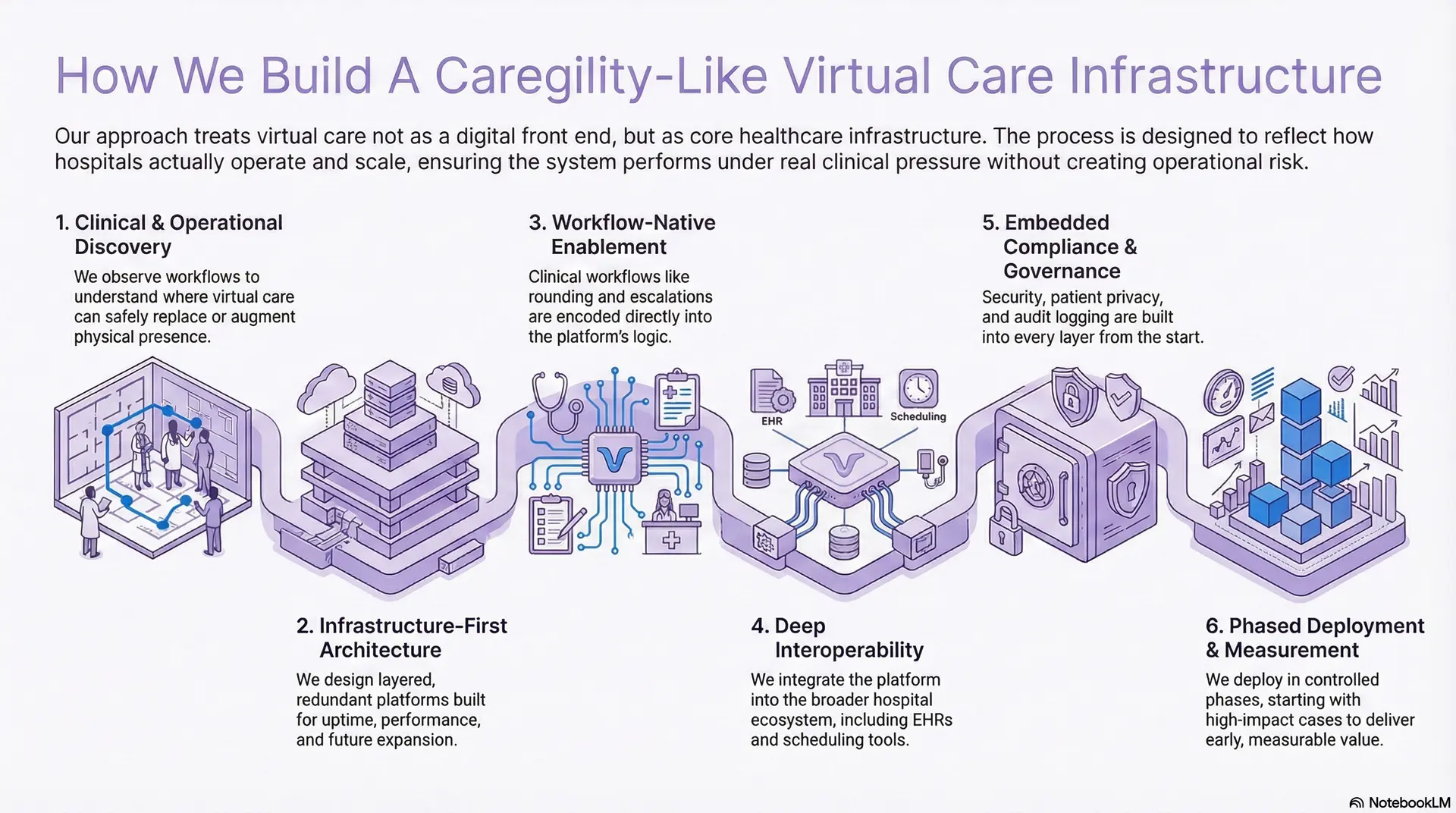
1. Clinical and Operational Discovery
We begin with deep discovery across inpatient units, nursing operations, command centers, and specialty services. This includes observing rounding workflows, escalation patterns, staffing models, and coverage gaps that exist today.
The goal is to understand where virtual care can safely replace physical presence and where it should augment it. This ensures the infrastructure supports clinical decision-making rather than introducing friction or unsafe shortcuts.
2. Infrastructure-First Architecture
Our architecture teams design layered platforms that separate endpoints, communication, workflows, and governance. This structure allows hospitals to expand virtual care without redesigning the system every time a new unit or facility is added.
We design for uptime, redundancy, and performance under peak load. The infrastructure is built to handle emergencies, shift changes, and simultaneous sessions without degradation.
3. Workflow-Native Virtual Care Enablement
We encode clinical workflows directly into the platform logic. Virtual rounding schedules, observation rules, consult pathways, and escalation triggers follow defined operational patterns.
This removes ambiguity for clinicians. Virtual care sessions start when they are needed, route to the right role, and escalate appropriately. Adoption improves because the system matches how care teams already work.
4. Deep Interoperability
Intellivon integrates virtual care into the broader hospital ecosystem. This includes EHRs, identity systems, scheduling tools, and clinical applications using standards-based interfaces.
Context travels with the interaction. Clinicians do not need to switch systems or duplicate documentation. IT teams retain architectural control while enabling seamless clinical workflows.
5. Compliance and Governance Embedded
Security and compliance are not added after deployment. We embed role-based access, audit logging, session governance, and data controls into every layer of the platform.
This ensures patient privacy, clinical accountability, and regulatory alignment as adoption grows. Organizations can scale virtual care without increasing compliance exposure.
6. Phased Deployment With Measurable Outcomes
We deploy virtual care infrastructure in controlled phases, starting with high-impact use cases such as observation, rounding, or virtual nursing. Each phase is measured against operational and clinical metrics.
This approach delivers early value, builds clinician confidence, and creates a clear path for enterprise-wide expansion without disruption.
Intellivon builds a Caregility-like virtual care infrastructure that holds up in real hospital conditions. By combining clinical insight, enterprise-grade architecture, and compliance-first execution, we help healthcare organizations turn virtual care into a long-term growth enabler, not a temporary workaround.
Cost to Build A Caregility-Like Virtual Care Infrastructure
Building a Caregility-like virtual care infrastructure does not require a multi-million-dollar commitment in the first phase. For healthcare enterprises that start with one or two high-impact inpatient workflows, such as virtual rounding, remote observation, or specialty consults, the platform can be delivered within a tightly controlled budget.
The deciding factor is not how many features are included, but how deliberately the infrastructure is phased. When virtual care is designed as a modular, infrastructure-first system, organizations can prove clinical and operational value before expanding scope.
At Intellivon, we align cost planning with leadership budget cycles, regulatory readiness, and near-term ROI. We focus on building a secure, hospital-ready core that can scale across units and facilities without rework.
Estimated Phase-Wise Cost Breakdown
| Phase | Description | Estimated Cost (USD) |
| Clinical & Operational Discovery | Inpatient workflow mapping, use-case prioritization, staffing and escalation analysis, and regulatory scoping | 6,000 – 12,000 |
| Infrastructure Architecture & Blueprint | Endpoint strategy, network planning, workflow orchestration design | 8,000 – 15,000 |
| Core Virtual Care Platform Development | Secure video layer, session orchestration, role-based workflows | 15,000 – 35,000 |
| Device & Endpoint Integration | Room devices or carts, clinician endpoints, provisioning workflows | 6,000 – 12,000 |
| Interoperability & Identity Integration | EHR context launch, SSO, role-based access alignment | 8,000 – 15,000 |
| Security & Compliance Controls | Encryption, audit logs, access governance, compliance validation | 6,000 – 10,000 |
| Testing, QA & Clinical Validation | Workflow testing, performance checks, and clinician sign-off | 5,000 – 8,000 |
| Pilot Deployment & Training | Live unit rollout, clinician onboarding, optimization | 6,000 – 10,000 |
Total Initial Investment Range: USD 50,000 – 150,000
This investment supports a hospital-grade virtual care infrastructure deployed for one or two inpatient pathways, operating inside a live clinical environment with enterprise security and governance in place.
Annual Maintenance and Optimization
Ongoing costs cover infrastructure hosting, security monitoring, device management, and integration upkeep.
- 10–15% of the initial build cost annually
- Approx. USD 6,000 – 20,000 per year
Predictability is highest when interoperability and compliance are engineered correctly from the beginning.
Cost Variables to Plan for During Scale
As adoption grows, additional costs may arise from:
- Expanding to more inpatient units or facilities
- Adding virtual nursing, observation, or command center coverage
- Increased device footprint and video usage
- Regulatory audits and documentation updates
- Advanced analytics or AI-assisted workflows
Planning for these early prevents budget pressure during expansion.
How Enterprises Stay Within the USD 50K–150K Range
Healthcare organizations that control virtual care infrastructure costs typically:
- Start with one clearly defined inpatient use case
- Avoid multi-facility or multi-region complexity in phase one
- Use modular architecture to expand incrementally
- Enforce security and compliance from day one
- Measure adoption, response times, and ROI in the first 90 days
This approach ensures the platform proves both clinical and financial value before larger capital deployment.
Talk to Intellivon’s healthcare platform architects to receive a phased cost estimate aligned with your enterprise growth strategy.
Conclusion
Virtual care has moved beyond experimentation. Platforms like Caregility show that when virtual capabilities are built as infrastructure, they unlock capacity, extend clinical reach, and strengthen operational resilience across the enterprise.
For healthcare leaders, the opportunity is not simply to reduce costs, but to redesign how care is delivered at scale. With the right architecture, governance, and execution partner, virtual care becomes a growth enabler that supports better outcomes, workforce sustainability, and long-term system performance. Intellivon brings the clinical insight and enterprise-grade engineering needed to make that transition work in real hospital environments.
Build Your Virtual Care Infrastructure Like Caregility With Intellivon
At Intellivon, we build a virtual care infrastructure that operates as part of hospital operations, not as an overlay or standalone tool. Our platforms are designed to function inside inpatient units, command centers, and hybrid care environments, enabling virtual rounding, observation, consults, and workforce extension through a single governed system.
Each solution is engineered for enterprise healthcare delivery. Platforms are infrastructure-first, compliant by design, resilient under continuous clinical load, and built to deliver measurable operational and financial ROI as virtual care expands across units and facilities.
Why Partner With Intellivon?
- Infrastructure-first virtual care design aligned with inpatient workflows, command centers, and enterprise governance
- Deep interoperability expertise across EHRs, identity systems, HL7, FHIR, and secure enterprise APIs
- Compliance-first architecture supporting HIPAA, GDPR, role-based access, audit trails, and clinical accountability
- AI-enabled operational intelligence for routing, workload balancing, observation support, and performance analytics
- Scalable, cloud-native delivery with phased rollout control, redundancy planning, and continuous optimization
Book a strategy call to explore how a Caregility-like virtual care infrastructure can extend clinical capacity, strengthen governance, and support long-term enterprise growth.
FAQs
Q1. What is a Caregility-like virtual care infrastructure?
A1. A Caregility-like virtual care infrastructure is an enterprise platform that embeds secure video, remote clinical workflows, and command-center operations directly into hospital environments. It supports inpatient, acute, and hybrid care delivery at scale.
Q2. How is virtual care infrastructure different from telehealth software?
A2. Telehealth software focuses on scheduled virtual visits. Virtual care infrastructure supports continuous inpatient workflows such as rounding, observation, consults, and virtual nursing, integrated into hospital operations and governance systems.
Q3. Can a Caregility-like platform integrate with existing EHR systems?
A3. Yes. Enterprise virtual care infrastructure integrates with EHRs using standards such as HL7 and FHIR. This allows clinicians to launch virtual sessions within clinical context while keeping documentation and workflows aligned.
Q4. How long does it take to build a Caregility-like virtual care platform?
A4. For one or two high-impact inpatient use cases, a Caregility-like platform can typically be built and deployed within three to five months. Timelines depend on workflow complexity, integrations, and compliance readiness.
Q5. Is building a virtual care infrastructure cost-effective for hospitals?
A5. When phased correctly, virtual care infrastructure reduces inpatient length of stay, improves workforce utilization, and increases system capacity. These operational gains often offset build costs within the first year of deployment.



