Key Takeaways:
-
AI revenue optimization connects EHR, payer contracts, claims, remittance, coding, and finance data together.
-
Revenue leakage detection, underpayment recovery, denial prediction, and charge capture gap analysis are core features.
-
FHIR R4 APIs, EDI 837/835 workflows, HIPAA controls, MLOps, and audit logs are mandatory requirements.
-
Custom builds cost $60,000 to $220,000 with 6 to 18 months, depending on enterprise rollout scope.
-
How Intellivon builds AI revenue optimization as production infrastructure, not a standalone reporting dashboard.
If you need your company’s revenue to be optimized, the first question you need to ask is whether the claims are being paid correctly. AI revenue optimization software is the infrastructure that answers it, which scans every remittance against every contracted rate, surfacing where payers paid less than they owed, and building the recovery case automatically.
Standard RCM tools catch denials, but they are not built to catch underpayments, which are payments that look correct on the surface yet fall short of what the contract requires. That distinction matters because underpayments can quietly erode collections by up to 11%. The fix for undetectable underpayments is a machine-readable contract layer that translates fee schedules and payer rules into structured data the platform can compare against every remittance. Build that layer in, and health systems have documented 8% reimbursement increases through AI-backed contract intelligence within the first year.
Intellivon has been building AI revenue systems at this depth for over ten years, with explainability designed in from the start, so every recommendation can be audited and defended. This blog extensively covers all corners of building such software, including the ML architecture, payer contract intelligence design, EHR compliance controls, and the actual development steps we follow.
What Is AI Revenue Optimization Software in Healthcare?
AI revenue optimization software is a specialized financial platform that stops hospital revenue from slipping through the cracks. It connects your clinical data directly to your billing cycle. Because of this integration, the system instantly spots underpayments, coding mistakes, and unfair insurance denials.
Several hospitals lose a lot of revenue and ROI every year simply because their legacy billing software cannot read complex insurance rules. This platform fixes that issue by finding hidden financial leaks automatically. Consequently, health systems collect every dollar they earn without adding manual administrative work.
How It Differs From AI RCM Software
Traditional AI RCM software focuses strictly on automating standard billing tasks like scheduling, eligibility checks, and basic claim submission. In contrast, AI revenue optimization software operates as an advanced intelligence layer that finds hidden revenue leaks across your entire financial ecosystem.
Therefore, it solves systemic underpayments and contract variances rather than just processing claims faster.
| Capability | Standard AI RCM Software | AI Revenue Optimization |
| Primary Focus | Task automation and workflow speed | Leakage discovery and margin recovery |
| Data Scope | Standard billing and clearinghouse data | Deep clinical, contract, and remittance data |
| Core Value | Lowers the administrative cost of collecting | Maximizes the total net collection rate directly |
Because of these differences, standard RCM platforms often miss complex coding gaps and payer contract non-compliance entirely. Implementing revenue optimization ensures you actually collect the full amount your health system is legally owed.
Where It Fits in the Healthcare Revenue System
This software operates as an intelligent overlay that sits directly above your existing core infrastructure. It does not replace foundational platforms like Epic, Oracle Health/Cerner, athenahealth, or Meditech. Instead, it extracts data from those systems to provide a centralized financial intelligence layer.
The platform integrates deeply across your entire financial and clinical software ecosystem:
- EHR and PM Systems: It extracts unstructured clinical notes and schedules to perform charge capture gap analysis and detect undercoding.
- Clearinghouses and Claims Engines: The platform monitors claim files before submission to run real-time allowed amount verification and predictive modeling.
- Contract Management and ERPs: It checks paid claims against digital fee schedules to run complex contract rate variance analysis.
- Analytics and Dashboards: It feeds clean, processed financial data into your executive systems for accurate ML revenue forecasting.
Revenue optimization software becomes valuable when it can prove where money is leaking, why it is leaking, and what action can recover it. That requires a broader architecture than a dashboard. The next section will map the exact revenue leakage points the platform must detect.
6 Revenue Leakage Sources That AI Revenue Optimization Software Targets
The six sources (underpayment, charge capture gaps, payer contract variance, denial clustering, HCC risk adjustment gaps, and prior authorization approval rate) require different ML model types and different data inputs.
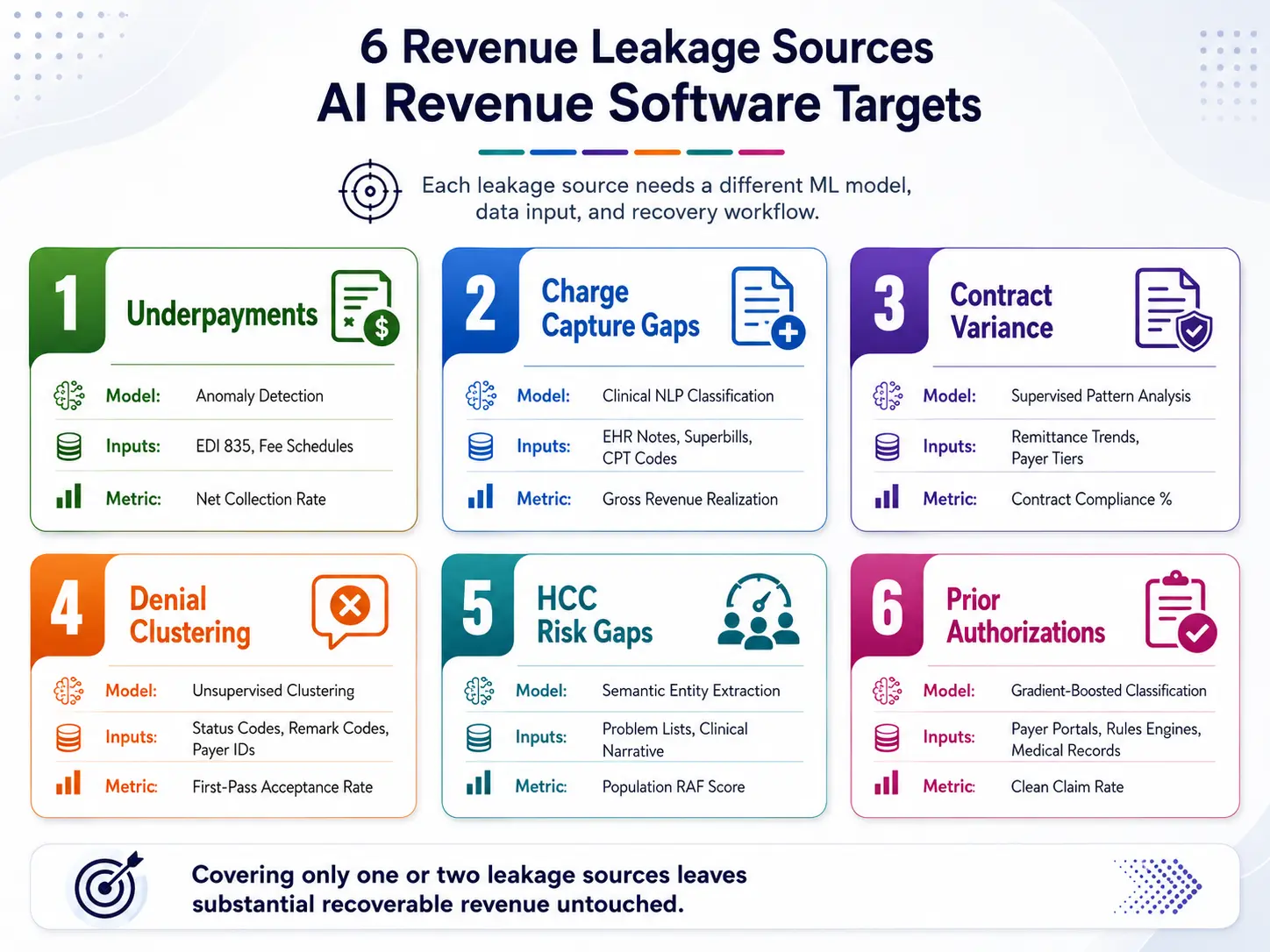
AI revenue optimization software must address all six principal leakage sources to produce meaningful net collection rate improvement. Addressing only denial management or only underpayment detection leaves the majority of recoverable revenue untouched.
| Leakage Source | Core ML Model Type | Primary Data Inputs Required | Target Financial Metric |
| 1. Underpayments | Anomaly Detection | EDI 835 Remittance, Digital Fee Schedules | Net Collection Rate |
| 2. Charge Capture Gaps | Clinical NLP Classification | Unstructured EHR Notes, Superbills, CPT Codes | Gross Revenue Realization |
| 3. Contract Variance | Supervised Pattern Analysis | Historical Remittance Trends, Payer Tiers | Contract Compliance Percentage |
| 4. Denial Clustering | Unsupervised Clustering | Claim Status Codes, Remark Codes, Payer IDs | First-Pass Acceptance Rate |
| 5. HCC Risk Gaps | Semantic Entity Extraction | Problem Lists, Clinical Narrative Text | Population RAF Score |
| 6. Prior Authorizations | Gradient-Boosted Classification | Payer Portals, Rules Engines, Medical Records | Clean Claim Rate |
1. Underpayment Detection
Underpayment detection compares the actual payment on each EDI 835 remittance against the contracted allowed amount for the service, payer, and contract tier.
The ML model flags claims where the variance exceeds a defined threshold and clusters systematic underpayments by payer, procedure code, and facility to distinguish pricing errors from isolated adjudication anomalies.
- Technical Model Architecture: The system deploys isolation forests or customized anomaly detection algorithms directly onto your incoming EDI 835 payment remittance streams.
- Data Integration Layer: It cross-references transaction data against a normalized SQL database containing your specific, multi-tiered commercial payer contract fee schedules.
- The Underlying Industry Gap: Most existing RCM tools store complex insurance contracts as flat PDF documents or static spreadsheet uploads. Because of this structural limitation, legacy software cannot perform dynamic, claim-level contract rate variance analysis when a partial payment occurs.
2. Charge Capture Gap Analysis
Charge capture gap analysis detects services delivered but not billed, and codes assigned at a lower complexity level than the documentation supports.
NLP models parse clinical documentation and compare it against the codes submitted, flagging undercoding at the encounter level before the claim is finalized, and not after it is paid.
- Technical Model Architecture: This component uses Natural Language Processing (NLP) named entity recognition models trained specifically on clinical terminology to evaluate documentation complexity.
- Targeted Detection Areas: The system uncovers Evaluation and Management (E&M) undercoding mismatches, completely absent add-on procedures, and undocumented medical supplies.
- Real-World Financial Impact: For example, published case studies from Topflight show NLP-driven medical coding software successfully surfaces 7.9% more valid billable codes than standard human reviews. Consequently, across a large $100M healthcare organization, a minor 3% to 5% coding accuracy improvement yields $3M to $5M in recovered capital every year.
3. Payer Contract Variance
Payer contract variance detection identifies cases where payers consistently pay below the contracted rate for specific procedure codes, modifier combinations, or service categories.
The model distinguishes pricing errors from coverage denials and routes contract variance cases to a separate recovery workflow.
- Technical Model Architecture: It utilizes supervised classification models combined with statistical process control to monitor ongoing payer adjudication behavior over time.
- Targeted Detection Areas: The system maps procedure-specific underpayment spikes by commercial payer, uncovers modifier-related remittance errors, and flags deviations in stop-loss calculations for complex ICU cases.
- Business Deliverable Output: Therefore, instead of generating simple, uncoordinated worker tasks, the system provides aggregated, legally audit-ready data packets. These reports give your executive leadership concrete evidence of systemic payer non-compliance to use during contractual renegotiations.
4. Denial Pattern Detection
Denial pattern detection clusters denied claims by root cause, and identifies payer-specific denial patterns that indicate systematic adjudication behavior rather than one-off claim issues.
The model prioritizes denial clusters by recoverable revenue value, routing high-value clusters to appeals automation and low-value clusters to write-off analysis.
- Technical Model Architecture: This engine applies unsupervised machine learning algorithms, such as K-Means or DBSCAN clustering, directly across your historic denial code registries.
- The Predictive Upgrade: Traditional billing teams analyze claims one by one as they arrive. Conversely, an ML model scans 50,000 transactions simultaneously to identify hidden trends, such as an insurance company intentionally denying specific orthopedic modifiers.
- Proven Operational Targets: According to industry studies published by the Healthcare Financial Management Association (HFMA), health systems using advanced machine learning pattern detection routinely achieve an 18% to 30% reduction in overall denials within the first year of production.
5. HCC Risk Adjustment Gaps
HCC (Hierarchical Condition Category) risk adjustment gaps represent revenue loss specific to value-based care contracts where reimbursement is tied to the documented risk score of the patient population.
If chronic conditions are present in the clinical record but not captured in the submitted diagnosis codes, the patient’s RAF (Risk Adjustment Factor) score is understated, and the capitation payment is lower than the clinical complexity justifies.
- Technical Model Architecture: It employs specialized clinical language transformers to parse text fields within electronic health records for implicit chronic disease mentions.
- Required Data Points: The system ingests historical unstructured physician notes, active outpatient problem lists, past encounter diagnostic history, and complete longitudinal claims data.
- Strategic Relevance for Founders: This is critical for groups running Medicare Advantage panels, Accountable Care Organizations (ACOs), or shared-risk payment models. For instance, a health network managing a $500M portfolio with an unaddressed 5% HCC omission gap leaves an estimated $10M to $25M in justified funding unclaimed due to simple coding documentation deficits.
6. Prior Authorization Approval Rate
Prior authorization approval rate optimization reduces the volume of services that reach billing without authorization and increases the approval rate for authorizations submitted for high-value procedures.
The ML model predicts authorization denial probability at submission time, triggers clinical documentation supplementation for high-risk requests, and routes borderline cases to clinical staff for enhancement before payer review.
- Technical Model Architecture: It uses a gradient-boosted decision tree classifier trained on historical authorization outcomes, clearinghouse transactions, and insurance rulesets.
- The Preventive Value: Medical procedures performed without a confirmed insurance approval token cannot legally be billed to a commercial payer.
- Revenue Protection Scale: By boosting your prior authorization approval rate by just 10 percentage points across expensive specialties like oncology or advanced imaging, a mid-sized healthcare delivery network successfully insulates $2M to $8M in annual operating margins from total forfeiture.
Each leakage source requires a different model, different data inputs, and a different recovery workflow. Building a platform that addresses one or two of these sources leaves the majority of recoverable revenue unaddressed.
Which Revenue Leak Should You Automate First?
The first revenue leak to automate should be selected by recoverable cash value, evidence quality, payer repeatability, time-to-cash, workflow effort, and compliance exposure, not by the largest estimated loss.
You should fund the workflow where AI can prove a payment gap, route an action, support recovery, and measure posted cash within a defined period.
1. Large Revenue Leaks Aren’t Always the Best First Step
A high leakage estimate does not automatically justify first-phase automation. Charge capture gaps, coding opportunities, denials, underpayments, write-offs, and bad debt each require different evidence, review effort, and compliance controls.
- Suspected vs. Recoverable Cash: An AI model can flag a massive financial opportunity without proving it can actually be collected.
- The Documentation Trap: Coding or HCC-related gaps look highly lucrative but require intense clinical verification, certified coder reviews, and high compliance scrutiny.
- The Underpayment Advantage: Commercial payer underpayments are often much easier to defend because they rely on hard math, digital contract terms, and ERA 835 remittance data.
A 2026 Oliver Wyman RCM survey found that 92% of respondents believe there are no-regret AI investments in revenue cycle management. However, hospital leaders rarely agree on one dominant first use case because individual organizational gaps vary widely.
The smaller underpayment category becomes the stronger first Minimum Viable Product (MVP) because it produces cash faster with minimal friction.
At Intellivon, we map each revenue opportunity against available evidence, review ownership, and compliance risk before recommending an MVP scope. That evaluation becomes practical when each leakage category receives a measurable prioritization score.
2. Rank Revenue Leaks by Recoverability Factor
A CFO-grade prioritization model converts each revenue leakage category into a comparable investment decision. This prevents leadership from funding high-volume software alerts that never actually become collected revenue.
Our framework, Intellivon’s Recoverability-Weighted MVP Scoring Model, evaluates the following key factors:
- Expected Recoverable Cash (25%): Focuses strictly on collectible revenue rather than unverified system noise.
- Evidence Quality (20%): Assesses contract clauses, claim lines, and payment rules to ensure your staff can defend the recovery action.
- Pattern Repeatability (15%): Measures frequency across payers or codes to prove if fixing one pattern creates scalable value.
- Compliance Exposure (15%): Examines risk of unsupported coding or audit concerns to prevent unsafe revenue recommendations.
- Time-to-Cash (10%): Pinpoints appeal deadlines and payer response cycles to favor quick financial returns.
- Workflow Effort (10%): Evaluates internal reviewer hours to ensure automated queues do not overwhelm your team.
- Strategic Payer Value (5%): Tracks contract renewal timing to support long-term payer negotiation strategies.
To use this framework, teams score each leak category from 1 to 5 for every factor. The platform then balances these variables using a direct calculation:
3. Compare Revenue Leakage Categories
Revenue leakage categories must be compared directly using the evidence they require, the cash they can recover, and the operational risk they create.
| Revenue Leakage Category | Evidence Needed Before Automation | Recoverability Potential | Compliance Risk | Operational Effort | Likely MVP Priority |
| Payer Contract Underpayments | Contract terms, digital fee schedules, EDI 835 logs | High | Low to Moderate | Moderate | Strongest First MVP |
| Denial Pattern Prevention | Claim history, CARC/RARC codes, payer rules | Medium to High | Low | Moderate | Strong alternative |
| Charge Capture Gaps | Clinical notes, orders, procedure logs, and bills | High | Moderate | High | Later Phase |
| Coding Accuracy | Documentation, CPT, ICD-10-CM, E&M rules | Medium to High | High | High | Later Phase |
| Zero-Balance Recovery | Closed accounts, adjustment logs, remittances | Medium | Low | Moderate | Secondary MVP |
| HCC Risk Optimization | Clinical narratives, problem lists, and ICD codes | High | Very High | High | Requires strict governance |
This matrix simplifies your implementation roadmap.
Intellivon uses this exact comparison to narrow your initial build to one clear focus area. This allows the platform to establish measurable recovery evidence before expanding into broader workflows.
The selected workflow still needs a baseline, because an AI alert cannot be counted as recovered revenue.
4. Define the Baseline and Success Metrics
The MVP should not begin until finance leaders know the current leakage baseline and the metric that will prove improvement.
- Establish an Industry Standard: We utilize the HFMA MAP Keys to create a reliable performance baseline across claims, account resolution, and financial management.
- Ignore Empty Activity Metrics: Simple software activity metrics, like the number of alerts generated or accounts scanned, do not prove ROI.
- Track Real Financial Outcomes: The system must track actual cash posted after an alert is created.
| MVP Metric | What It Measures | Why the CFO Needs It |
| Validated Leakage Value | Dollar value confirmed by reviewer evidence | Separates credible opportunities from weak AI flags |
| Recovered Cash Posted | Additional reimbursement actually received | Establishes realized financial return on the build |
| Recovery Rate by Payer | Recovered dollars divided by validated variance | Shows which payer patterns deserve platform expansion |
| Median Days to Cash | Time required to produce a financial return | Supports future rollout scheduling and staffing decisions |
| Reviewer Hours per Dollar | Staff cost of acting on machine findings | Protects your core cost-to-collect targets |
| Protected Revenue | Overpayment risk or compliance errors avoided | Shows compliance value separately from cash gains |
We recommend a strict 90-day validation window after deployment to track these metrics. The system must log whether every alert was accepted, appealed, recovered, or dismissed.
Once leadership selects the highest-value, lowest-risk workflow and defines proof of success, the platform architecture can be designed around evidence, recovery actions, and financial accountability.
AI revenue optimization should begin with the revenue leak that can be proven, recovered, measured, and governed, not the category with the loudest loss estimate. That is exactly how we do it at Intellivon. We ensure a recoverability-weighted scoring model gives CFOs a practical method to choose the first MVP without overbuilding the platform or creating avoidable compliance exposure.
Turning Government Data Into Real Negotiating Power in 2026
New government laws have changed how hospitals talk to insurance companies. Instead of viewing transparency rules as a boring paperwork headache, smart leaders use this data to win better insurance deals.
Putting this public information into a simple AI system gives your hospital network a huge advantage when it is time to renew your contracts.
1. What Changed with the Rules
The law now forces hospitals to show exactly what insurance companies pay them. Because of this, insurance companies can no longer hide their rates to keep your payments low.
The government rules say files must include:
- Exact Dollar Ranges: Hospitals must show the middle payment rate, the lowest 10% rate, and the highest 90% rate in clear dollar amounts.
- Proof of Invoices: Files must list the exact number of past bills used to calculate those averages, proving the math is correct.
- ID Codes: Every hospital must link these payment rates directly to their official National Provider Identifier (NPI) numbers.
- Boss’s Signature: The hospital CEO or President must sign a paper proving all the data is 100% correct.
As a result, what used to be messy paperwork is now a clean, easy-to-search list of insurance prices.
2. How AI Software Uses This Data to Help You
The law forces health insurance companies to publish all their rates online. This means you can easily see what your competitors are getting paid. By putting this public data into a custom AI tool, you turn raw files into direct power for your team.
The software handles the data in a few clear steps:
- Step 1: The software securely reads your current insurance contracts and past receipts.
- Step 2: The system automatically downloads the public payment data from rival hospitals.
- Step 3: The AI matches identical medical codes and cleans up confusing or messy insurance plan names.
- Step 4: The tool compares your actual payments against what your competitors are making nearby.
- Step 5: The screen flags exactly which insurance contracts pay you less than the market average.
This simple process gives your team real answers. For example, if the software shows that a nearby hospital gets paid 40% more for the exact same knee surgery, your team can demand equal pay using hard proof. Ultimately, custom AI tools turn government rules into extra cash for your business.
How to Build AI Revenue Optimization Software Healthcare Teams Can Trust
To build AI revenue optimization software healthcare teams can trust, start with revenue leakage scope, data access, payer contract structure, workflow owners, compliance controls, model strategy, integration design, and KPI baselines. The strongest MVP does not automate the whole revenue cycle. Instead, it proves recovery value in one or two high-impact leakage categories.
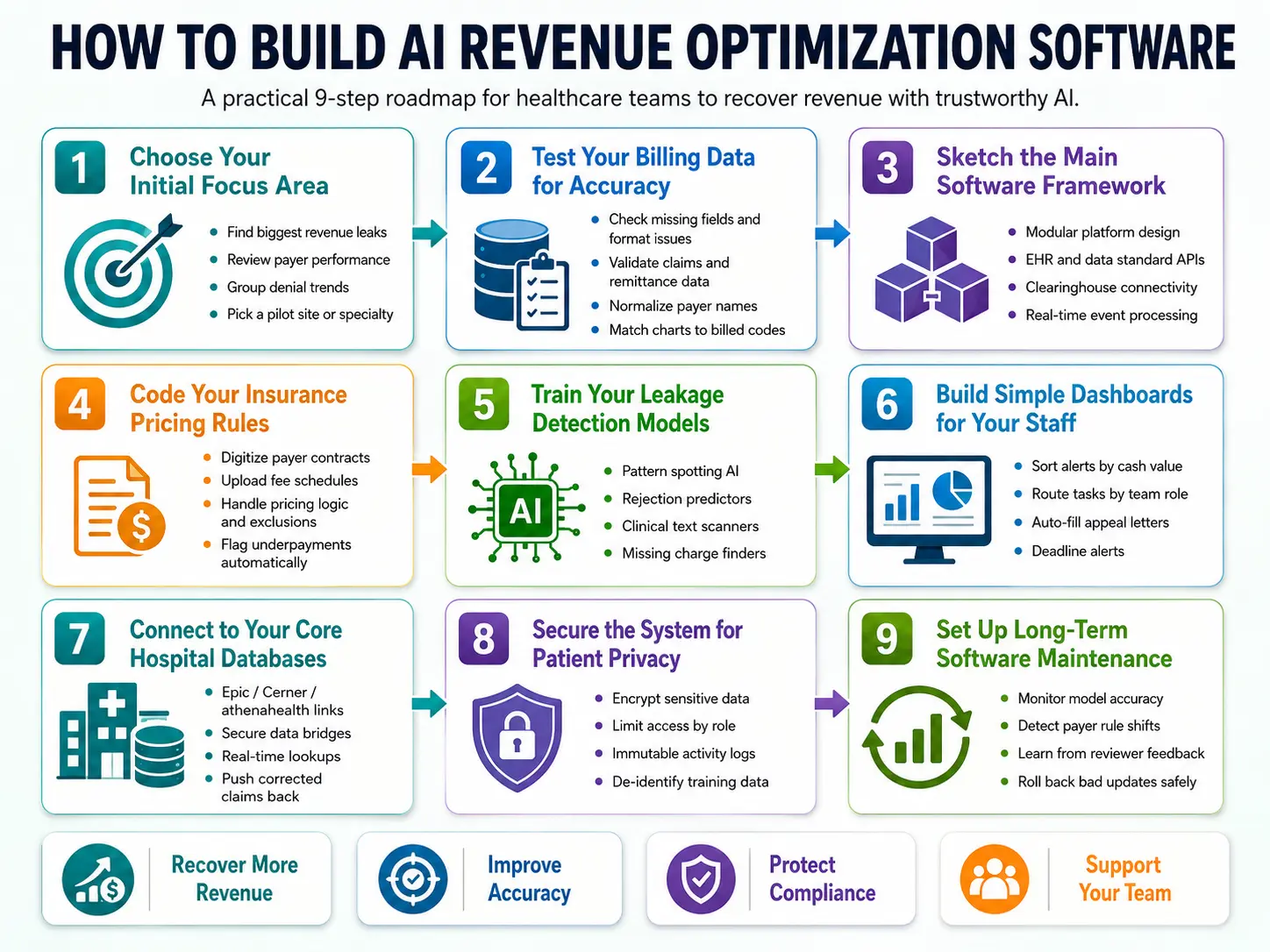
1. Choose Your Initial Focus Area
The first step is to pick one or two specific areas where your hospital is losing money. We call this building a Minimum Viable Product (MVP). Instead of trying to optimize every single invoice, you focus the software on an isolated, high-impact problem like underpaid insurance claims.
To set this up, the tech team will handle the following planning steps:
- Review your current billing performance to locate the biggest cash leaks.
- Sort your bills by insurance company to see which payers cause the most trouble.
- Group old rejections by their error codes to find recurring denial trends.
- Pick a single hospital location or medical specialty to use as a test site.
At Intellivon, we look at your daily claim volume and your staff’s manual workload before writing any code. We find that starting small prevents your team from getting overwhelmed by automated alerts. Once your target is clear, you must verify that your database is actually ready for an AI upgrade.
2. Test Your Billing Data for Accuracy
Your software will fail if your records are missing critical information. Before building anything, you must run a deep check on your past invoices, insurance rules, and doctor notes to ensure the data is complete and clean.
This verification phase requires these specific tasks:
- Scan your database to find blank boxes or formatting mistakes in old files.
- Build code to read standard digital health files like bills and payment receipts.
- Group all the different names for the same insurance company under one clear label.
- Double-check that the treatments listed in patient charts match your final bills.
We check your source data for missing pieces and format conflicts before moving forward. This screening step stops the AI from generating incorrect alerts that waste your staff’s time. After your data passes the test, your team can design the core framework of the platform.
3. Sketch the Main Software Framework
The main software framework acts like a traffic cop for your data. It must safely pull information out of your current billing tools, process it through the AI, and send clean action lists to your team without breaking your daily operations.
Your development team will set up these infrastructure layers:
- Build the platform as a collection of small tools that talk to each other safely.
- Use modern data standards to securely pull text from your electronic health records.
- Connect the software directly to the clearinghouses that route your insurance claims.
- Program the system to run its checks the exact second a new receipt arrives online.
We separate the data gathering tools from the AI logic and the user dashboards. This independent design means you can upgrade your machine learning models in the future without messing up your main data pipelines. Next, you need to teach the software how to read your insurance contracts.
4. Code Your Insurance Pricing Rules
This layer is where the software learns to spot math errors. The system needs to calculate exactly what an insurance company owes you for a specific treatment before a human clerk looks at the check.
Your engineers will build these calculation rules into the tool:
- Convert complex, legal insurance contracts into organized database tables.
- Upload your regional medical price sheets into a central digital index.
- Program rules to handle multi-procedure discounts and custom pricing exclusions.
- Set the software to flag an invoice the moment a payment comes up short.
We build this contract layer using clear mathematical formulas rather than a mysterious, hidden AI model. This means your billing clerks can always click an alert and see the exact math calculation behind every single underpayment warning. Once these basic rules are live, you can deploy advanced AI to catch complex patterns.
5. Train Your Leakage Detection Models
Static billing rules can easily miss hidden financial trends, such as an insurance company slowly delaying payments for a specific medicine. This step is where you train machine learning models to spot subtle billing anomalies across your entire network.
Your data science team will implement these specific models:
- Pattern Spoting AI: Deploys models to find unusual payment drops across plans.
- Rejection Predictors: Reviews old data to guess if a claim will be denied.
- Text Scanners: Uses language AI to read doctor notes and find treatment proof.
- Missing Charge Finders: Catches situations where care was given but never billed.
We link every single AI prediction directly to hard evidence, a dollar estimate, and a confidence score. This total openness helps your finance team trust the machine instead of ignoring its warnings. However, finding a mistake only matters if your team has a clear way to fix it.
6. Build Simple Dashboards for Your Staff
The software must turn its complex data findings into clear, easy-to-read to-do lists for your hospital staff. If the AI finds an underpayment, it needs to route that specific issue directly to the worker who handles that exact insurance company.
Your developers will create these simple workflow features:
- Organize all billing alerts into digital lists sorted by total cash value.
- Route coding errors to coders and insurance math problems to contract teams.
- Automatically fill out insurance appeal letters with the required medical proof.
- Add a live countdown timer to warn your team before an appeal deadline expires.
We build review screens that keep your human experts in total control. The software does the heavy lifting by gathering the proof and sorting the clutter, leaving your team free to secure your cash. Next, the tool must link directly with your existing hospital databases.
7. Connect to Your Core Hospital Databases
To work efficiently, the new software must plug directly into platforms like Epic, Cerner, or athenahealth. This connection allows the AI to read clinical records and update account balances automatically.
Your tech team will build secure data bridges to these external platforms:
- Connect directly to your primary health records to read daily clinical logs.
- Set up automated folders to safely ingest incoming and outgoing financial files.
- Route corrected claims directly back into your primary billing submission software.
We design these connections to talk directly to the systems that hold the source of truth for each workflow. Also, we never make huge, messy copies of your entire hospital database. Instead, the AI looks up the exact data point it needs in real time. Once these bridges are open, you must lock down the system for patient privacy.
8. Secure the System for Patient Privacy
Healthcare software must follow strict federal laws regarding private health information. You must build electronic walls around your database to encrypt patient records and log every single time a user opens a file.
Your security engineers will implement these compliance features:
- Scramble all data using high-grade math codes while it sits in your database.
- Limit data access so employees can only see the records needed for their jobs.
- Keep an unchangeable log that tracks every single view, edit, or file export.
- Strip out names and personal numbers from data used to train the machine.
We build safety controls into your database pipelines and user screens from day one. This deep security ensures your hospital stays completely safe during federal audits. Finally, you need a plan to keep the software running accurately over time.
9. Set Up Long-Term Software Maintenance
Insurance companies change their billing guidelines and rejection codes constantly. Because of this shifting landscape, an AI model that is highly accurate today will slowly lose its effectiveness over time unless it is constantly monitored and updated.
Your technology team will use these maintenance systems:
- Create a simple dashboard to monitor the software’s accuracy in real time.
- Set up alerts to warn you if a model’s accuracy drops after a payer updates their rules.
- Save the exact reasons why your staff skips an alert to improve future training.
- Build a quick reset button to safely restore an older software version if an update fails.
We treat revenue AI as a continuously monitored production system, never a one-time code release. This ongoing care ensures your platform adapts automatically as insurance companies adjust their tactics. Now that you know how the system is built, let’s look at the actual costs involved in funding a project like this.
Healthcare Revenue Optimization Software Development Cost
Healthcare revenue optimization software development cost usually ranges from $60,000 to $220,000 for a focused MVP. That budget can support one measurable recovery workflow, such as payer underpayment detection or charge capture gap analysis, with secure integrations and review controls.
A multi-facility platform with broader contract intelligence, several EHR connections, and mature MLOps requires later expansion phases.
For many hospital systems, that may be payer underpayment recovery based on claim-line data, contract terms, and ERA 835 payment evidence.
1. Cost Breakdown for a Focused AI Revenue Optimization MVP
| Development Phase | Estimated Cost | What It Covers |
| Product discovery and revenue leakage audit | $5,000–$12,000 | KPI baselines, payer mix review, leakage category mapping, MVP workflow selection |
| Data readiness and architecture planning | $8,000–$20,000 | EHR, claims, remittance, contract, ERP, and clearinghouse data assessment |
| Revenue workflow UX and dashboards | $5,000–$15,000 | CFO dashboards, recovery queues, reviewer screens, payer views, action tracking |
| Data ingestion and normalization layer | $12,000–$40,000 | FHIR R4, HL7, EDI 837/835, payer feeds, contract data, field normalization |
| Initial contract intelligence and AI model | $15,000–$55,000 | Allowed amount verification, leakage detection, variance scoring, recovery prioritization |
| Compliance, testing, and deployment | $10,000–$35,000 | HIPAA controls, access rules, audit logs, QA, UAT, model validation, production release |
| MLOps and monitoring setup | $5,000–$43,000 | Model tracking, drift monitoring, feedback capture, performance dashboards, update workflow |
| Focused MVP Total | $60,000–$220,000 | One recoverable revenue workflow with production controls and measurable KPI tracking |
Planning an AI Revenue Optimization Software Budget?
Contact Intellivon’s experts to figure out your Revenue Optimization Build Roadmap to estimate MVP scope, AI model requirements, payer contract intelligence needs, integration complexity, compliance controls, timeline, and development cost before committing to a build.
Enterprise Expansion Costs After the MVP
Once the first workflow proves recoverable value, healthcare systems can expand the platform in controlled phases rather than overbuilding from day one.
| Expansion Module | Additional Estimated Cost | What It Adds |
| Multi-payer contract intelligence expansion | $35,000–$90,000 | More contract types, fee schedules, carve-outs, allowed amount logic, payer comparisons |
| Additional EHR, PM, or facility integrations | $20,000–$70,000 per integration group | New source mappings, validation, user workflows, deployment testing |
| Advanced revenue forecasting and payer analytics | $40,000–$120,000 | Revenue trend analysis, payer behavior models, service-line benchmarking |
| Enterprise MLOps and model governance | $25,000–$75,000 | Drift monitoring, model registry, validation workflows, approval controls |
| Commercial SaaS architecture | $35,000–$100,000 | Tenant management, configurable workflows, onboarding, client reporting |
Ongoing Maintenance Cost
Healthcare organizations should plan for 18% to 28% of the initial build cost per year for ongoing maintenance. For a $60,000 MVP, that means roughly $10,800 to $16,800 annually. For a $220,000 MVP, it means roughly $39,600 to $61,600 annually.
Data Integration (What the Platform Must Ingest to Function)
AI revenue optimization software requires data from five source categories to function: clinical documentation, billing transactions, payer contracts, prior authorizations, and population health files.
Each source requires a separate ingestion pipeline and a data quality gate before it feeds any ML model. Consequently, your platform must connect directly to these pipelines to establish an accurate financial picture.
1. Ingesting Clinical Records via EHR Bridges
Your software must read clinical data straight from your electronic health records (EHR) to catch missed charges and coding errors.
- Using Modern Standards: The platform connects to tools like Epic or Cerner using secure FHIR R4 APIs to extract patient demographics, encounter lengths, and procedure history.
- The Text Reading Challenge: For deep analysis, like finding missed chronic condition codes, the system needs raw doctor notes.
- Access Requirements: This text data is pulled using specialized documentation links. However, hospital networks often need to sign extra access agreements with their EHR vendors to unlock these text pipelines.
2. Processing Insurance Receipts in Real Time
To stop underpayments before they damage your cash flow, the software must monitor transaction files the exact second they arrive from your clearinghouse.
- Reading Digital Receipts: The ingestion pipeline constantly reads electronic payment receipts, which are standard digital text files detailing what the insurance company paid.
- Line-Item Checks: The tool parses every single line item, checking the exact dollar amounts and adjustment reason codes.
- Speed Matters: This processing must happen live, not in slow nightly batches. Catching an underpayment the moment it is posted allows your billing team to flag the variance before the account is mistakenly closed out as “paid in full.”
3. Managing Multi-EHR Databases After Mergers
Hospital networks that grow by buying out smaller local clinics usually inherit a messy mix of different software systems.
- The Blueprint Issue: If your network runs Epic in your main hospital but uses Meditech or athenahealth at your rural clinics, your AI cannot read the data.
- The Solution Layer: You must build an integration translation layer that reformats different software records into one matching style.
- The Financial Realities: Adding this translation database increases complexity, adding $30,000 to $80,000 to your software development costs for every additional EHR system you connect.
For a deeper look at EHR integration architecture, see our guide on Building Smart EHR Systems with AI Capabilities.
4. Verifying Prior Approvals and Population Health Data
The final ingestion layers feed your preventive models, making sure you have permission to bill for high-cost care before it happens.
- Tracking Permissions: The platform pulls data from prior authorization databases and insurance portals to match treatment approvals with final claims.
- Value-Based Care Data: For specialized value-based care contracts, the system tracks population health registries to monitor patient risk scores.
- The Data Gatekeeper: Every single piece of incoming data passes through an automated cleanliness gate that filters out corrupt text and duplicate files before they reach your AI models.
Data integration is a permanent architecture layer. Health systems that underestimate the complexity of their data environment (multiple EHRs, legacy clearinghouse connections, fragmented payer contract storage) consistently underestimate build timelines and cost by 25% to 40%.
ROI Metrics for AI Revenue Cycle Optimization Software Build Decisions
AI revenue cycle optimization software build decisions should be based on measurable revenue outcomes, not automation volume.
The strongest ROI metrics include underpayment recovery, net collection rate improvement, denial rate reduction, first-pass acceptance rate, days in AR reduction, cost to collect reduction, write-off reduction, and recovered dollars per reviewer hour.
1. Tracking the Numbers That Matter
To justify building custom software, you must tie the platform’s performance directly to your bottom line. Finding mistakes is useless if your team cannot turn those warnings into real cash.
Therefore, your business case should focus on actual recovered dollars rather than the total volume of files scanned by the machine.
The table below shows a standard ROI model for a health system after launching a custom platform:
| ROI Metric | Baseline | Target After MVP | Why It Matters |
| Underpayment Recovery Rate | 0.5% of net revenue | 1.0% to 2.5% | Direct revenue recovery |
| Denial Rate | 10% | 7% to 8% | Reduces rework and lost cash |
| Clean Claim Rate | 87% | 92% to 95% | Improves first-pass acceptance |
| Days in AR | 48 days | 40 to 43 days | Speeds cash flow |
| Cost to Collect | 3.5% | 2.8% to 3.1% | Improves operating efficiency |
| Write-Off Rate | Current baseline | 10% to 20% reduction | Protects earned revenue |
2. Recovery Value Should Beat Detection Volume
Generating thousands of automated software alerts actually hurts your business if they overwhelm your billing team. For example, 10,000 low-value alerts are far worse than 500 high-value, fully resolvable errors.
Because your staff has limited hours, the platform must sort and rank its findings automatically:
- True Cash Value: Sort alerts by the exact dollar amount you can legally recover.
- Payer History: Score the probability that a specific insurance company will actually pay the claim based on past cases.
- Filing Timers: Prioritize claims that are close to their hard federal or contractual appeal deadlines.
- Staff Capacity: Match the daily alert volume to the actual number of available reviewers on your team.
This automated filtering keeps your staff focused on high-value wins that move your financial metrics quickly.
2. Dashboards Need Explainable Financial Evidence
Hospital finance leaders will not trust an AI alert that simply says “payment error” without showing its work. To make a real impact, your executive dashboard must present clear, audit-ready proof for every single discrepancy.
Every item in your review queue needs to display these specific facts on a single screen:
- Source Document: A direct digital link to the original medical bill and the insurance receipt.
- Contract Rule: The exact page and paragraph of the insurance contract that dictates the price.
- The Payment Gap: Clear math showing the expected payment, the actual payment, and the final variance amount.
- Confidence Rating: A percentage score showing how sure the AI is that a mistake actually happened.
- Next Steps: A single button to automatically generate an appeal letter or route the file to a specialist.
ROI should define the product roadmap. This is because when metrics shape the architecture, the platform stays focused on revenue outcomes instead of empty AI features. Therefore, the final section highlights how choosing the right partner ensures your system is built to deliver these exact financial returns.
Build AI Revenue Optimization Software With Intellivon
Intellivon helps healthcare systems, RCM companies, and digital health product teams build AI revenue optimization software that identifies revenue worth recovering and proves why it is recoverable.
The platform we build connects payer contracts, claims, ERA 835 remittance data, clinical evidence, reviewer workflows, and finance KPIs into a reimbursement truth layer built for real payment decisions.
A. Start With the Revenue Leak Worth Automating
A revenue optimization platform should not begin with every possible billing gap. Intellivon helps teams identify the first workflow where AI can support measurable cash recovery, strong evidence, manageable review effort, and controlled compliance exposure.
- Prioritize payer underpayments, charge capture gaps, denial leakage, or write-off recovery.
- Compare suspected leakage with evidence-backed recoverable revenue.
- Score opportunities by cash value, repeatability, effort, and compliance risk.
- Define the MVP around one measurable financial outcome.
B. Build a Reimbursement Truth Layer
Revenue teams need more than an alert that a payment looks low. Intellivon builds systems that connect the submitted claim, expected reimbursement, payer contract rule, and reviewer action in one auditable workflow.
- Ingest claims, contracts, fee schedules, and ERA 835 files.
- Validate allowed amounts against payer-specific payment logic.
- Identify recurring contract variance across payers and service lines.
- Route evidence-backed recovery opportunities to the right teams.
C. Make AI Recommendations Defensible
AI should help revenue teams recover valid payments without creating unsupported billing actions. Intellivon designs model outputs around explanation and audit visibility so finance and compliance teams can trust every recommended action.
- Score underpayment and leakage opportunities by recovery probability.
- Show the evidence behind each AI recommendation.
- Flag coding, documentation, or overpayment risks for review.
- Maintain human approval before financial action is taken.
D. Connect Recovery Intelligence to Daily Operations
A useful platform must fit into the systems and queues that revenue teams already use. Intellivon connects reimbursement intelligence with EHR, practice management, and finance environments so findings can move from detection to action.
- Integrate FHIR R4, HL7, EDI 837/835, payer, and finance data.
- Create work queues for revenue integrity, billing, contracting, and compliance teams.
- Track disputes, appeals, corrections, recoveries, and protected revenue.
- Monitor payer patterns across facilities, specialties, and service lines.
C. Measure Recovered Cash, Not AI Activity
Intellivon structures the platform around finance outcomes rather than model volume. Success is measured by validated leakage, recovered payment, recovery time, reviewer effort, protected revenue, payer performance, and revenue cycle KPI improvement.
- Track detected, validated, recovered, and protected revenue separately.
- Measure payment recovery by payer, facility, and leakage category.
- Monitor net collection rate, days in AR, and write-off reduction.
- Expand only after the first workflow proves measurable value.
If you are planning to build AI revenue optimization software for a hospital network, RCM company, or healthcare SaaS platform, Intellivon can help you define the first recoverable revenue workflow, design the reimbursement intelligence layer, and build a compliant production roadmap around measurable financial results.
Conclusion
Building custom financial software allows your healthcare network to plug costly billing leaks and secure your hard-earned revenue. By targeting real underpayments and organizing messy insurance data, this system shifts your financial team from reactive tracking to strategic market leverage.
Ultimately, owning your own artificial intelligence infrastructure protects your operating margins, helps ensure long-term compliance, and delivers predictable, cash-backed returns straight to your bottom line.
Things To Know About AI Revenue Optimization Software
Q1. How much does AI revenue optimization software cost to build?
A1. AI revenue optimization software usually costs $50,000 to $220,000+ to build. That being said, a focused MVP for underpayment detection or payer contract variance may cost $70,000. Additionally, a multi-facility enterprise platform with EHR integration, contract intelligence, MLOps, and HIPAA controls can exceed $220,000.
Q2. How long does it take to build AI revenue optimization software that healthcare teams can use?
A2. A focused MVP usually takes 6–9 months, while an enterprise platform takes 12–18 months. However, the timeline depends on EHR access, payer contract quality, claims history, remittance data, AI model depth, security review, and workflow complexity. Data readiness often drives the schedule more than coding.
Q3. Can AI revenue leakage detection software recover underpayments automatically?
A3. AI revenue leakage detection software can detect and prioritize underpayments automatically, but recovery should include human review. However, the system should compare expected payment with actual payment, show contract evidence, calculate variance, score recovery probability, and route cases to billing or payer contracting teams for action.
Q4. Is custom AI revenue optimization healthcare software better than buying an RCM tool?
A4. Custom AI revenue optimization healthcare software is better when payer contracts, facility workflows, leakage categories, and integration needs are too specific for standard tools. Buying works for claim scrubbing or basic denial queues. Building works when you need proprietary payer intelligence, underpayment recovery, and multi-facility revenue visibility.