

Key Takeaways:
- Agentic AI executes multi-step billing workflows across eligibility, coding, claims, denials, and payment posting.
- Multi-agent orchestration, FHIR R4 APIs, RAG pipelines, and EDI 837/835 automation are core requirements.
- Confidence thresholds, audit trails, HIPAA controls, and human-in-the-loop review ensure production-grade governance.
- Custom builds cost $50,000 to $170,000, depending on agent complexity, integrations, and enterprise scale.
- How Intellivon builds agentic AI RCM as governed healthcare infrastructure and not disconnected AI proof-of-concept demos.
Building agentic AI for revenue cycle management requires four components in the right sequence. These include an orchestration layer that defines decision boundaries, a clinical AI model fine-tuned on RCM workflows, an EHR integration framework, and a human-in-the-loop review layer. Without this sequence, you get an autonomous system that either stalls at every decision point or runs without the audit control that healthcare compliance requires.
The piece that determines whether agentic RCM works in production is the orchestration layer, specifically, the decision boundaries that define what the agent executes autonomously and what it routes for human review. Without these boundaries, compliance teams shut the system down or restrict it until it performs no better than a rules engine. When built correctly, agentic systems can automatically rework the 65% of denied claims that billing teams currently write off without ever reviewing.
Intellivon has spent over 10 years building agentic AI systems for healthcare workflows with orchestration-first architecture, the design pattern that keeps agents compliant, auditable, and useful in production. This blog covers agent architecture, decision boundary design, EHR integration specs, HIPAA controls, and real development cost ranges, so you can make an informed decision on this build.

What Is Agentic AI for Revenue Cycle Management?
Agentic AI for revenue cycle management is a software architecture where specialized AI agents autonomously plan, execute multi-step workflows, call APIs, and manage exceptions across the billing lifecycle.
Unlike rule-based automation, this system uses goal-directed AI planning to handle complex tasks like clinical document retrieval and denial root cause classification without human intervention at every individual step.
To transform your billing infrastructure from rigid rules to autonomous execution, you must understand how agentic systems operate differently from legacy software.
1. Technology Comparison
The table below establishes how agentic architecture fundamentally changes the RCM technology stack.
| Technology | Operation Model | Core Capability | RCM Limitation |
| RPA | Deterministic scripts | UI click replication | Breaks when payer portals change UI |
| Generative AI | Probabilistic next-token | Document summarization | No execution power or system memory |
| Predictive AI | Statistical matching | Denial risk scoring | Identifies problems but cannot fix them |
| Agentic AI | Goal-directed loops | Tool calling & reasoning | Requires human-in-the-loop for low confidence |
2. Deconstructing the AI Agent
In simple terms, an “agent” is an autonomous software worker built using five core components:
- Goal: A specific objective, such as “resolve this denied claim.”
- Context: The environment data, including the patient’s EHR and the payer’s rules.
- Tools: Action mechanisms like database queries, FHIR R4 APIs, and browser automation.
- Memory: Short-term session tracking and long-term historical billing patterns.
- Decision Policy: Guardrails that dictate when to act and when to escalate.
3. Traditional vs. Agentic RCM Software
Building an agentic AI healthcare billing platform shifts your software from a passive database to an active workforce.
Traditional software requires users to manually open charts and click through screens. Agentic software operates via specialized agents that coordinate tasks independently.
- Eligibility Verification Agent: Uses clearinghouse agent connectors to query insurance databases, parsing response files to confirm active coverage limitations.
- Prior Authorization Agent: Extracts clinical documentation, checks medical necessity rules, and uploads packets to payer portals using a ReAct agent framework.
- Claims Submission Agent: Runs NCCI edit validation and formats data into EDI 837 files for straight-through processing.
- Denial Management Agent: Performs denial root cause classification and queries internal systems for missing data elements.
- Payment Posting Agent: Reconciles electronic remittance advices (EDI 835) against bank deposits, identifying hidden contractual variances.
- Appeal Drafting Agent: Conducts clinical document retrieval to generate custom appeal letters containing specific payer policy citations.
An agentic platform handles the variable logic of healthcare billing natively, eliminating the need for constant script maintenance.
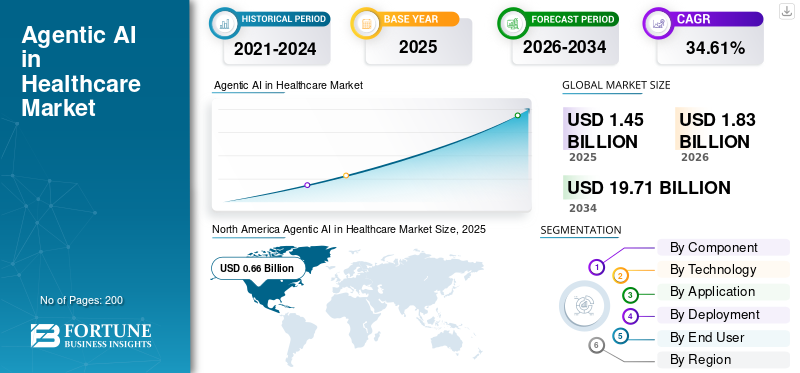
Agentic AI for Revenue Cycle Management (RCM) is the fastest-growing application within the healthcare AI RCM market, with RCM holding the largest market share (20.8% in 2026) in the broader agentic AI healthcare sector.
Agentic RCM is a workflow execution layer that sits between clinical data, payer rules, billing systems, and human reviewers. That makes architecture the real decision, not model choice alone.
Why Health Systems Are Moving Beyond RCM Automation
Health systems are moving beyond rule-based RCM automation because payer workflows now change faster than static rules can keep up. At the same time, revenue teams need systems that can read documents, retrieve payer criteria, call APIs, navigate portals, classify denials, draft appeals, and route exceptions without asking humans to manage every step manually.
1. The Problem With Old Rules
Old-school automation uses rigid “if-then” rules. This approach breaks down because modern billing work is scattered across too many different places.
- Too many portals: A billing worker must log into separate insurance portals, check an EHR, and read long insurance policies just to fix one tiny mistake.
- Brittle bots: Old software bots get confused and stop working the moment a payer changes a button on their website.
- Massive staff shortages: Hospitals do not have enough billing experts to fix these broken automations manually.
- Climbing denial rates: Insurance claim denials have climbed significantly, hovering at an average benchmark above 10% in 2026. In specific settings like ACA marketplaces, data from KFF shows in-network denial rates averaging 19%.
- High operational costs: This surge in manual rework drives up hospital costs. The Healthcare Financial Management Association (HFMA) tracks strategies to mitigate these rising administrative and labor expenses, which traditionally push a hospital’s overall cost-to-collect range between 2% and 4% of total revenue.
Why Autonomous Workflows Matter
This is why an autonomous RCM workflow automation build is so valuable. Instead of doing one small copy-paste job, the AI can handle a whole chain of tasks from start to finish without stopping.
When you switch to an agentic system, your platform tracks success using clear business metrics:
- First-pass resolution rate: The percentage of claims paid on the very first submission.
- Straight-through processing rate: The share of claims handled entirely by AI without a human ever touching them.
- Days in AR reduction: Getting money from insurance companies days or weeks faster to improve cash flow.
- Cost per claim reduction: Dropping the manual labor cost needed to process every bill.
For a deeper breakdown of broader RCM platform planning, see our guide on How to Build an AI Revenue Automation Platform.
The shift is not from humans to machines. The shift is from static queues to governed execution. Once the workflow needs planning, tool use, state tracking, and escalation, the architecture must support agents from the beginning.
RPA vs. Workflow Automation vs Agentic AI: What Should Handle Each RCM Task?
Engineers should not use AI agents for every RCM task because deterministic code is safer and cheaper for predictable billing steps. At the same time, autonomous agents are built for variable tasks that require human-like reasoning, tool usage, and document text comprehension.
The framework below maps typical revenue cycle steps to the correct automation technology.
| RCM Task | Best Automation Type | Why It Fits |
| Eligibility checks | API + workflow automation | Uses structured data and repeatable query logic. |
| Payer portal navigation | RPA + supervised agent | Portals vary frequently and can break rigid UI scripts. |
| Prior auth evidence matching | Agentic AI + RAG | Requires deep document retrieval and medical reasoning. |
| Claim edit validation | Rules engine | Follows simple, deterministic pass or fail logic. |
| Denial classification | ML + agent workflow | Needs multi-layered pattern detection and case context. |
| Appeal drafting | LLM agent + human review | Demands natural language generation and evidence layout. |
| Payment posting | EDI automation + rules | Runs on highly structured remittance file workflows. |
Using this specialized distribution keeps your platform fast, accurate, and cost-effective. This ensures you use high-compute AI models only when structural uncertainty makes standard code impossible to use.
5 Levels of RCM Agent Autonomy
The safest way to build agentic AI for revenue cycle management is to assign every workflow a specific autonomy level before development starts. Some agents can retrieve data or draft text independently, while others can submit transactions only after passing clear confidence checks.
At the same time, high-risk actions, such as changing diagnostic codes or adjusting financial balances, require human approval.
1. Defining the Five Levels of Agent Autonomy
Engineering teams should structure their multi-agent system design around five progressive levels of operational autonomy. This framework controls how much permission an AI agent has within your active electronic health records (EHR) and billing software.
- Level 0 – Observe Only: The agent reads claim data, checks status portals, and observes workflows. It has zero write permissions and is perfect for shadow-mode testing.
- Level 1 – Recommend: The agent identifies issues and suggests solutions, such as highlighting a likely denial reason. A human operator makes the final decision.
- Level 2 – Draft: The agent creates complex text files like appeal letters or prior authorization requests. The system requires a human to review the text before hitting send.
- Level 3 – Execute with Guardrails: The agent handles simple data transactions independently if its internal confidence score passes a preset threshold. If the score falls low, the system triggers an agent fallback routing mechanism to a human queue.
- Level 4 – Autonomous with Exception Routing: The agent runs a complete workflow from start to finish, such as tracking down and reconciling an outstanding claim status. It only alerts humans if a rare, unrecognized error occurs.
- Level 5 – Restricted / Human-Owned: High-risk financial or legal tasks where autonomous AI action is permanently blocked. Humans must execute these tasks to maintain compliance.
2. The RCM Autonomy Layers
The table below maps everyday RCM tasks to their safe, production-ready autonomy levels.
| RCM Workflow | Target Autonomy Level | Core Engineering Justification |
| Eligibility verification | Level 3–4 | High data structure consistency and low clinical compliance risk. |
| Prior authorization assembly | Level 2–3 | Demands complex clinical document retrieval and evidence matching. |
| Prior authorization submission | Level 2–3 | Portal variations require strict human-in-the-loop agent review. |
| ICD-10-CM / CPT coding | Level 1–2 | High audit exposure and severe revenue integrity risk. |
| Claims submission | Level 3 | Safe to automate once deterministic clearinghouse edits pass. |
| Denial root cause classification | Level 2–3 | Excellent for classification, but corrective steps require oversight. |
| Appeal drafting | Level 2 | An appeal drafting agent creates the text, but humans sign off. |
| Payment posting | Level 3–4 | Clear matching patterns when EDI 835 transaction files are clean. |
| Patient balance adjustment | Level 0–1 | Extreme financial sensitivity prevents autonomous edits. |
Building a multi-agent system design with these five clear levels keeps your hospital records completely safe. It stops the software from accidentally changing or erasing important billing information by mistake.
By keeping simple tasks separate from high-risk money changes, you make sure your AI tools stay helpful and never cause costly legal mistakes.
Agentic AI Architecture for a Multi-Agent RCM System
Agentic AI architecture for RCM should separate workflow orchestration, agent reasoning, tool access, data retrieval, rules validation, human review, and audit logging.
A safe multi-agent RCM system does not let one general agent run the revenue cycle. At the same time, it uses specialized agents with scoped permissions and monitored execution paths.
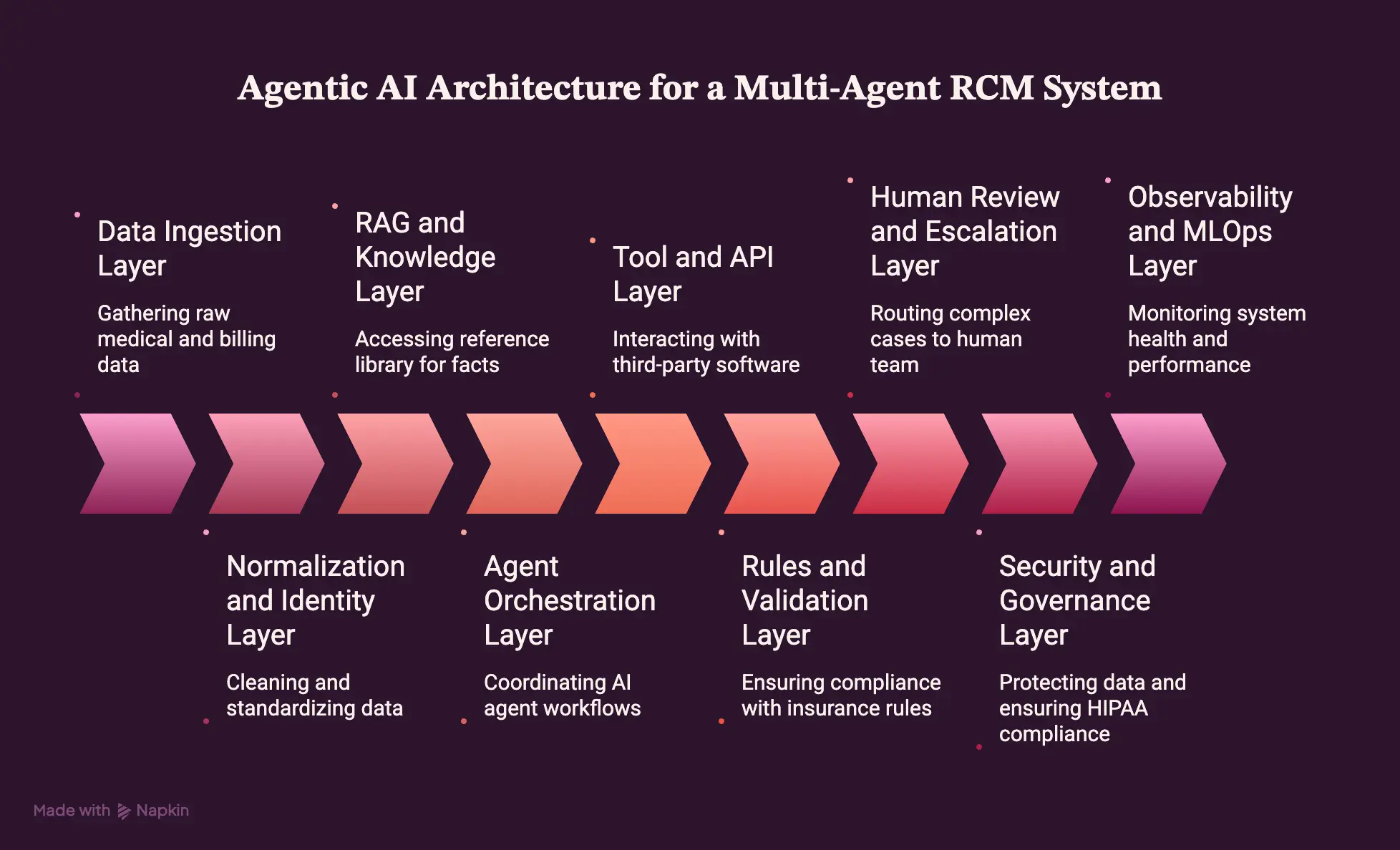
1. Data Ingestion Layer
This initial layer pulls in all the raw medical and billing data from your software systems. It gathers patient records from the EHR, financial logs from practice management data, and historical claims history.
The software also reads electronic remittance files, incoming payer responses, and unstructured text like clinical documentation, call notes, and scanned PDFs. Gathering this information into one spot ensures your agents have the raw facts they need to evaluate a bill.
2. Normalization and Identity Layer
This block cleans up the data so the AI does not get confused by different naming styles. It runs patient matching and encounter linking to make sure every doctor visit connects to the right person.
[Raw Billing Files] ──> [Normalization Layer] ──> [Clean, Unified Data Profiles]
The system maps unique claim IDs, provider locations, and varying payer plans into standard labels. Normalizing these terms prevents errors caused by mismatched insurance names or typos across hospital systems.
3. RAG and Knowledge Layer
This section acts as the platform’s reference library, using a RAG pipeline for RCM to look up facts on demand. It performs automated clinical document retrieval to pull the exact charts needed for a specific insurance claim.
- Payer policy retrieval: Finds the latest coverage rules from insurance websites.
- Medical necessity criteria: Checks if a treatment matches standard medical guidelines.
- Contract terms: Confirms the exact dollar amounts the insurance company agreed to pay.
- NCCI edits references: Cross-references federal coding rules to spot banned code pairs.
- Internal SOPs: Keep track of your own billing team’s custom work habits.
4. Agent Orchestration Layer
This layer serves as the main brain that coordinates the AI agent orchestration process. It uses LangGraph agent workflows to build clear, reliable paths for data to follow.
Using a ReAct agent framework, individual agents can think and act in a loop, breaking down massive billing problems through agent task decomposition. This goal-directed AI planning allows the software to manage its own progress via strict agent state management, tracking what has been fixed and what to do next.
5. Tool and API Layer
This layer gives your agents a hand to interact with third-party software platforms. It handles EHR workflow agent integration through standard FHIR R4 API links and custom payer API integrations.
[AI Agent Brain] ──> [Function Calling Engine] ──> [Triggers EHR API or Portal Click]
The system uses clearinghouse agent connectors to send bills, runs EDI 837 / EDI 835 automation to read payments, and deploys a payer portal navigation agent to log into insurance websites. By using native function calling in LLMs, the system turns text thoughts into instant tool calling and API integration commands.
6. Rules and Validation Layer
This block acts as a digital safety guard that double-checks all AI decisions against hard laws. It runs a deterministic payer rules engine integration to make sure bills match insurance contracts perfectly.
The platform runs strict NCCI edit validation and uses a medical necessity checking agent to verify clinical details. It screens every claim edit check and coverage rule to confirm that all CPT and ICD-10-CM constraints are met before any file leaves the system.
7. Human Review and Escalation Layer
This layer protects your revenue by routing difficult or confusing cases to your human team. It enforces a human-in-the-loop agent review system based on strict agent confidence thresholds.
[Low AI Confidence Score] ──> [Agent Fallback Routing] ──> [Human Reviewer Queue]
If an agent is unsure how to fix a denial, it triggers agent fallback routing to push the record into dedicated reviewer queues. Human billers can see the issue on custom approval screens, read the AI’s exception notes, and make manual corrections easily.
8. Security and Governance Layer
This layer keeps your data safe and ensures you deploy completely HIPAA-compliant AI agents. It uses PHI de-identification and PHI tokenization to scramble private patient data before it touches any AI models.
- Private model hosting: Keeps all health data inside your own secure cloud walls.
- Zero-trust architecture: Mandates that every software piece verifies its identity constantly.
- BAA compliance: Fulfills federal legal contracts required for handling healthcare records.
- Agent prompt injection controls: Blocks malicious text inputs from confusing the AI’s programming.
- LLM guardrails in healthcare: Sets hard boundaries so the AI never makes up facts or outputs weird answers.
9. Observability and MLOps Layer
This final layer monitors the health and speed of your active AI system using specialized MLOps for agentic AI. It runs continuous model drift monitoring to check if changing insurance patterns are lowering your AI’s accuracy over time.
The software runs agent performance benchmarking and agent regression testing inside a safe, isolated agent regression testing landscape. Every single decision is saved in a secure agent audit trail, providing clear, explainable agent decisions so human managers can audit exactly why an agent chose a specific billing action.
[For a deeper breakdown of the underlying data structures and risk modules, see our guide on AI Claims Scrubbing Software Development for Healthcare.]
The architecture should make agents powerful only where the workflow can prove correctness. Therefore, the system needs deterministic checks around probabilistic reasoning. The next section should show how to assign specific agents to the revenue cycle.
Core AI Agents for Revenue Cycle Automation Workflows
A production agentic RCM platform should use specialized agents for each major revenue workflow instead of one broad agent. The best starting set includes eligibility, prior authorization, coding support, claims validation, denial management, appeals, payment posting, and revenue intelligence agents, each with defined tools, permissions, confidence rules, and escalation paths.
RCM Agent Comparison
The table below breaks down what each helper agent does, how much freedom it has to work alone, and when it must stop and ask a human for help.
| Helper Agent | What It Does | Freedom Level | When It Stops For Humans |
| Eligibility Verification | Checks insurance coverage and copays | High | If insurance data is missing or confusing |
| Prior Authorization | Gathers doctors’ notes for approval | Medium | Always requires a final human check before sending |
| Coding Support | Suggests medical billing codes | Low | Gives choices; humans must pick the final code |
| Claims Submission | Double-checks and sends out the bills | High | If a bill has errors that violate payer rules |
| Denial Management | Finds out why a bill was rejected | Medium | If the reason for rejection is completely new |
| Appeal Drafting | Writes letters to fight rejected bills | Low | Write the letter, but a human must sign it |
| Payment Posting | Matches bank deposits to open bills | High | If the money received does not match the bill |
Once your workflow agents are up and running, you can connect them to your master dashboard to watch your processing speeds climb.
This transition transforms your billing setup from an expensive pile of messy data into a clean, smooth, and highly automated cash flow machine.
HIPAA, PHI, and Security Controls for Healthcare AI Agents
HIPAA-compliant AI agents need access controls, audit controls, transmission security, PHI minimization, encryption, role-based permissions, private inference controls, and vendor agreements before production use. Agentic systems need stricter safeguards because agents can retrieve data, call tools, write outputs, and trigger actions across multiple healthcare systems.
1. Protecting Patient Data
Keeping patient data safe means locking down how information flows through your system. So, you cannot let raw medical records float around freely.
- PHI tokenization: Scrambles private names and numbers into safe codes before they touch any AI models.
- Private model hosting: Keeps your AI brain running inside your own secure cloud walls so data never leaks to outsiders.
- Data minimization: Gives the agent only the exact snippet of text it needs to fix a specific bill, nothing more.
2. Controlling Agent Actions
You must set strict boundaries on who can look at files and what tools your software is allowed to use.
- Tool allowlists: A hard list of approved websites and APIs the AI is allowed to visit.
- Agent prompt injection controls: Specialized blocks that stop bad text inputs from hijacking your software’s instructions.
- Kill-switch triggers: Instant shut-off buttons that stop an agent the moment it behaves oddly or tries to access unapproved files.
[Secure EHR Data] ──> [Tokenization Gate] ──> [Safe AI Processing] ──> [Human Guardrail]
3. Staying Legal and Compliant
Every single step your software takes must leave a clear paper trail for legal audits.
- BAA compliance: Signed legal agreements that prove your tech setup follows all federal healthcare laws.
- Agent audit trail: A permanent, unchangeable digital logbook that records every file the AI reads and every tool it clicks.
- Action approval gates: Safety checkpoints where the AI must stop and wait for a human signature before making big financial changes.
Security for agentic RCM is not only about protecting stored data. It is about controlling what each agent can see, decide, and do. That is why governance must sit inside runtime architecture, not outside it.
How to Build Agentic AI for Revenue Cycle Management
To build agentic AI for revenue cycle management, start with workflow scope, then define agents, data access, tool permissions, human review, compliance controls, model strategy, integration design, testing, and ROI tracking.
The safest roadmap starts with low-risk workflows before expanding into coding, prior authorization, appeals, and claims automation.
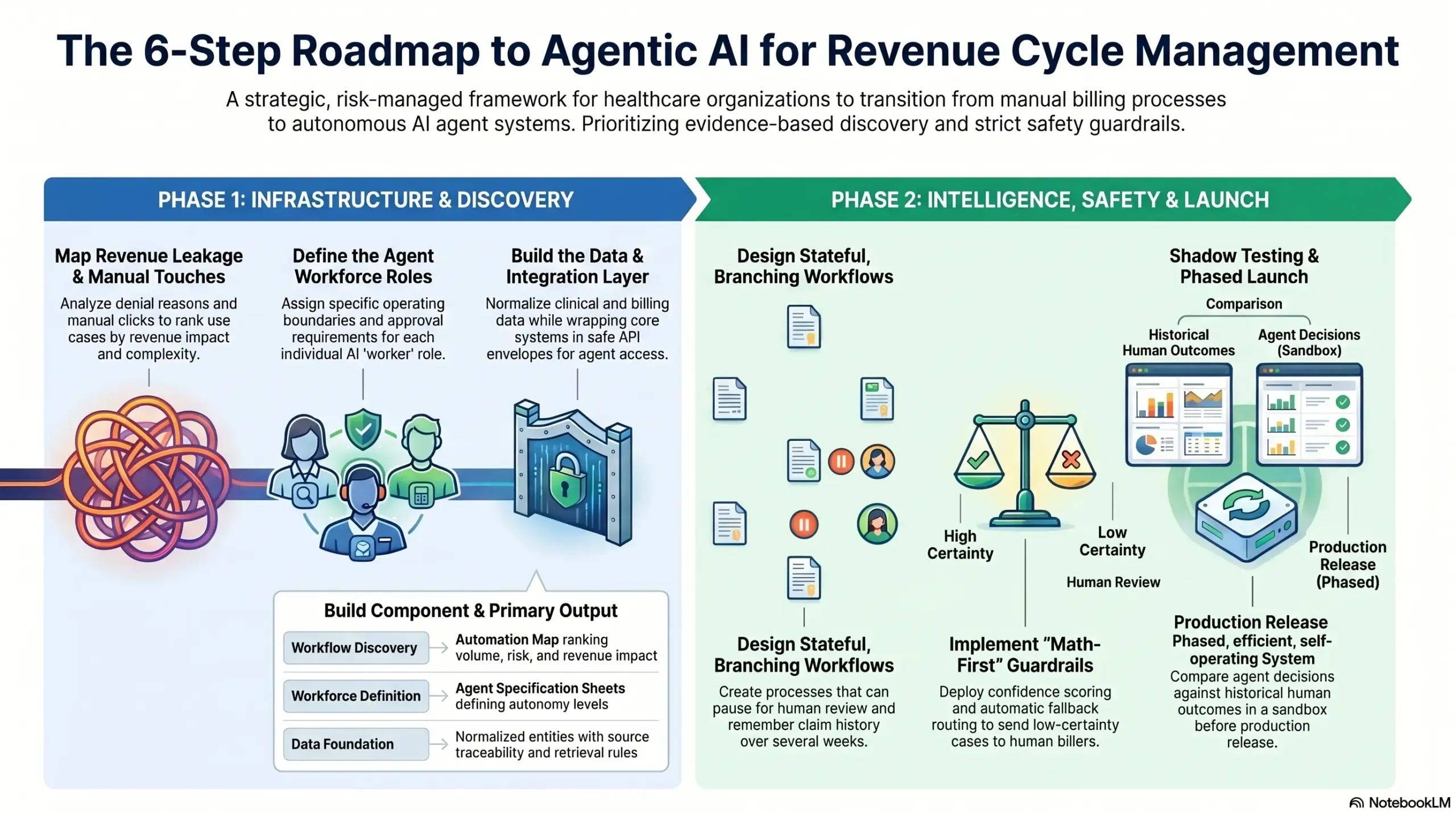
Step 1 — Map RCM Workflows and Revenue Leakage
Start by mapping where revenue work gets delayed, denied, underpaid, or manually touched too often. At the same time, agentic AI should not begin with model selection. It should begin with workflow evidence, including denial reasons, payer delays, manual task volume, claim aging, staff effort, and recovery potential.
- Deep Claim Audits: We trace your bills from creation to final payment to locate hidden cash leaks.
- Manual Touch Tracking: Our team counts exactly how many times your staff clicks inside a record to fix repetitive errors.
- Payer Behavior Review: We analyze historical insurance data to map which companies deny claims most frequently.
- Intellivon Approach: We run workflow discovery with billing, coding, IT, compliance, and finance teams. The output should be an automation map that ranks use cases by volume, risk, revenue impact, and integration complexity.
After the workflow map is clear, the next step is deciding which agents should exist.
Step 2 — Define the Agent Workforce and Autonomy Levels
Define each agent by job, tools, data access, confidence threshold, fallback route, and approval requirement. At the same time, a multi-agent RCM system development project becomes risky when agents are vaguely scoped. Each agent needs a clear operating boundary before engineering begins.
- Custom Agent Catalogs: We design specific software worker roles so no single AI tries to manage everything.
- Task Decomposition Frameworks: We configure our systems to break massive problems like insurance disputes into small, bite-sized tasks.
- Permission Mapping: Our builders assign strict read and write boundaries to every single AI helper tool.
- Intellivon Approach: We create an agent specification sheet for every workflow. This keeps scope disciplined and helps stakeholders understand what the system will automate, assist, draft, or block.
Once roles are defined, the platform needs a data infrastructure that agents can trust.
Step 3 — Build the Data and Knowledge Foundation
Build the data foundation by connecting clinical, billing, payer, claims, remittance, and document sources into a normalized RCM layer. Additionally, agents need a complete case context before acting. And without clean patient, encounter, claim, payer, and document linkage, autonomous workflows will create noise instead of throughput.
- Context Linking: We connect separate insurance files, doctor notes, and bank receipts into unified data profiles.
- Policy Ingestion Engine: Our platforms use a RAG pipeline for RCM to read, index, and query thousands of pages of changing insurance rules.
- Clean Record Routing: We ensure your files match up cleanly so the AI never misreads a patient’s medical history.
- Intellivon Approach: We prioritize data reliability before model development. The team would create normalized entities, source traceability, and retrieval rules so every agent action can point back to evidence.
With trusted data in place, agents can safely call tools and APIs.
Step 4 — Design Tool Calling and System Integrations
Design tool calling so agents can retrieve records, validate claim fields, check eligibility, query payer requirements, create drafts, and update workflow status through controlled backend functions. This model should not directly manipulate production systems. Your application should validate every tool call before execution.
- Safe API Wrappers: We wrap core EHR and clearinghouse systems inside protected data envelopes.
- Function Validation: Our engineers force the system to double-check every single command before it clicks an insurance website.
- Failure Catching: We program smart timeout and retry rules so a slow internet link does not crash your automated system.
- Intellivon Approach: We place a secure tool gateway between agents and production systems. This lets agents act through approved functions while preserving auditability, access control, and rollback options.
After tool access is defined, the team can build agent workflows around real RCM states.
Step 5 — Build Agent Workflows With State, Memory, and Review
Build agent workflows as stateful processes that can pause, retry, escalate, and resume. RCM cases rarely move in a straight line. Additionally, a prior authorization may wait for documents, a denial may need appeal evidence, and a claim may need correction before resubmission.
- Branching Workflows: We build LangGraph agent workflows that let the AI take multiple separate paths based on changing data.
- Persistent State Management: Our platforms remember what happened weeks ago on a claim so it never repeats a step.
- Human Hand-off Queues: We build smart pause checkpoints where the AI halts and waits patiently for a human review.
- Intellivon Approach: We use graph-based design for workflows with branching and review. This helps teams replay agent decisions, identify bottlenecks, and prove that human approval occurred where required.
Once workflows operate, the platform needs rules and guardrails that prevent unsafe autonomy.
Step 6 — Add Rules, Guardrails, and Confidence Thresholds
Add guardrails before agents can execute revenue actions. Guardrails should combine payer rules, coding edits, documentation checks, confidence thresholds, prompt injection controls, PHI limits, and human approval gates. This layer keeps agentic automation safe when model outputs are uncertain or incomplete.
- Math-First Rule Engines: We run strict code checks to stop bad or weird formatting from leaving your network.
- Confidence Scoring: Our systems rank every AI thought with a strict grade percentage.
- Automatic Fallback Routing: If a score drops below your set benchmark, the file skips instantly to a human biller’s desk.
- Intellivon Approach: We define pass, review, and block conditions for every agent action. The system should not “trust” an agent because it sounds confident. It should trust only validated outputs.
Guardrails protect decisions, but testing proves whether agents can perform in production-like conditions.
Step 7 — Test Agents in Sandbox and Shadow Mode
Test agents in sandbox and shadow mode before production release. The agent should process real historical cases without changing live workflows. This lets teams compare agent recommendations against human decisions, payer outcomes, denial rates, appeal results, and payment data before granting execution permissions.
- Historical Data Replays: We feed thousands of past claims through the AI to check its choices against real historical outcomes.
- Accuracy Benchmarking: Our teams calculate exactly how often the AI matches a human expert’s work.
- Hallucination Scans: We screen the system to catch and fix any instances where the model makes up false medical text.
- Intellivon Approach: We benchmark agent performance against baseline RCM outcomes. The team would measure where the agent improves throughput and where it needs stricter rules, more data, or lower autonomy.
After sandbox testing, launch should happen in phases, not across the full revenue cycle at once.
Step 8 — Launch, Monitor, and Improve Agent Performance
Launch agentic RCM in phases using monitored production workflows, clear KPIs, reviewer feedback, and rollback plans. This goal is a learning operating layer that improves straight-through processing, denial prevention, appeal quality, and revenue recovery without losing control.
- Live Drift Monitoring: We use advanced MLOps for agentic AI setups to watch the system and ensure accuracy stays high.
- Human Feedback Loops: We build simple like and dislike tools so your human billers can train the AI while they work.
- Dashboard Tracking: Our teams install real-time dashboards to watch your cost per claim drop day by day.
- Intellivon Approach: We treat post-launch monitoring as part of the build, not a maintenance afterthought. Agent actions, reviewer edits, payer outcomes, and revenue KPIs should continuously improve the workflow.
After the build roadmap, readers need a realistic cost range before they commit.
Agentic AI RCM Platform Development Cost
Agentic AI RCM platform development cost usually ranges from $60,000 to $230,000, depending on workflow scope, number of AI agents, EHR integration depth, payer connectivity, model complexity, HIPAA controls, and whether you are building a focused MVP or a controlled multi-agent RCM workflow platform.
A lower-cost build usually focuses on one or two workflows, such as eligibility verification, denial triage, claim status checks, or appeal drafting. A higher-cost build includes multiple agents, deeper EHR and clearinghouse integrations, RAG-based document retrieval, tool calling, human review workflows, and production monitoring.
Cost Breakdown by Development Phase
| Development Phase | Estimated Cost | What It Covers |
| RCM workflow discovery and automation scope | $5,000–$12,000 | Workflow mapping, denial analysis, payer mix review, automation scoring, KPI baseline |
| Agent strategy and autonomy design | $6,000–$18,000 | Agent catalog, autonomy levels, permission matrix, human review rules, escalation paths |
| UX/UI for agent worklists and reviewer screens | $8,000–$22,000 | Agent dashboard, exception queues, reviewer approval screens, audit views |
| Data ingestion and normalization layer | $10,000–$35,000 | EHR, claims, remittance, payer, document, and billing data pipelines |
| RAG and clinical document retrieval layer | $8,000–$28,000 | Vector database, payer policy retrieval, clinical evidence search, SOP indexing |
| Agent orchestration and workflow engine | $12,000–$38,000 | LangGraph workflows, agent states, retry paths, fallback routing, human review checkpoints |
| Tool calling and API integration layer | $10,000–$40,000 | EHR APIs, payer APIs, clearinghouse connectors, EDI workflows, portal automation |
| AI model development and evaluation | $12,000–$45,000 | Clinical NLP, classification, LLM workflows, denial scoring, structured outputs |
| Rules engine and validation controls | $8,000–$28,000 | Payer rules, NCCI edits, medical necessity checks, confidence thresholds |
| HIPAA security and compliance controls | $8,000–$30,000 | RBAC, audit logs, encryption, PHI controls, BAA support, zero-trust setup |
| Testing, sandbox, and shadow deployment | $8,000–$28,000 | Historical replay, regression testing, reviewer comparison, safety testing |
| Production deployment and monitoring | $7,000–$25,000 | MLOps, drift monitoring, KPI dashboards, alerts, and launch support |
Total Cost Bands
| Build Type | Estimated Cost | Best Fit |
| Focused agentic RCM MVP | $60,000–$95,000 | One workflow, such as eligibility verification, claim status checks, or denial triage |
| Controlled two-agent RCM platform | $95,000–$150,000 | Two connected workflows, such as eligibility plus prior authorization support |
| Multi-agent RCM workflow platform | $150,000–$230,000 | Three to four agents across claims, denials, appeals, and payment follow-up |
Ongoing Maintenance Cost
Ongoing maintenance usually costs 15%–25% of the initial build per year. This covers payer rule updates, model monitoring, integration maintenance, security patches, agent regression testing, performance tuning, prompt updates, and compliance reviews.
For example, a $100,000 agentic RCM MVP may need $15,000–$25,000 per year for maintenance. A $230,000 multi-agent platform may need $34,500–$57,500 per year, especially if it connects with EHR systems, clearinghouses, payer APIs, and production billing workflows.
Need a practical cost estimate before you scope the build?
Contact Intellivon to map your workflows, integrations, agent roles, compliance controls, and estimated development budget before speaking with vendors.
Agent Permissioning, Identity, and Kill-Switch Design for RCM Agents
Managing multiple autonomous workers creates a unique control problem often called “agent sprawl.” If left unmanaged, independent billing tools can retain background data access long after their tasks are finished.
To prevent this security risk, we construct a central agent identity registry that treats every AI tool like an individual digital employee. We use this framework to lock down system safety through three specific mechanisms:
- Tool-Level Permissions: Each agent receives scoped access keys that only allow it to read or write to the specific database tables needed for its current billing task.
- Credential Expiry: System connection tokens automatically expire and rotate out on a set schedule, stopping hackers from hijacking old active connections.
- PHI-Bounded Memory: The architecture uses strict data minimization rules that instantly erase all temporary patient data from the model’s active session memory the second a task closes.
To protect your daily operations from runaway software loops, we build automated kill-switch rules directly into the core engine. If an agent hits system rate limits, repeats actions, or attempts an unauthorized financial adjustment, a circuit breaker instantly triggers.
This safety switch immediately revokes the agent’s digital ID, freezes its operations, and routes the entire billing case to a human queue while preserving a clean audit trail for your team.
Build Agentic AI for RCM With Intellivon
Intellivon helps healthcare SaaS founders, RCM companies, health systems, and digital health teams build agentic AI for RCM around real revenue workflows.
The work starts with scope, agent architecture, compliance controls, integration planning, model design, human review, MLOps, and revenue KPIs before full development begins.
1. Define the Right Agentic RCM Automation Scope
Intellivon maps eligibility, prior authorization, coding, claims, denials, appeals, payment posting, and A/R workflows to identify where agents should assist, draft, execute, or escalate. This prevents over-automation and helps teams launch with the safest revenue impact first.
- Identify high-volume RCM workflows with clear automation potential.
- Separate low-risk tasks from workflows needing human approval.
- Prioritize eligibility, denials, claims, appeals, or payment follow-up.
- Define where agents recommend, draft, execute, or escalate.
- Align automation scope with revenue KPIs and compliance risk.
2. Design Multi-Agent RCM Architecture
Intellivon designs multi-agent RCM system development around workflow states, tool permissions, data access, fallback routing, and audit visibility. Each agent receives a defined job, approved tools, confidence gates, and human review rules before production execution.
- Build agent workflows around real RCM operating states.
- Define tool access for each agent before deployment.
- Add confidence thresholds for high-risk billing decisions.
- Route exceptions to coders, billers, or revenue teams.
- Maintain audit trails for every agent action and decision.
3. Build Tool-Using AI Agents With Secure Integrations
Intellivon builds tool-using AI agents that connect with EHRs, payer APIs, clearinghouses, EDI workflows, document systems, and finance platforms through controlled backend functions. Agents act through validated tools, not uncontrolled prompts.
- Connect agents with EHR, billing, and claims systems.
- Use tool calling for controlled backend task execution.
- Support EDI 837, EDI 835, and clearinghouse workflows.
- Add payer API and portal automation where required.
- Validate every agent action before production system updates.
4. Make Agentic RCM Secure, Explainable, and Monitorable
Intellivon embeds HIPAA controls, PHI safeguards, audit logs, explainable agent decisions, prompt injection defenses, model monitoring, and reviewer feedback loops into the platform architecture. This helps teams scale agentic workflows without losing operational control.
- Protect PHI with access controls and audit-ready logging.
- Add human review for sensitive claims and appeal workflows.
- Track model drift, agent errors, and reviewer overrides.
- Explain agent decisions with evidence, rules, and source data.
- Monitor revenue KPIs after every workflow goes live.
If you are planning to build AI agent revenue cycle software around eligibility, prior authorization, claims, denials, appeals, or payment posting, Intellivon can help you define the roadmap before development begins.
Conclusion
Agentic AI for revenue cycle management is worth building when your organization needs more than dashboards, rules, or isolated AI recommendations. The real value comes from governed agents that can retrieve evidence, call tools, execute workflow steps, escalate exceptions, and improve revenue operations with every reviewed outcome.
However, the strongest platforms start narrow, define autonomy carefully, and connect agents to secure healthcare data infrastructure. Instead, they combine RAG, function calling, payer rules, EHR integration, EDI workflows, HIPAA controls, and human review into one controlled operating layer.
Things To Know About Agentic AI for Revenue Cycle Management
Q1.How much does it cost to build AI agent revenue cycle software?
A1. Building AI agent revenue cycle software usually costs $70,000 to $230,000 for a custom pilot setup. At the same time, a narrow system with one or two specialized agents falls on the lower end of this range. Therefore, the total pricing scales upward depending on the number of required EHR integrations and active portal automation tools.
Q2. How long does autonomous AI revenue cycle software development take?
A2. Autonomous AI revenue cycle software development usually takes 5 to 8 months for an initial rollout. At the same time, simple eligibility and denial triage tools launch fastest. However, Complex tasks like prior authorization and appeal drafting take longer because they require deeper software connections, stronger rules validation, and custom human review workflows.
Q3. Can agentic AI healthcare billing agents be HIPAA compliant?
A3. Yes, agentic AI healthcare billing agents can be fully HIPAA compliant when built with strict safety boundaries. Therefore, the underlying system must use private cloud hosting, business associate agreements, and permanent audit trails. Furthermore, agents must only look at the absolute minimum data needed to complete an active billing task.
Q4. Should we build or buy an agentic AI RCM platform?
A4. You should build a platform when your specific workflows, insurance payer mix, or custom software requirements demand unique business logic. Conversely, buying works better if you need a quick point solution for a single repeatable task. Ultimately, a custom build ensures you own your software code and avoid expensive monthly licensing fees.
Q5. Can an AI agent submit claims or appeals without human review?
A5. An AI agent can submit low-risk claims automatically after passing traditional code edits, but complex appeals always require human sign-off. As a result, the best strategy is to let agents gather evidence and draft documents first. Thereafter, you should only grant autonomous submission permissions after live performance data proves complete reliability.



