
Key Takeaways:
-
AI EHR burnout solutions include ambient documentation, pre-charting, inbox management, and smart templates.
-
FHIR and HL7 integration, HIPAA controls, and physician review workflows are non-negotiable production requirements.
-
Specialty-specific note generation, EHR workflow automation, and burnout ROI dashboards drive measurable clinical impact.
-
Focused MVPs cost $70,000 to $140,000 while enterprise platforms reach $180,000 to $450,000 plus.
-
How Intellivon builds this: clinical workflow infrastructure reducing documentation time and click burden without removing clinician control.
An EHR burnout solution earns its place when it removes documentation from a physician’s day, and not just transcribes it. The features that achieve this fall into four categories, which include ambient voice documentation, pre-charting automation, specialty-specific template logic, and in-basket and inbox triage. These must run as one integrated workflow. These capabilities only work as a burnout solution when they run as one integrated system, not when each is adopted in isolation. An EHR burnout solution earns its keep when the architecture connecting them is designed correctly from the start.
What standard feature evaluations miss, though, is a consequential gap in how these components connect. Without adaptive, specialty-aware workflow learning in the documentation engine, ambient AI functions as a transcription upgrade while the physician’s load stays unchanged. When that layer is present, however, and documentation connects natively to pre-charting and inbox automation, the results are measurable: 82% of 7,260 Permanente physicians reported improved work satisfaction after deploying integrated ambient AI tools.
Intellivon has spent over ten years building clinical documentation AI with a compliance-first, specialty-aware architecture that evaluation teams consistently find missing in vendor conversations. This blog covers the full EHR burnout solution features framework, from ambient documentation and workflow automation to compliance controls and outcome metrics, so you leave with a working evaluation checklist.
What Is EHR Burnout Reduction Software?
EHR burnout reduction software is an enterprise technology layer designed to eliminate the manual data entry, clerical tasks, and click burden that cause clinical fatigue. Instead of forcing providers to navigate rigid user interfaces, this software automates clinical documentation, triages incoming inbox messages, and optimizes underlying medical workflows.
Consequently, physicians can shift their focus back to direct patient care while the background AI manages core compliance, billing, and structural data requirements.
What Does This Software Help Hospitals Achieve?
Hospitals deploy these specialized platforms to fundamentally restructure operational workflows and recover lost clinical capacity. Rather than treating electronic records as a manual logging chore, administrative leaders use intelligent automation to convert raw data inputs into clean assets.
This programmatic intervention stabilizes daily delivery metrics while directly protecting clinical teams from administrative exhaustion.
Core Organizational and Clinical Outcomes
The primary objective of this software layer is to compress the time spent on electronic maintenance and return hours back to patient care. By automating manual tracking and communications, hospitals achieve tangible performance gains across multiple departments.
- 70% Pajama Time Reduction: Eliminates late-night chart logging by drafting complex notes in real time during the patient encounter.
- Automated In-Basket Sorting: Filters routine patient portal messages and administrative notifications to reduce daily click burden.
- Enhanced Revenue Integrity: Captures accurate documentation metrics automatically, minimizing downstream insurance denial risks and coding errors.
Ultimately, eliminating systemic software friction directly stabilizes workforce metrics and slows down escalating clinician turnover rates. Replacing rigid data entry with intelligent automation allows health networks to achieve a durable balance between compliance and delivery.
Why Hospitals Are Investing in EHR Burnout Solutions Now
Health systems are aggressively deploying EHR burnout solution features because acute clinical documentation burden has surpassed manageable operational thresholds. Rather than viewing administrative fatigue as a static HR issue, enterprise executives now treat manual clinical logging as a direct threat to workforce retention and revenue integrity.
According to industrial data from Grand View Research, the U.S. AI medical scribing market is projected to skyrocket from $397.05 million in 2024 to $2,955.72 million by 2033, expanding at a sharp compound annual growth rate (CAGR) of 25.09%.
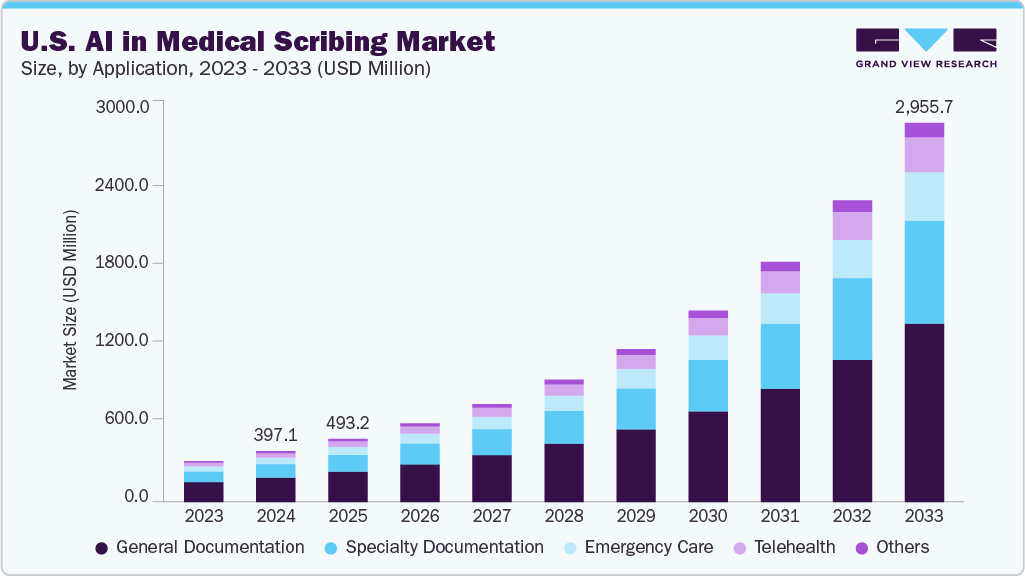
Consequently, health informatics buyers are rapidly shifting from localized departmental pilots toward massive enterprise-wide rollouts to capture sustainable time savings.
1. Unprecedented Adoption of Ambient AI Documentation Features in EHR
Large health systems are moving beyond basic transcription scripts to deploy fully continuous ambient listening platforms across their entire outpatient ecosystems. This rapid transition is validated by significant data-driven time savings achieved at major healthcare delivery organizations.
- Proven Capacity Reclamation: The American Medical Association (AMA) reported that The Permanente Medical Group utilized ambient AI scribes over 2.5 million times within a single year, recovering more than 15,000 document hours for their frontline clinicians.
- Rapid Voluntary Scaling: Demonstrating unprecedented organizational pull, the Cleveland Clinic scaled from an initial 250-doctor pilot to 4,000 voluntary clinician adopters in just 15 weeks, ultimately passing 1 million documented patient encounters.
2. Why Buyers Mandate a Comprehensive Feature Checklist
The massive explosion of emerging technology vendors has created a fragmented market filled with shallow wrappers that lack deep clinical integration capabilities.
Without a rigorous, technically sound requirement framework, hospital systems risk purchasing isolated software silos that fail under heavy production workloads.
- Integration Framework Planning: Teams must map out core HL7 and FHIR R4 API data requirements before selecting external vendors or committing to internal code builds.
- Operational Risk Mitigation: Enterprise buyers require pre-established checklists to evaluate model fine-tuning processes, dedicated BAA data agreements, and custom inbox routing logic.
Ultimately, the unprecedented shift toward enterprise-scale automated charting highlights a fundamental realization: administrative capacity can no longer depend on manual human labor.
By standardizing core integration, compliance, and UI requirements early, health networks successfully transform their existing technology layers into high-performing administrative assets.
Why EHR Burnout Needs More Than an AI Scribe
EHR burnout needs more than an AI scribe because physician workload spreads across the full clinical workflow.
Therefore, documentation matters, but so do inbox messages, pre-charting, chart search, order entry, quality documentation, coding support, and after-hours note completion. At the same time, a strong platform should reduce several types of work, not only generate clinical notes faster.
1. Managing the Growing Inbox Backlog
Electronic messaging queues are rapidly overwhelming clinical teams across the country. At the same time, doctors spend hours every single day triaging patient portal messages, refill requests, and simple administrative notices.
- Rising Communication Demands: Recent clinical informatics data shows that electronic message volume for medical specialists rose by 19%, causing severe administrative exhaustion.
- Patient Query Surges: Patient-initiated portal inquiries spiked by 34%, creating a continuous digital backlog that doctors must review after regular clinic hours.
- Constant Disruptions: This massive volume of incoming requests creates severe digital fatigue and interrupts direct patient care throughout the typical workday.
2. Reducing the Daily Click Burden
Navigating through dense electronic health record screens requires a massive amount of physical clicking. This repetitive process slows down standard medical workflows and frustrates providers who want to work efficiently.
- Excessive Screen Navigation: Frontline medical providers encounter an intense click burden, considering that a single chart documentation task can require 346 mouse clicks to complete.
- Fragmented Information Windows: Doctors must constantly click through 43 different user screens just to track simple clinical data points for a single patient.
- Operational Slowdowns: This heavy interface navigation drains mental energy, making total click burden reduction EHR capabilities an absolute necessity for health systems.
3. Eliminating Late Night Pajama Time
Many medical professionals are forced to finish their charting duties late at night. This practice destroys work-life balance and acts as a leading cause of industry attrition.
- Persistent After-Hours Work: Primary care clinicians who reduce their total face-to-face patient appointments by 32% only see their electronic record work drop by 21%.
- Systemic Tracking Overhead: This mismatch proves that deep administrative tasks remain high regardless of how many patients a doctor actually treats.
- Targeting Real Reclamation: Software must deliver major time in EHR reduction across the whole day to completely eliminate late-night administrative catch-up.
4. Improving Total Workspace Usability
Basic transcription scripts help draft sentences, but they completely fail to fix broader workspace layout issues. True efficiency requires an intelligent tool that streamlines every phase of the care delivery process.
- Fragmented Tool Deficiencies: Standalone recording gadgets operate in complete isolation, which leaves secondary paperwork like referral letters and after-visit summaries fully unoptimized.
- Fixing System Usability: Achieving real EHR usability improvement requires an end-to-end framework that simplifies ordering, coding, and message tracking simultaneously.
- Lowering Cognitive Load: Consolidating multiple clinical tracking windows into a simplified dashboard reduces cognitive strain and keeps doctors focused on patient care.
An AI scribe can reduce typing time, but it cannot solve every EHR pain point alone. At the same time, the right platform starts before the visit, continues during the encounter, and supports post-visit tasks.
Real Examples of EHR Burnout Reduction With AI Documentation
Hospitals are no longer treating EHR burnout tools as experimental software. At the same time, several large health systems have already tested ambient documentation and AI scribe platforms in clinical settings, with measurable improvements in burnout, documentation burden, cognitive load, physician satisfaction, and documentation-related well-being.
These real-world deployments provide a clear roadmap for organizations looking to scale their own infrastructure.
1. Mass General Brigham
Mass General Brigham provides the industry with the strongest direct example of measurable clinical burnout reduction using automated administrative tools.
Their recent enterprise evaluation focused heavily on tracking real-world clinical behavior and daily provider sentiment across diverse care settings.
- Drastic Attrition Mitigation: A landmark peer-reviewed study published in JAMA Network Open revealed that overall clinician burnout dropped sharply from 52.6% down to 30.7% at the 84-day mark following system adoption.
- Rapid Workflow Relief: This major drop was visible early in the deployment lifecycle, with initial 42-day checkpoint metrics showing burnout already falling from 50.6% to 29.4% among active platform users.
- Diverse Workforce Testing: The system validated these time-saving outcomes by analyzing continuous feedback from a large cohort of 873 participating physicians and advanced practice providers.
- Strategic Buyer Takeaway: Hospital leaders should use this data to prove that ambient AI clinical documentation tools directly lower workforce attrition. The strongest enterprise solutions must tie core software deployment directly to clear, trackable clinician well-being metrics.
2. Emory Healthcare
Emory Healthcare provides critical operational proof because their data tracks improvements in direct documentation-related well-being rather than just general workplace satisfaction.
Their informatics teams focused on how reducing interface friction changes a provider’s daily relationship with the electronic health record workspace.
- Massive Sentiment Improvement: The same joint research initiative published in JAMA Network Open showed that clinicians reporting a positive impact from their documentation practices jumped from a tiny 1.6% baseline to 32.3%.
- Targeted Documentation Relief: This massive shift proves that restructuring note creation workflows directly transforms how medical professionals experience their daily administrative tasks.
- Broad Operational Scale: The health system successfully evaluated these satisfaction changes across a pilot cohort of 557 clinicians spanning more than 45 distinct medical specialties.
- Strategic Buyer Takeaway: This case study shows that software evaluations must look beyond simple transcription speed. True solutions must actively improve how clinicians feel about their data-entry tasks by integrating smart templates and native physician review workflows.
3. The Permanente Medical Group
The Permanente Medical Group demonstrates what massive enterprise-scale adoption looks like when deployed across thousands of active clinicians.
Their regional leadership focused on testing ambient recording tools within heavy, high-volume production environments rather than isolated academic departments.
- Massive Operational Scale: According to official data published by the American Medical Association (AMA), more than 7,200 frontline physicians utilized ambient AI scribes to log over 2.5 million patient encounters within a single year.
- Aggregated Time Reclamation: This massive multi-department deployment successfully saved physicians a total of 15,791 documentation hours, which equals nearly 1,800 full eight-hour workdays recovered from administrative overhead.
- Elevated Care Delivery: Alongside massive documentation time reduction, 84% of surveyed clinicians reported a positive impact on patient communication, while 82% noted higher overall job satisfaction.
- Strategic Buyer Takeaway: Large healthcare networks must evaluate potential vendor platforms on their ability to handle massive enterprise data volume. True software solutions require deep native EHR integration and structured governance frameworks to successfully support thousands of simultaneous clinical users.
4. Six U.S. Health Systems
A comprehensive multicenter study highlights the rapid systemic impact of automated scribing platforms across highly varied corporate health environments.
This broad evaluation confirms that ambient time savings are highly repeatable outside of isolated, single-center hospital pilots.
- Consistent Multi-Site Success: Research covering six independent U.S. health systems confirmed that ambulatory clinic burnout dropped from 51.9% down to 38.8% within just 30 days of system activation.
- Statistically Significant Relief: This rapid operational improvement represented an impressive 74% lower odds of experiencing clinical burnout symptoms for participating providers.
- Accelerated Velocity Gains: The fact that significant cognitive relief appeared within the first month proves that advanced medical language models require very minimal user training to deliver value.
- Strategic Buyer Takeaway: Health IT buyers should recognize that fast, network-wide relief is achievable when deployment strategies focus on workflow fit. Organizations need structured implementation plans to ensure that immediate efficiency gains convert into permanent cultural improvements.
5. Included Health
Included Health serves as a premier real-world example of how custom-built AI solutions outperform generic, off-the-shelf software tools.
Their engineering teams chose to build a dedicated internal platform tailored explicitly to the unique data needs of their nationwide virtual care network.
- Custom Infrastructure Design: The organization built a proprietary ambient scribe system optimized for telemedicine documentation features, utilizing Whisper for audio transcription and GPT-4o for clinical note generation.
- High Internal Adoption: The specialized software layer was integrated directly into their native electronic health record platform, with more than 540 active virtual care clinicians using the tool in production.
- Overwhelming Clinician Validation: Internal surveys confirmed that 94% of practicing clinicians experienced reduced cognitive load, while 97% reported a measurable decrease in daily documentation burden.
- Strategic Buyer Takeaway: When generic commercial tools fail to align with unique clinical workflows or specialized interface layouts, building a custom platform is the right move. Tailored software ensures higher user adoption rates because the underlying code matches the health system’s exact operational logic.
Ultimately, enterprise tech buyers must demand that AI EHR burnout reduction platform features connect directly to verifiable clinician data points. Implementing a new software layer without a clear measurement baseline prevents organizations from proving a real return on investment.
The ideal platform must combine advanced automation tools with clear administrative dashboards to track, optimize, and protect your clinical capacity over time.
The Core Features Every EHR Burnout Solution Should Have
The core EHR burnout solution features include pre-charting support, ambient documentation, smart templates, inbox automation, EHR navigation support, coding assistance, compliance controls, analytics, and physician approval workflows.
These features work together to reduce documentation time, click burden, message overload, and after-hours charting across different clinical settings.
1. Master Feature Matrix for Health IT Evaluators
| Care Phase | Primary Feature Category | Core Administrative Focus | Target Technical Objective |
| Before the Visit | Pre-Chart Data Synthesis | Chart navigation and history retrieval | Reduce click burden and manual file search |
| During the Visit | Ambient Voice Pipeline | Real-time clinical transcription | Eliminate in-room typing and screen distraction |
| After the Visit | Automated Output Engine | Care continuity and sign-off paperwork | Compress the total time to sign clinical notes |
| Around the Visit | In-Basket and Flow Triage | Inbox automation and administrative tasks | Streamline messaging and complex prior auths |
| Enterprise Control | Production Integrity Layer | Compliance, privacy, and performance monitoring | Enforce strict HIPAA and BAA data protection |
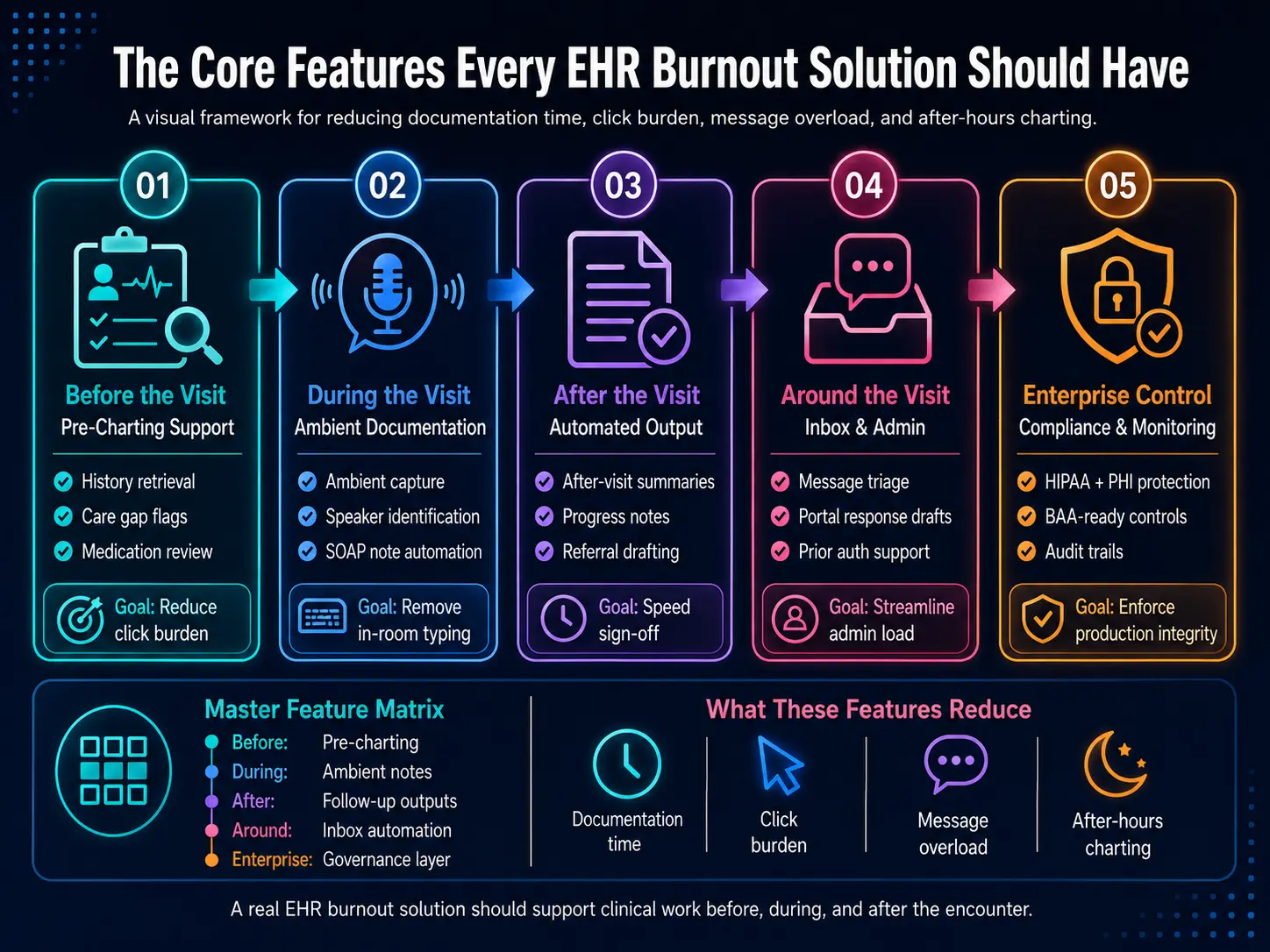
2. Feature Category 1 — Before the Visit
Pre-charting automation shifts the administrative burden away from the actual face-to-face patient encounter.
By compiling historical patient charts automatically, the system allows providers to walk into the exam room fully informed without spending 15 minutes manually opening historical chart tabs.
- RAG Patient History Retrieval: Pulls contextually relevant past medical records from deep archives using retrieval-augmented generation.
- Care Gap Identification: Flags missing routine screens, upcoming vaccinations, or delayed laboratory tests instantly based on age and history.
- Chronic Disease Documentation Automation: Synthesizes longitudinal data for complex cases like diabetes or hypertension before the appointment begins.
- Medication and Problem List Management: Suggests clean updates for outdated medication reconciliation automation, allergy list management, and active problem lists.
3. Feature Category 2 — During the Visit
Ambient voice documentation features EHR convert natural doctor-patient conversations directly into clinical text.
This real-time ambient AI documentation eliminates the laptop barrier, allowing physicians to maintain eye contact with patients rather than typing notes during the visit.
- Advanced AI Clinical Scribe Pipeline: Transforms unscripted multi-party conversations into structured medical sentences without requiring strict dictation commands.
- Speaker Identification Clinical System: Separates speech from the doctor, patient, and family members cleanly to prevent data misattribution.
- Background Noise Filtering Clinical AI: Isolates clear clinical audio even inside noisy pediatric units or chaotic emergency rooms.
- Real-Time SOAP Note Automation: Builds accurate, compliant structured notes instantly during natural patient conversations.
4. Feature Category 3 — After the Visit
An automated post-visit documentation engine eliminates the lingering paperwork tail that creates late-night charting drag.
By generating care continuity paperwork immediately after an encounter closes, the platform accelerates the final review cycle.
- After-Visit Summary Generation: Drafts clear, action-oriented, patient-facing summary automation texts regarding treatment plans and prescriptions.
- Progress Note Automation: Pre-populates relevant clinical data fields directly into daily inpatient charts to ensure continuity.
- Referral Letter Generation: Produces formatted consultation note automation texts and external referral letters based entirely on the visit data.
- Compressed Signature Timelines: Minimizes the total time to complete documentation, allowing physicians to sign off on files immediately.
5. Feature Category 4 — Around the Visit
Inbox management automation addresses the massive administrative load that occurs completely outside of physical patient visits.
This intelligent triage layer handles the constant influx of digital documentation requests that plague a provider’s electronic workspace.
- In-Basket Management EHR Triage: Categorizes incoming messaging queues automatically to separate urgent issues from routine notifications.
- Patient Portal Message Automation: Analyzes and drafts accurate contextual responses to basic, non-clinical patient inquiries.
- Prior Authorization Documentation Automation: Compiles required insurance paperwork by automatically extracting supportive data from past encounters.
- Quality Measure Documentation Automation: Links clinical actions directly to MACRA, MIPS, and meaningful use documentation metrics in the background.
6. Feature Category 5 — Enterprise Control
Enterprise control systems ensure that modern AI administrative tools meet rigid security, compliance, and clinical performance standards.
This technical layer transforms raw machine learning models into highly secure, production-grade hospital infrastructure.
- HIPAA Compliant AI Documentation: Protects sensitive patient data by enforcing end-to-end encryption across all data pipelines.
- PHI Protection AI Scribe Systems: Removes or sanitizes protected health information automatically during temporary transcript processing stages.
- BAA Requirements Compliance: Operates under strict, legally binding Business Associate Agreements required by enterprise health networks.
- Production MLOps Pipeline Tracking: Uses an explicit audit trail clinical documentation system alongside real-time model accuracy monitoring clinical tools.
This checklist gives buyers a clean way to separate useful tools from narrow AI demos. A real EHR burnout solution should support clinical work before, during, and after the encounter. The next section should start with the first workload physicians face: chart review before the visit.
Features That Reduce Pre-Visit Chart Review
Pre-visit chart review features help physicians understand the patient faster before the encounter begins. The system should summarize recent visits, diagnoses, medications, allergies, lab trends, imaging, referrals, care gaps, and open tasks.
At the same time, every summary should link back to the source chart data so clinicians can verify the information.
1. Automated History Summaries
Patient history summaries pull relevant details from the EHR and present them in a short, source-linked view.
The summary includes recent encounters, active problems, medication changes, allergies, test results, referrals, and unresolved follow-ups to maximize clarity.
- Contextual Data Aggregation: Uses RAG patient history retrieval and retrieval-augmented generation clinical pipelines to securely query long-term archives.
- Unstructured Text Parsing: Employs advanced NLP clinical note analysis and structured data extraction notes to isolate historical diagnoses.
- Native Enterprise Interoperability: Connects securely using standard FHIR R4 documentation API pipelines and traditional HL7 integration clinical notes.
- Deep Interface Embedding: Plugs into existing workflows via native Epic chart summarization tools and specialized Cerner integration AI scribe technical connection hooks.
This automated timeline compilation allows clinicians to prepare documentation requirements before the patient encounter officially begins.
2. Automated Care Gap Detection
Care gap tracking features identify missing preventive care, chronic disease requirements, HCC opportunities, and risk adjustment documentation needs before the physician opens the encounter.
The system prioritizes clinically relevant prompts to prevent system fatigue.
- Proactive Preventive Tracking: Drives automated care gap identification and preventive care documentation workflows based on patient age and history.
- Longitudinal Condition Tracking: Manages chronic disease documentation automation for complex cases like chronic kidney disease or cardiovascular illness.
- Payer Compliance Support: Optimizes HCC capture documentation and risk adjustment documentation support to track condition severity scores accurately.
- Administrative Metric Alignment: Streamlines quality measure documentation automation to easily satisfy complex MACRA MIPS documentation burden and meaningful use documentation rules.
By highlighting outstanding care parameters early, the platform transforms retrospective audit logs into proactive clinical assets.
3. Intelligent Chart Search
Intelligent chart search lets providers query the electronic health record using natural language phrases instead of manually digging through hundreds of old PDF scans.
This feature dramatically compresses file navigation timelines during complex pre-visit preparations.
- Semantic Concept Indexing: Locates specific clinical keywords across messy, unstructured legacy medical chart abstraction files and past handwritten consultation notes.
- Dynamic Timeline Filtering: Organizes scattered diagnostic events, surgical reports, and specialty-specific documentation templates into a single searchable log.
- Context-Aware Question Answering: Resolves precise inquiries regarding historical medication changes or past clinical findings using localized search indexing.
- Direct Grounded Citations: Links generated query results back to the original database row or patient document for instant accuracy verification.
Replacing standard manual text searches with semantic analysis prevents critical data from being overlooked before care begins.
4. Pre-Encounter Order Pre-Populating
Pre-encounter order pre-populating queues up relevant laboratory tests, follow-up imaging, and routine medication renewals based on the specific visit reason.
This capability streamlines interface operations before the provider enters the exam room.
- Adaptive Protocol Mapping: Suggests appropriate diagnostic orders by analyzing complex care gaps and structured patient history trends automatically.
- One-Click Batch Approval: Consolidates multiple diagnostic requests into a single screen to achieve real click burden reduction EHR benefits.
- Clinical Decision Support Integration: Evaluates drafted orders against drug interaction databases and institutional safety protocols to ensure patient safety.
- Pending Queue Management: Holds proposed orders in a secure draft status until the physician reviews and signs them.
Pre-populating routine clinical orders ensures that providers spend their day managing patient treatment rather than clicking checkboxes.
Deploying these four targeted pre-visit capabilities removes significant administrative drag before face-to-face appointments even begin. By condensing historical review and automated ordering into a single layout, health centers protect clinical energy.
After optimizing this pre-visit preparation phase, the platform can help clinicians document the live encounter naturally.
Features That Reduce Documentation Time
The best features for physician EHR burnout tools reduce documentation time without reducing note quality. These include ambient AI clinical documentation, SOAP note automation, specialty templates, real-time transcription, note completeness checks, and physician review workflows.
The goal is not automatic note signing. The goal is faster, safer draft creation.
1. Ambient AI Clinical Documentation
Ambient AI clinical documentation listens to the patient encounter, converts speech into text, identifies speakers, and creates a structured draft note.
At the same time, the system should support patient consent, background noise filtering, specialty vocabulary, real-time transcription accuracy, and physician review before anything enters the legal medical record.
Continuous Audio Processing and Ambient Voice Infrastructure
Transforming raw examination room conversations into highly structured text files requires a resilient acoustic processing pipeline. This clinical automation layer runs passively in the background so medical professionals can prioritize live patient communications rather than constant manual interface typing.
- Persistent Mobile Deployment: Operates via multi-device documentation support using specialized mobile EHR documentation tools and wearable microphone integration.
- Acoustic Signal Isolation: Employs advanced speaker identification clinical systems alongside hardware-level background noise filtering clinical AI algorithms.
- Asynchronous Content Ingestion: Processes multi-party medical dialogue using advanced post-visit transcription features and stable offline documentation capability.
- Empirical Impact Validation: Highlighting the scale of modern deployment, The Permanente Medical Group tracked 2.5 million ambient AI scribe uses, which saved their clinicians over 15,000 total hours of manual dictation.
2. Smart Templates and Specialty-Specific Notes
Smart templates should generate notes that match the specialty, visit type, physician style, and documentation requirements.
At the same time, a useful platform should support SOAP notes, progress notes, operative notes, consultation notes, discharge summaries, referral letters, and patient-facing summaries.
Contextual Structure and Multi-Department Chart Customization
A standard, one-size-fits-all text layout fails to capture the intricate technical data parameters across distinct medical branches. Modern solutions deploy smart template EHR systems and adaptive template learning to match the exact vocabulary and clinical goals of the active practice.
- Ambulatory Care Customization: Integrates outpatient documentation automation, multi-specialty documentation support, and specialty-specific documentation templates natively.
- Acute Care Tracking: Automates high-density charts through inpatient documentation automation, emergency medicine documentation, and progress note automation frameworks.
- Procedural Event Mapping: Generates complex records using surgical documentation automation, operative note generation, and discharge summary automation.
- Continuity Paperwork Creation: Speeds up external communication via referral letter generation, consultation note automation, and patient-facing summary automation.
- Virtual Encounter Optimization: Supports remote care delivery using dedicated telemedicine documentation features and remote patient monitoring documentation data streams.
3. Note Review and Completion Support
Note review features should help physicians approve documentation faster while preserving clinical responsibility.
Accelerating the data finalization loop requires a transparent data verification environment that helps providers check drafted materials quickly. At the same time, embedding real-time documentation feedback systems into the validation screen prevents structural compliance errors before final submission.
- Interactive Review Environment: Optimizes data verification through human-in-the-loop note review screens and native physician review and approval workflows.
- Structural Note Auditing: Uses real-time note completeness checking and documentation quality scoring to ensure optimal documentation accuracy rates.
- Operational Time Tracking: Monitors health network efficiency using continuous metrics like time to sign clinical notes and time to complete documentation.
- Reclaiming Personal Evenings: Measures direct lifestyle improvements by tracking measurable documentation after-hours reduction and physician pajama time reduction scores.
Deploying these three synchronized documentation features removes the primary administrative text-entry bottlenecks that cause widespread clinical exhaustion.
By transforming unstructured ambient speech directly into structured, specialty-compliant record drafts, health networks significantly lower cognitive overhead. While optimizing face-to-face dictation is essential, managing the surrounding electronic communication channels requires equal platform focus.
Features That Reduce Inbox and Admin Work
EHR burnout solution software features should include inbox and admin automation because physicians lose hours to patient messages, refill requests, forms, lab questions, prior authorization documentation, and routing decisions.
The platform should classify work, draft safe responses, route non-physician tasks, and escalate clinical issues that need review. This ensures that clinical communication remains manageable without overwhelming the provider’s screen.
1. Patient Portal Message Automation
Patient portal message automation should classify messages by intent, urgency, risk, and owner. At the same time, it should route scheduling, billing, and form requests away from physicians when possible.
By sitting directly inside the messaging pipeline, this capability prevents administrative queues from turning into a primary source of cognitive exhaustion.
- Contextual Queue Triage: Drives inbox management automation and in-basket management EHR workflows by sorting inbound files based on complex NLP classification models.
- Proactive Risk Management: Scans message text for high-risk phrases to trigger immediate red-flag symptom escalation protocols for urgent clinical issues.
- Automated Response Drafting: Utilizes historical data fields to execute safe, accurate draft response generation for non-urgent care inquiries.
- Dynamic Task Allocation: Assigns administrative files to appropriate personnel via role-based routing systems backed by continuous audit logging rules.
2. Prior Authorization and Form Support
Prior authorization documentation automation should pull clinical evidence from the chart, prepare payer-ready summaries, and show missing documentation before submission. It should reduce repetitive medical necessity writing without making coverage decisions.
This feature helps physicians, RCM teams, and administrative staff work from the same evidence base.
- Evidence Collection Automation: Accelerates prior authorization documentation automation by running instant clinical note retrieval and targeted evidence extraction queries.
- Compliance Document Generation: Pre-populates extensive justification sheets via automated medical necessity summary generation engines tailored to unique payer requirement checklists.
- Operational Validation Control: Maintains explicit human approval loops to verify all drafted administrative materials prior to system submission.
- Revenue Cycle Alignment: Connects cleanly with billing systems through revenue cycle management (RCM) integration hooks to drive continuous clinical documentation improvement.
- Federal Standard Adherence: Helps health systems naturally adapt to modern regulatory changes like the CMS 2026 Prior Authorization Rule (CMS-0057-F), which mandates electronic prior authorization (ePA) use to meet strict 7-day turnaround windows.
Once administrative communication burdens are successfully reduced, the platform must also simplify how clinicians navigate the core electronic record workspace itself.
Features That Make the EHR Easier to Use
EHR workflow automation burnout features should reduce the number of clicks, searches, tabs, and repeated entries physicians face during care. At the same time, useful features include EHR navigation automation, order context retrieval, smart shortcuts, clinical decision support integration, and structured field suggestions.
The system should assist physicians without taking unsafe autonomous actions.
1. EHR Navigation Automation
EHR navigation automation should open the right chart sections, retrieve relevant records, stage documentation fields, and reduce repetitive searching. At the same time, it should not create hidden actions inside the EHR.
Every automated action should be visible, permission-based, and logged for clinical and compliance review.
- Targeted Clicks Reduction: Achieves noticeable click burden reduction EHR metrics by bypassing deep, nested electronic folders automatically.
- Natural Search Queries: Employs a structured chart search system to find specific historical encounters or test reports instantly.
- One-Touch Interface Shortcuts: Launches pre-configured smart shortcuts that load complete multi-tab layouts tailored to standard clinical situations.
- Granular Permission Isolation: Protects information pipelines using role-based access clinical documentation filters alongside a verifiable audit trail clinical documentation log.
- Legacy Infrastructure Adaptation: Outlines clear Epic and Cerner workflow constraints to make sure background scripts match native platform execution rules.
2. Order and Decision Support Assistance
Order entry automation should assist with context, not replace clinician judgment. The platform may suggest order sets, retrieve prior results, flag missing information, or stage draft actions.
However, the physician should confirm orders, prescriptions, referrals, and clinical decisions before anything becomes active.
- Predictive Order Entry: Runs intelligent order entry automation setups that suggest logical diagnostic paths based on active visit codes.
- Unified Safety Verification: Drives background clinical decision support integration loops to flag medication contradictions or allergy conflicts early.
- System Conciliatory Processing: Simplifies coordination tasks through automated medication reconciliation automation, allergy list management, and problem list management automation tools.
- Proactive Wellness Alignment: Pre-stages preventive care documentation forms to simplify institutional value-based care reporting requirements.
- Strict Alert Control Guardrails: Minimizes system alert fatigue by replacing standard intrusive pop-up windows with passive physician approval workflows.
Optimizing basic record navigation and order staging structures significantly reduces the micro-frustrations that accumulate over a doctor’s workday. By handling repetitive screen-switching tasks quietly in the background, the interface matches the quick logical flow of a live clinical encounter.
While streamlining workspace layout helps, tracking the financial and integration realities of building these modules remains essential.
Features That Keep Patient Data Safe
HIPAA-compliant AI documentation requires security, privacy, access control, auditability, and clear vendor responsibilities.
Any AI scribe EHR burnout solution features checklist should ask where audio, transcripts, prompts, draft notes, final notes, and model logs are stored. At the same time, the platform must protect PHI across every workflow stage.
1. PHI Protection and Vendor Agreements
PHI protection AI scribe requirements should cover data capture, processing, storage, access, retention, deletion, and vendor use.
At the same time, BAA requirements for AI scribe vendors should clarify safeguards, subcontractors, breach duties, model training restrictions, and data ownership before any patient encounter data enters the platform.
2. Strict Technical and Regulatory Boundaries
Enforcing digital privacy mandates requires hard-coded rules that govern data at rest and in motion.
Modern systems implement these rigorous protocols to meet the 2026 HIPAA Security Rule updates, which eliminate previous “addressable” categorization and mandate strict technical compliance across all networks.
- Universal Data Protection: Enforces advanced encryption in transit and at rest across all clinical databases and storage buckets using minimum AES-256 standards.
- Access Environment Enforcements: Integrates multi-factor authentication and role-based access clinical documentation limits to prevent unauthorized chart access.
- Ephemeral Audio Pipelines: Configures immediate audio retention rules that purge patient recordings automatically within seconds of final transcript delivery.
- Zero-Retention Model Policies: Restricts vendor model training through legally binding clauses preventing the usage of clinical inputs for foundational optimization.
- Informed Consent Gathering: Captures explicit patient consent indicators before starting background ambient record devices during live clinic interactions.
3. Audit Logs and Model Monitoring
Audit logs should show who captured, generated, reviewed, edited, approved, exported, and signed every note. Model monitoring should track transcription errors, hallucinations, omissions, unsafe drafts, edit patterns, specialty performance, and drift.
These controls help hospitals trust the system after deployment.
4. Statistical Auditing and Engineering Oversight
Deploying AI inside high-stakes clinical spaces requires a permanent technical verification architecture.
At the same time, by checking processing metrics and user behaviors continuously, healthcare IT teams protect operational networks from severe code degradation or logic shifts.
- Tamper-Proof Data Logging: Maintains an unbroken audit trail of clinical documentation log tracking every micro-edit made to machine-generated drafts.
- Production Pipeline Control: Evaluates live algorithmic behaviors through a structured MLOps documentation AI pipeline with continuous model accuracy monitoring clinical tools.
- Drift Analysis Systems: Detects specialty-level drift across separate departments to ensure vocabulary tools remain precise across varied practices.
- Iterative Learning Control: Uses safe continuous learning documentation AI models to analyze localized user edit behaviors without retaining raw patient data.
- Safety Interception Queues: Routes low-confidence generated materials directly into specialized safety review queues for validation before clinical display.
Enforcing these strict data governance and system tracking rules ensures that administrative optimization never undermines patient privacy obligations.
By hard-coding universal encryption, rapid session purges, and persistent drift monitoring into the system layer, health systems fulfill modern data-security expectations.
Safety and privacy ensure the platform functions responsibly in live clinical areas, which allows administrators to pivot toward calculating actual fiscal and operational returns.
How Hospitals Can Measure Burnout Reduction
Hospitals should measure burnout reduction through EHR activity data, documentation metrics, inbox metrics, adoption trends, and physician feedback.
At the same time, a platform can generate many notes and still fail if physicians spend the saved time correcting drafts, handling messages, or finishing work after hours.
1. The Burnout Reduction Scorecard
A Burnout Reduction Scorecard connects each feature to a measurable workload outcome.
Instead, it should track documentation time reduction, time in EHR reduction, click burden reduction, after-hours work, note signing speed, message touches, and physician satisfaction. This makes burnout improvement visible to clinical and financial leaders.
2. Complete Feature and Workload Metric Mapping
| Feature | Workload It Should Reduce | Main Metric | Target Outcome |
| Ambient AI documentation | Typing and note drafting | Documentation time reduction | 25–40% reduction |
| Pre-charting automation | Chart search | Time in EHR before visit | 20–30% reduction |
| Inbox automation | Message triage | Physician touches per message | 30–50% reduction |
| Smart templates | Editing and formatting | Time to sign clinical notes | 20–35% reduction |
| EHR navigation automation | Clicking and tab switching | Click burden reduction EHR | 15–25% reduction |
| Analytics dashboard | Invisible after-hours work | Pajama time reduction for physicians | 20–35% reduction |
3. Key Operational and Experience Metrics Explained
Evaluating administrative platforms requires tracking both technical system speeds and direct human sentiment data. At the same time, hospital operations leaders look at automated usage dashboards alongside external validation scores to confirm long-term workflow improvements.
An enterprise platform must run a continuous documentation analytics dashboard that calculates saved minutes per clinical chart automatically. This automated monitoring separates actual system performance from subjective user estimates during deployment reviews.
- Granular Time Logging: Captures the exact moments spent inside chart windows to compile clear time savings reporting data points.
- Proving Financial Value: Connects recovered administrative hours to standard operational ROI measurement documentation tools across different clinics.
- Tracking Hidden Overhead: Isolates actual documentation after-hours reduction gains to verify that work stays within the standard shift.
4. Advanced Clinician Experience and Wellbeing Metrics
True software success must show up in independent workforce retention indicators and validated industry surveys.
At the same time, system changes should directly improve standard medical tracking scores by removing day-to-day software friction.
- Standardized Quality Benchmarks: Aligns interface performance with KLAS Research’s Arch Collaborative Executive Scorecard to track overall EHR satisfaction improvements.
- Industry Burnout Realities: Addresses key system pain points, noting that KLAS indicates 62% of burned-out physicians directly point to the EHR as a primary source of work distress.
- Measuring Workforce Alignment: Compares platform adoption rates against the Press Ganey State of Healthcare Employee Experience Report, which shows that highly engaged health systems experience 9% lower employee turnover rates.
- Subjective Strain Reductions: Measures real clinician well-being metrics to ensure that ambient tools successfully lower daily stress scores.
Tracking these combined technical and cultural metrics allows large hospital networks to confirm clear operational benefits.
Moving from unstructured software use to verifiable tracking ensures that technology choices actively support workforce stability. Once ROI metrics are clear, the reader needs cost clarity.
How Much Does an EHR Burnout Solution Cost?
A custom EHR burnout solution usually costs $70,000–$140,000 for a focused MVP and $180,000–$450,000+ for an enterprise platform.
This cost increases with ambient AI documentation, EHR write-back, specialty templates, inbox automation, HIPAA controls, analytics dashboards, model monitoring, and multi-site deployment requirements.
1. Complete Development Phase Cost Structure
| Development Phase | What It Includes | Estimated Cost |
| Discovery and workflow mapping | Clinician interviews, EHR audit, workflow mapping, baseline metrics | $8,000–$20,000 |
| Product architecture and UX | Feature roadmap, user flows, physician approval workflows, system design | $15,000–$35,000 |
| AI documentation MVP | Audio capture, transcription, SOAP note automation, review workflow | $35,000–$80,000 |
| EHR integration | FHIR, HL7, Epic, Cerner, Meditech, athenahealth, note write-back | $30,000–$100,000 |
| Inbox and admin automation | Message routing, portal drafts, forms, prior authorization support | $25,000–$75,000 |
| Compliance and security | HIPAA controls, RBAC, audit logs, encryption, BAA support | $20,000–$60,000 |
| Analytics and ROI dashboard | Time savings, documentation metrics, burnout scorecard, adoption tracking | $20,000–$55,000 |
| MLOps and model monitoring | Accuracy checks, drift monitoring, retraining, performance dashboards | $25,000–$70,000 |
2. Ongoing Maintenance Cost
Annual maintenance usually costs 18–25% of the initial build. This covers model monitoring, EHR API updates, compliance reviews, template improvements, bug fixes, infrastructure, and new specialty workflows.
Cost should be judged against time saved, after-hours work reduced, physician adoption, and documentation quality improvement. At the same time, a cheaper tool may cost more later if it creates copy-paste work or weak EHR integration.
Build vs Buy: Which Option Makes More Sense?
Hospitals should buy when they need fast AI scribe deployment for standard documentation workflows. Instead, they should build or customize when they need enterprise EHR burnout solution features across multiple specialties, inbox work, EHR navigation, coding support, compliance controls, analytics ownership, and deep integration with existing clinical systems.
1. Buy When the Need Is Narrow
Buying is usually better when the organization mainly needs AI note drafting for outpatient visits.
At the same time, vendor tools can move faster when templates are standard, integration needs are limited, and the clinical team wants a short pilot. This works best when workflow control is not the main requirement.
2. Advantages of Immediate Commercial Software Adoption
Opting for a commercial vendor allows health systems to address immediate documentation bottlenecks with minimal development delays.
At the same time, ready-made options provide a predictable path for standard outpatient settings where data formats remain constant.
- AI Scribe EHR Burnout Solution Features: Access pre-trained models optimized for basic conversational speech recognition out of the box.
- Ambient AI Documentation: Deploy passive listening software immediately within standard, low-complexity ambulatory exam rooms.
- Basic Note Generation: Produce structured text summaries like standard SOAP formats without needing custom data mapping.
- Fast Rollout Realities: Launch the application across targeted clinics within a matter of weeks rather than planning a multi-month development lifecycle.
- Lower Upfront Cost: Avoid significant initial capital expenditures by using predictable, subscription-based software-as-a-service (SaaS) pricing models.
- Vendor-Managed Updates: Rely on the external technology provider to handle ongoing server maintenance, core feature expansions, and model updates.
3. Build When the Workflow Is Complex
Building is usually better when the organization needs deep workflow control, specialty-specific documentation, internal analytics, privacy rules, and multiple automation layers.
Consequently, custom development fits hospitals, health IT vendors, and large ambulatory groups that want the platform to support documentation, inbox, coding, quality, and EHR navigation together.
Strategic Advantages of Custom Engineering Projects
Designing a dedicated, internal solution ensures that the underlying software aligns perfectly with the unique infrastructure requirements of an enterprise network.
This comprehensive customization transforms basic transcription utilities into a long-term clinical asset that optimizes multiple departments simultaneously.
- Enterprise EHR Burnout Solution Features: Create a unified platform designed to handle large-scale, multi-facility data volume and high-density clinical traffic.
- Multi-Specialty Documentation Support: Program tailored charting logic to support complex areas like emergency medicine, inpatient rounding, and surgical workflows.
- EHR Workflow Automation Burnout Features: Automate complex clerical actions including in-basket message triaging, prior authorization forms, and order pre-population.
- FHIR and HL7 Integration: Build direct, bidirectional data write-back pipelines that sync data into proprietary database structures.
- Internal Analytics and MLOps Ownership: Maintain complete ownership over your clinical data streams, performance dashboards, and foundational model accuracy monitoring clinical tools.
- Custom Compliance Rules: Enforce rigid institutional security frameworks, custom audio retention policies, and localized data sanitization boundaries.
Build vs buy is a control decision around workflow, data, compliance, integrations, and long-term product ownership. Therefore, choosing the right path requires evaluating whether your operational goals fit a standard commercial box or demand a tailored infrastructure framework.
Build EHR Burnout Reduction Software With Intellivon
Intellivon designs EHR burnout reduction software, so clinical teams can reduce documentation burden, inbox overload, chart review time, and after-hours work without removing physician control. Every AI-generated note, summary, message draft, or workflow suggestion is built to remain reviewable, editable, traceable, and governed.
This gives hospitals, ambulatory care networks, and health IT vendors a safer way to use AI documentation and EHR workflow automation without creating black-box notes, unsupported clinical summaries, compliance gaps, or additional review work for physicians.
1. What Intellivon Helps You Build
- Ambient AI documentation workflows: Capture physician-patient conversations, convert speech into structured notes, and generate SOAP notes, progress notes, consultation notes, discharge summaries, referral letters, and patient-facing summaries for physician review.
- Pre-charting automation systems: Pull patient history, recent encounters, medications, allergies, lab trends, imaging references, care gaps, and open tasks into one source-linked clinical summary before the visit begins.
- Physician-approved note generation: Generate first-draft clinical notes that physicians can edit, approve, reject, or send back for correction before anything enters the legal medical record.
- Specialty-specific documentation templates: Build templates for outpatient care, inpatient rounding, emergency medicine, surgery, behavioral health, telemedicine, chronic disease management, and remote patient monitoring workflows.
- Inbox and in-basket automation: Classify patient portal messages, refill requests, lab questions, form requests, administrative tasks, and clinical escalations so care teams can route work to the right owner.
- Patient message draft support: Generate patient-facing response drafts with clear clinical context while keeping physicians, nurses, or care team members in control of final approval.
- EHR navigation and workflow automation: Reduce repeated chart search, tab switching, field entry, and documentation steps through permission-based EHR workflow support.
- Clinical documentation quality checks: Review notes for missing history, assessment, plan, medication updates, follow-up instructions, quality measure fields, coding support, and CDI gaps before signing.
- Source-linked clinical summaries: Connect each generated summary or note section to the patient record, encounter detail, lab result, medication list, previous note, or care gap that supports it.
- Human-in-the-loop approval controls: Keep physicians, clinical informatics teams, and care leaders in full control of note approval, message approval, workflow changes, exceptions, and escalations.
- Burnout reduction analytics: Track documentation time reduction, time in EHR reduction, click burden reduction, after-hours documentation, note completion speed, inbox load, and clinician wellbeing trends.
- HIPAA-ready deployment architecture: Build secure, access-controlled AI documentation workflows with encryption, role-based access, audit logs, PHI safeguards, data retention rules, and model governance.
2. When to Build EHR Burnout Reduction Software
A custom EHR burnout reduction platform makes sense when physicians spend too much time completing notes, reviewing charts, answering inbox messages, fixing documentation gaps, or finishing EHR work after clinic hours.
It is also useful when generic AI scribe tools cannot match your specialty workflows, EHR environment, compliance rules, or internal reporting needs.
This build is especially relevant if your organization manages high patient volumes, multiple specialties, complex documentation requirements, heavy in-basket activity, chronic disease workflows, quality reporting needs, or fragmented EHR processes.
In these cases, a standalone AI scribe may help with notes, but it will not solve the full burnout workflow.
3. What You Get Before Full Development Begins
Before engineering starts, Intellivon helps your team define the EHR burnout workflow, clinical documentation gaps, integration needs, AI boundaries, reviewer permissions, compliance risks, and technical scope. This gives clinical, operational, and technology leaders a clear build plan before investing in a production platform.
The early-stage roadmap can include:
- Physician workflow and documentation burden assessment.
- Current EHR activity and after-hours work review.
- Pre-charting, note drafting, inbox, and admin workflow mapping.
- Specialty-specific template and note-type planning.
- Epic, Cerner, Meditech, athenahealth, FHIR, and HL7 integration review.
- Ambient AI documentation architecture planning.
- Patient history retrieval and source-linking design.
- Human-review and physician approval workflow design.
- HIPAA, PHI, audit-log, and role-based access requirements.
- Model accuracy, hallucination-control, and clinical safety framework.
- Documentation analytics and ROI measurement planning.
- MVP scope, cost range, timeline, and rollout roadmap.
4. Why This Matters
AI can reduce EHR burnout only when it removes real clinical work. A weak implementation may generate polished notes while physicians still spend time correcting drafts, answering inbox messages, searching through charts, or completing documentation after hours.
That balance matters because EHR burnout is not just a documentation problem. It is a clinical operations problem where time, accuracy, patient context, compliance, physician trust, and workflow adoption all matter.
If your organization is evaluating EHR burnout solution features, start with a workflow and documentation-readiness review before choosing models or vendors. Talk to Intellivon to scope your AI documentation architecture, EHR integration requirements, physician review controls, HIPAA safeguards, analytics dashboard, development cost, and rollout roadmap before committing to a full build.
Conclusion
EHR burnout solution features should remove real work from the physician’s day, not only generate faster notes. The strongest platforms connect ambient documentation, pre-charting, inbox automation, smart templates, EHR navigation, coding support, compliance controls, and ROI tracking.
As ambient AI scribes show measurable reductions in administrative burden and burnout, hospitals should judge every platform by verified time saved, fewer clicks, less rework, and reduced after-hours documentation.
Things To Know About EHR Burnout Solution Features
Q1. What should EHR burnout software include?
A1. EHR burnout software should include ambient documentation, pre-charting automation, inbox management, smart templates, EHR navigation support, physician approval workflows, HIPAA controls, EHR integration, and ROI analytics. More importantly, it should reduce documentation time, click burden, message load, and after-hours work together, because burnout usually comes from connected workflow pressure, not one task.
Q2. How much do AI EHR burnout reduction platform features cost?
A2. AI EHR burnout reduction platform features usually cost $70,000–$140,000 for an MVP and $180,000–$450,000+ for an enterprise build. However, the final budget depends on ambient documentation, Epic or Cerner integration, specialty templates, inbox automation, compliance controls, analytics, model monitoring, and whether the platform supports one department or multiple sites.
Q3. What are the best features for physician EHR burnout tools?
A3. The best features for physician EHR burnout tools are ambient AI documentation, patient history summaries, smart templates, inbox triage, note quality checks, coding support, and time savings dashboards. Together, these features reduce work before, during, and after the visit. As a result, physicians spend less time documenting and more time focusing on care.
Q4. Are ambient AI documentation features EHR systems safe for PHI?
A4. Ambient AI documentation features can be safe for PHI when the platform includes HIPAA safeguards, a BAA, encryption, access controls, audit trails, retention rules, patient consent, and clear model training restrictions. However, buyers should verify where audio, transcripts, prompts, and notes are stored before rollout, because privacy risk depends on architecture.
Q5. Should hospitals build or buy an EHR burnout platform?
A5. Hospitals should buy when they need fast AI scribe support for standard outpatient documentation. However, they should build or customize when they need workflow control across documentation, inbox, coding, EHR navigation, specialty templates, compliance, and analytics. Therefore, the decision should follow workflow complexity, integration depth, and governance needs, not hype
To Sum Up
- An AI scribe can reduce typing, but it will not fix EHR burnout if physicians still handle the same inbox, chart review, and admin workload.
- EHR burnout reduction should be measured through EHR activity data, not only clinician feedback surveys.
- The best EHR burnout platforms connect documentation, inbox work, coding, compliance, and analytics into one workflow layer.
- FHIR and HL7 integration determine whether AI documentation becomes daily infrastructure or another copy-paste tool.
- Custom development makes sense when hospitals need control over specialty templates, PHI rules, model monitoring, and ROI measurement.



