

Key Takeaways:
-
Denial prevention AI includes EDI 837 validation, eligibility verification, prior authorization, and payer-specific models.
-
NCCI edit validation, LCD/NCD compliance checking, real-time risk scoring, and explainability are core requirements.
-
NLP clinical review, MLOps, HIPAA controls, and human-in-the-loop review ensure production-grade platform reliability.
-
Internal platforms cost $120,000 to $420,000, while multi-payer SaaS builds reach $450,000 to $750,000 plus.
-
How Intellivon builds denial prevention as secure revenue-cycle infrastructure where model, workflow, compliance, and ROI integrate.
Building denial prevention AI costs between $180,000 and $600,000, depending on model complexity, payer scope, and integration depth, because this is infrastructure, and not a feature you add later. At the same time, revenue cycle teams losing 5–10% of claims to denials are dealing with a prediction gap, and closing that prominent gap takes purpose-built AI platforms.
The difference between a platform that prevents denials and one that only flags them comes down to one architectural decision: whether payer-specific behavior modeling sits inside the ML core from day one, or comes in later out of context. This is why organizations that get this right recover first-pass acceptance rates by 20–30% within 12 months, and the AMA’s $25–$181 rework cost per denial makes the ROI case without a calculator.
Intellivon has spent over a decade building denial prevention AI, with HIPAA compliance designed at the architecture level, not retrofitted, which is the piece revenue cycle leaders are looking for before they can articulate why. This post covers costs by phase, what moves them, and what you’ll need for the budget case.
What is a Denial Prevention AI Platform?
A denial prevention AI platform checks claims before submission and flags the ones likely to be denied. It validates coding accuracy, payer rules, patient eligibility, and clinical documentation in real time. Because of this, issues get fixed before they reach the payer, not after a denial comes back. The result is a higher first-pass acceptance rate and less time spent on rework.
Why Are Organizations Adopting It Now?
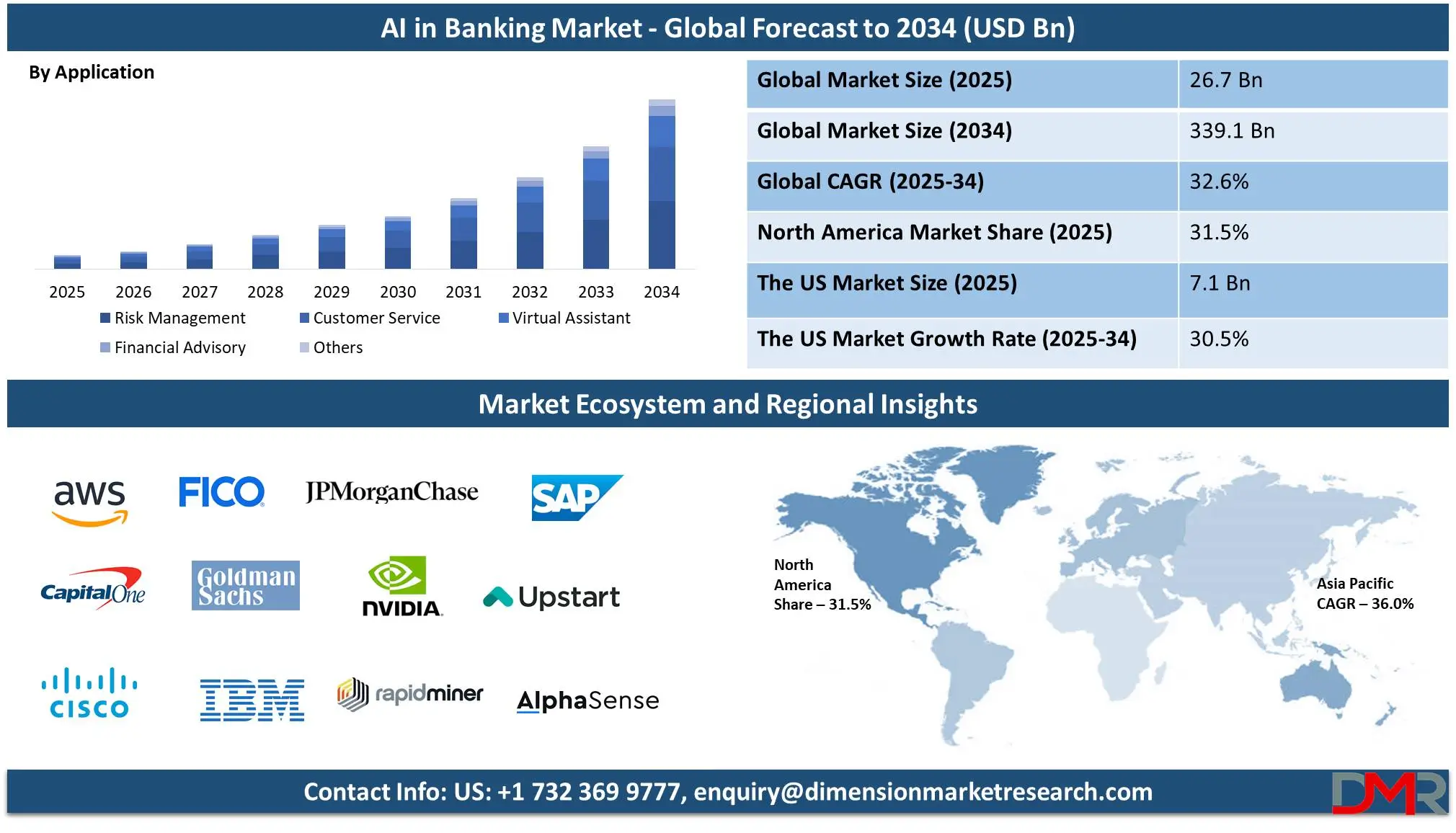
Banks are rushing to deploy AI-powered fraud and denial prevention platforms as the global AI in banking market surges at a 32.6% CAGR, projected to reach $339.1 billion by 2034. At the same time, traditional rule-based systems can’t keep pace with sophisticated cybercriminals, forcing banks to adopt real-time AI detection.
1. Fraud Detection Crisis Demands AI Solutions
Digital transactions have exploded, making cyber threats and financial fraud a major regulatory concern. 98% of banks either already use or plan to use generative AI, which is the highest adoption rate among all industries. Traditional systems simply cannot detect sophisticated fraud patterns in real-time.
2. Proven ROI Drives Rapid Adoption
The business case is undeniable. American Express saw +6% fraud detection using LSTM AI models, while PayPal achieved +10% real-time fraud improvement. 55% of U.S. banking leaders already recognize AI benefits, with virtually every major bank running financial AI pilot programs for fraud detection, chatbots, and credit risk.
3. Competitive Pressure and Strategic Shifts
Citigroup acquired Feedzai, an AI risk management platform, in November 2024, signaling the industry’s decisive move. Within five years, AI readiness will separate leaders from laggards.
Banks that delay adoption risk losing competitive advantage as AI becomes the baseline for modern banking operations.
4. Real-Time Detection Capabilities
AI can mine large datasets instantly for swift threat responses, enabling automated security operations and behavioral biometrics that prevent unauthorized access.
This real-time capability is critical for preventing DDoS attacks and transaction denials that conventional systems miss.
The momentum combines competitive pressure with clear early wins, such as cost reductions and improved customer engagement, making AI denial prevention platforms essential, not optional.
How Much Does Denial Prevention AI Cost to Build?
Denial prevention AI development usually costs $120,000–$420,000+ for a production-grade internal platform, depending on payer mix, claim volume, EHR complexity, rules-engine depth, AI model scope, and HIPAA requirements.
A narrow MVP can start near $75,000, while commercial multi-tenant SaaS platforms can exceed $750,000.
| Development Phase | Estimated Cost Range | What It Covers |
| Discovery and denial economics audit | $10,000–$25,000 | Denial baseline, payer mix, CARC/RARC analysis, workflow mapping |
| Data pipeline and denial taxonomy | $25,000–$70,000 | EDI 837, 835, claims history, eligibility, authorization, documentation data |
| Payer rules engine | $35,000–$110,000 | NCCI edits, LCD/NCD logic, payer-specific rules, medical necessity checks |
| AI model development | $45,000–$140,000 | Denial prediction model development, XGBoost, gradient boosted trees, NLP, confidence scoring |
| EHR, PMS, clearinghouse, payer integrations | $50,000–$160,000 | FHIR R4 API, HL7 CDA, Epic, Cerner, clearinghouse, payer API connections |
| Workflow and dashboard layer | $35,000–$95,000 | Human review, alert routing, denial prevention dashboard, work queues |
| HIPAA, audit, security, and MLOps | $35,000–$105,000 | PHI tokenization, RBAC, zero-trust architecture, audit trail, model drift monitoring |
| QA, validation, deployment | $25,000–$75,000 | UAT, claim simulation, payer scenario testing, production release |
Ongoing maintenance cost: Plan for 18%–28% of the initial build cost per year. This covers payer rule decay management, retraining pipeline cost, model versioning, security updates, integration monitoring, QA regression testing, and new payer policy mapping.
1. Understanding the Variables in Your Financial Blueprint
The total price fluctuates because engineering hours scale with system complexity. For example, a single-specialty hospital network with one primary payer requires fewer specialized models than a multi-state health system. Specifically, your team must account for historical data differences across commercial carriers, Medicaid, and Medicare.
For a deeper breakdown of claims workflow integrations, see our guide on AI healthcare claims processing software development
Security frameworks also dictate financial investments. Implementing a zero-trust architecture with complete protected health information tokenization requires specialized security engineers. Therefore, skipping these early structural steps can create massive non-compliance liabilities that erase initial development savings.
In summary, building an enterprise-grade prevention platform requires a structured financial commitment ranging from $120,000 to over $420,000, supplemented by an ongoing annual maintenance budget. The real budget is not one AI model. Instead, it is the full prevention layer around the model.
Why Denial Prevention Costs More Than Denial Prediction
Denial prevention costs more than denial prediction because it must fix claim risk before submission, not just forecast it. A prediction tool flags risk.
On the other hand, a prevention platform validates eligibility, authorization, coding, documentation, payer rules, medical necessity, charge capture, and claim edits before the claim leaves the billing workflow.
1. Denial Prediction vs Denial Prevention
| Capability | Denial Prediction | Denial Prevention |
| Main purpose | Scores denial probability | Stops preventable denial triggers before submission |
| Core data | Historical denials, 835 files, payer behavior | Claims, eligibility, authorizations, clinical notes, payer rules, coding edits |
| Output | Risk score | Risk score + correction path |
| Technical layer | ML model and dashboard | ML model, rules engine, NLP, EHR workflow, claim validation |
| Cost impact | Lower | Higher because more systems must connect |
2. The Infrastructure Gap Between Scoring and Correcting
Analytical tools only look backward at historical claim outcomes to generate a basic risk score. Consequently, the initial denial prediction model development cost remains relatively low because it does not interact with live clinical systems. However, real-time denial risk scoring cost escalates when you move from static reports to active intervention within the revenue cycle.
True mitigation requires a multi-layered software architecture that intercepts claims inside the billing department pipeline. Specifically, your team must budget for an AI pre-submission denial prevention cost that includes the following engineering layers:
- Algorithmic Forecasting: Machine learning models that calculate real-time denial probability scores before a claim leaves your billing workflow.
- Programmatic Correction: A translation layer that converts abstract risk flags into specific, step-by-step resolution paths for billing specialists.
- Dynamic Claims Scrubbing: A custom claims scrubbing AI development cost to replace rigid, hardcoded legacy edits with an engine that adapts to changing carrier policies.
For a deeper breakdown of the prediction layer, see our guide on [AI Denial Prediction Software Development for Hospitals].
3. The Financial Reality of Clinical Integration
Building an automated mitigation engine means engineering deep connections into your patient documentation pipelines. Therefore, a major driver of overall expenses is the clinical documentation denial prevention cost.
This deep integration requires two primary architectural systems to run simultaneously:
- NLP Text Analysis: Natural language processing pipelines that read unstructured physician notes to verify that the documented care matches the billed codes.
- Payer Rules Engine: A custom payer rules engine development cost to automatically check clinical data against localized coverage determinations and insurance contracts.
As a result, the platform catches complex errors before they cause an administrative rejection.
In summary, prediction tools simply expose revenue risks after the clinical encounter has already concluded. Prevention platforms require a much larger financial investment because they actively modify workflows to eliminate errors before submission.
The Denial Prevention AI Architecture That Drives Cost
Denial prevention AI architecture has five cost-driving layers: data ingestion, rules validation, AI risk scoring, workflow routing, and compliance governance.
Each layer adds cost because it must work with real claims, real payer policies, clinical documentation, EHR data, clearinghouse workflows, and PHI security controls.

| Architecture Layer | Core Cost Drivers | Operational Impact |
| 1. Data Foundation | EDI parsing, historical labeling, CARC/RARC mapping | Creates clean, unified data inputs for AI models |
| 2. Rules Validation | NCCI edits, LCD/NCD compliance, custom policy engines | Catches hardcoded billing and medical necessity errors |
| 3. ML & NLP Modeling | XGBoost models, text analysis, SHAP explainability | Predicts complex denials and reads unstructured text |
| 4. Workflow Integration | Alert routing, CDI automation, custom dashboards | Puts actionable insights into the hands of billing staff |
| 5. Security & MLOps | PHI tokenization, RBAC, drift tracking, audit logs | Guarantees HIPAA compliance and prevents model decay |
Layer 1 — Claims and Revenue-Cycle Data Foundation
The data foundation layer converts messy, fragmented billing histories into a clean, structured stream for machine learning models. Specifically, engineering this layer requires your development team to build custom parsing engines for electronic insurance files.
- EDI 837 validation cost: Engineering automated checks to ensure outbound digital claim files match strict clearinghouse formats.
- Historical denial data labeling cost: Paying data engineers to organize thousands of old claims so the AI can learn from past mistakes.
- CARC RARC analysis cost: Creating a classification engine that reads standard insurance denial reason codes to understand exactly why claims were rejected.
- Front-End Automations: Building background software modules for eligibility verification automation, prior authorization checking cost, and real-time charge capture validation cost.
Consequently, this foundational layer ensures that your downstream AI components do not process inaccurate patient or insurance data. The next step is building the logic layer to evaluate these clean data streams against active medical policies.
Layer 2 — Rules Engine and Policy Validation
The rules engine layer evaluates claims against millions of active insurance rules to stop technical billing errors before submission. Because insurance companies change their rules constantly, this module cannot rely on static, old-school software spreadsheets.
- Payer-specific denial model cost: The price to build custom logic patterns for individual insurance companies like Aetna, Cigna, or Blue Cross.
- Payer rules engine development cost: The baseline engineering investment required to code a central system that updates coverage policies automatically.
- National & Local Compliance: Engineering checks for NCCI edit validation cost alongside automated LCD NCD compliance checking cost to verify regional Medicare rules.
- Coding & Necessity Validation: Software layers dedicated to medical necessity validation cost, ICD-10-CM validation cost, CPT code validation cost, HCPCS validation cost, modifier validation cost, and E&M coding validation cost.
Therefore, this layer filters out clear administrative mistakes before the claim reaches the advanced machine learning models. Let us now examine the cost components of those predictive mathematical layers.
Layer 3 — Machine Learning and NLP Models
The predictive layer uses advanced mathematical models and text-reading algorithms to flag complex, hidden denial risks. Specifically, this is where the software reads unstructured doctor notes to ensure the documented medical care matches the final bill.
- Machine learning denial prevention platform cost: The total investment for data science hours, computing infrastructure, and model training routines.
- Predictive Algorithms: Developing custom XGBoost denial model cost frameworks and gradient boosted trees claims cost structures to analyze risk patterns.
- Data Preparation: The ongoing feature engineering cost claims teams face when transforming raw patient metrics into model inputs.
- NLP clinical text analysis cost: Computational pipelines that use natural language processing to extract clinical context from unstructured medical charts.
- Trust & Transparency: Engineering a confidence scoring system cost and an explainability layer development cost, usually driven by SHAP values implementation cost.
As a result, your team receives highly accurate risk scores accompanied by transparent explanations. However, these predictions are only useful if they route to the correct human reviewer at the right time.
Layer 4 — Workflow and Human Review
The workflow layer delivers the AI’s findings directly into the daily applications used by your hospital’s billing specialists. Consequently, this layer prevents software alerts from being ignored or lost in cluttered email inboxes.
- Human-in-the-loop review cost: Designing interactive validation steps so a human expert can easily approve or reject AI recommendations.
- Alert routing workflow cost: Building intelligent background code to send specific coding errors to coders and clinical errors to nurses.
- Denial prevention dashboard cost: Developing a clean, minimalist web interface for revenue cycle managers to track overall performance.
- Documentation Improvement: Incorporating tools for clinical documentation improvement cost and dedicated CDI automation development cost.
Therefore, a well-designed user layer ensures that automated insights turn into fast, actual claim corrections. Next, we must secure this entire network layer to protect sensitive patient records.
Layer 5 — Security, Compliance, and MLOps
The security and operations layer protects patient privacy and keeps the AI running accurately after it goes live. Because healthcare data is highly regulated, skipping these security layers can lead to massive legal fines.
- HIPAA compliant denial prevention AI cost: The total engineering cost to meet federal healthcare privacy and security regulations (Source: [HHS HIPAA Security Rule, 2024]).
- PHI tokenization cost: Developing encryption software that replaces sensitive patient details with secure, randomized digital tokens.
- Zero-Trust Architecture: Implementing strict identity verification tools, role-based access control cost features, and complete BAA compliance cost documentation.
- Operational Monitoring: Building an audit trail development cost module, an MLOps pipeline cost denial prevention system, and continuous model drift monitoring cost denial prevention tools.
Our security specialists deploy zero-trust architectures that isolate protected health information from the core machine learning models.
Furthermore, we install automated drift monitors that alert your team the moment a payer changes its behavior patterns.
In summary, this final layer transforms a vulnerable data science experiment into a highly secure, enterprise-grade medical application. Without these governance pieces, your system cannot legally handle live patient accounts.
Denial Prevention AI Platform Development Cost Breakdown by Phase
A denial prevention AI platform development cost breakdown should separate discovery, data engineering, rule logic, model development, integrations, workflow, compliance, and maintenance.
This structure helps CFOs compare internal build cost against vendor licensing cost without hiding the expensive parts inside one vague platform estimate.
Strategic Breakdown of Development Milestones
| Phase | Duration | Core Investment | Primary Technical Deliverable |
| Phase 1: Discovery | 2–4 Weeks | $10,000–$25,000 | Operational roadmap and baseline ROI metrics |
| Phase 2: Data Pipeline | 4–6 Weeks | $25,000–$70,000 | Unified, clean denial taxonomy and labeled inputs |
| Phase 3: Rules Engine | 6–8 Weeks | $35,000–$110,000 | Deterministic policy checker with custom edits |
| Phase 4: AI Modeling | 6–10 Weeks | $45,000–$140,000 | XGBoost risk scoring and clinical text NLP |
| Phase 5: Integration | 8–12 Weeks | $50,000–$160,000 | Connected EHR, PMS, and clearinghouse pipelines |
| Phase 6: Workflows | 4–6 Weeks | $35,000–$95,000 | Custom routing queues and performance dashboards |
| Phase 7: Security & Ops | 4–6 Weeks | $35,000–$105,000 | HIPAA-compliant MLOps with automated drift alerts |
We treat auditability as a platform requirement from day one, not a compliance layer added before go-live. Specifically, we program detailed audit trail development cost components that track every single modification made to a claim by both humans and AI.
In summary, this final layer transforms a raw predictive framework into a secure, enterprise-ready healthcare platform. After the build phases are clear, the next decision is where your first dollar should go.
Which Denial Category Should You Automate First?
The first AI investment should target the denial category with the highest preventable revenue value, fastest correction path, cleanest data, and clearest workflow owner.
For most teams, that means starting with eligibility-related, authorization-related, coding-related, or documentation-related denials before attempting broad multi-payer prevention.
1. The Denial Automation Priority Score
Competitor posts explain AI denial management broadly. However, they do not give CFOs and CTOs a prioritization model for deciding where to fund the first build.
Specifically, you can use the following evaluation framework to score each potential project from 1 to 5.
| Criteria | Score 1 | Score 3 | Score 5 |
| Annual preventable denial value | Low | Moderate | High |
| Data availability | Fragmented | Partial | Clean and mapped |
| Correction speed | Slow | Moderate | Same-day correction possible |
| Workflow ownership | Unclear | Shared | Clear owner |
| Payer variability | High | Moderate | Stable enough for rules |
2. Best First Use Cases by Buyer Type
Your organizational structure dictates where automation yields the fastest financial return. For example, a single-specialty clinic faces entirely different operational blockages than a national billing aggregator.
Therefore, matching your specific buyer type to the correct entry module prevents wasted software spending.
| Buyer | Best First Module | Why |
| Hospital network | Authorization and medical necessity prevention | High-dollar denials and complex payer rules |
| Physician group | Eligibility and coding validation | Faster implementation and measurable clean claim gains |
| RCM company | Multi-payer denial risk scoring | Strong SaaS differentiation and portfolio-wide learning |
| Healthcare SaaS platform | Pre-submission claim validation API | Productizable infrastructure and recurring revenue potential |
3. Selecting and Budgeting Your Initial Automation Module
Targeting front-end errors provides a rapid path to production because administrative data streams are highly standardized. Specifically, implementing an eligibility-related denial prevention cost module lets you intercept basic registration mistakes before care occurs.
- Front-End Validation: Automates patient registration checks to deliver immediate, same-day insurance data corrections.
- Utilization Management: An authorization-related denial prevention cost module cross-references scheduled procedures against real-time payer registries.
- Coding Optimization: A coding-related denial prevention cost system uses intelligent scrubbing logic to isolate unique, specialty-specific denial prevention cost variations.
For a deeper breakdown of administrative workflow setup, see our guide on [custom AI denial prevention software cost].
4. Managing Mid-Cycle Complexity and Payer Variability
Evaluating unstructured clinical documentation serves as a highly complex entry point that requires natural language processing.
Specifically, an organization facing steep medical necessity rejections must budget for a comprehensive clinical documentation denial prevention cost pipeline.
- Clinical NLP: Advanced text pipelines parse physician charts to verify that clinical evidence matches the final billing codes.
- Payer Variation: Engineering must map the massive differences found in commercial vs Medicaid vs Medicare denial cost structures.
- Scalable Architecture: Building a flexible multi-payer model cost framework allows the software to handle varying regional compliance constraints.
Intellivon’s data scientists engineer decoupled text analysis models that isolate clinical risk without disrupting daily charting workflows. Therefore, this advanced integration ensures complete billing accuracy while protecting your organization from compliance risks.
In summary, attempting to automate every denial category simultaneously leads to bloated development timelines and integration failure. By using a clear scoring model, you can focus your initial capital on the highest-value module.
What AI Models Are Needed for Denial Prevention?
A production denial prevention platform usually needs supervised machine learning for denial risk scoring, natural language processing for clinical documentation review, rules-based validation for payer policy logic, and explainability models for audit readiness.
LLMs can support summarization, but deterministic claim validation and supervised denial models should control reimbursement-sensitive decisions.
1. Structural Modeling Core Components
| Model Type | Core Technology | Operational Task | Primary Output |
| Supervised ML | XGBoost, Gradient Boosted Trees | Historical claim evaluation | Probability score (0-100%) |
| NLP Pipeline | Named Entity Recognition, Clinical Transformers | Unstructured chart parsing | Documentation deficiency alerts |
| Rules Engine | Deterministic Boolean Logic, Query Filters | Hardcoded compliance matching | Pass/Fail validation edits |
| Explainability | SHAP, Layered Feature Attribution | Algorithmic logic translation | Human-readable warning reasons |
2. Supervised ML for Risk Scoring
Supervised machine learning algorithms process structured data fields from old medical bills to calculate the probability of an insurance rejection.
Specifically, calculating an accurate XGBoost denial model cost requires clean rows of historical client submissions and remittance files.
- Ensemble Power: Designing gradient-boosted tree claims cost models allows your software to analyze deep interactions between provider taxonomies, billing codes, and historical payer responses.
- Carrier Behavioral Insights: Building a dedicated payer behavior modeling cost routine helps uncover invisible shifting trends across private carriers.
- Operational Filtering: Implementing a statistical confidence scoring system cost prevents system alert fatigue by routing only highly certain claim risks to human staff.
Consequently, this lightweight framework allows your financial teams to screen thousands of outbound medical vouchers simultaneously without experiencing application lag.
3. NLP for Clinical Notes and CDI
Natural language processing pipelines convert messy, unorganized doctor notations into structured data fields that the predictive algorithms can easily understand. Therefore, calculating your final NLP clinical text analysis cost depends directly on the volume of patient charts you process daily.
- Text Ingestion: Building localized text extractors that scan clinical documentation improvement cost metrics inside your electronic records system.
- Documentation Automation: Constructing a specialized CDI automation development cost module flags missing procedural details while the patient is still admitted.
- Necessity Checks: Running automated medical necessity validation cost software compares clinical diagnoses against localized contract rules before billing.
This automated system allows your review staff to supplement weak charts before the documentation leaves your corporate network.
4. Rules Engine for Non-Negotiable Billing Logic
A hardcoded rules engine handles deterministic compliance guidelines that are completely rigid and should never be guessed by an AI model. Specifically, budgeting for a claim scrubbing rules engine cost ensures that your system blocks obvious administrative layout errors.
- Federal Alignment: Encoding precise NCCI edit validation cost structures catches incorrect or illegal procedure code combinations instantly.
- Government Rules: Mapping out an LCD NCD compliance checking cost module screens medical items against active state and federal Medicare guidelines.
- Coding Foundations: Embedding strict programmatic checks handles basic CPT code validation cost parameters and complex modifier validation cost tables.
Therefore, you protect your active cash pipeline from disruption when a payer updates their formatting criteria overnight.
5. Explainability Layer for Review and Audit
An explainability layer translates abstract mathematical formulas into clear, plain-English directions that billing personnel can immediately act upon. Consequently, investing in an explainability layer development cost prevents your administrative team from ignoring automated system warnings.
- Mathematical Attribution: Implementing a custom SHAP values implementation cost framework reveals exactly which data fields caused a high risk score.
- Tracking Governance: Creating an immutable audit trail development cost module logs every single automated change made to a claim.
- Human Control: Designing an interactive human-in-the-loop review cost view gives your staff final veto power over all automated corrections.
In summary, a functional denial mitigation network relies on multiple specialized technologies working in perfect synchronization. Hard rules handle formatting, machine learning scores total risk, language algorithms read text, and explainability tools guide humans.
What Integrations Increase Denial Prevention AI Cost?
Integration cost rises when the platform must read claims, clinical notes, eligibility data, authorizations, payer responses, and claim-status events from multiple systems.
The most expensive builds involve Epic, Cerner, clearinghouses, payer APIs, FHIR R4, HL7 CDA, EDI 837, practice management software, and document stores.
1. Cost Realities by Data Source
| System Target | Protocol Baseline | Average Engineering Scope | Cost Velocity Multiplier |
| Enterprise EHR | Epic App Market, Oracle Cerner Ignite | 8–12 Weeks | High (Requires third-party vendor developer fees) |
| Interoperability Layer | HL7 FHIR R4 JSON, Legacy HL7 v2 | 6–8 Weeks | Moderate (Standards are stable but version mappings vary) |
| Clearinghouse Gateways | X12 EDI 837 Real-Time Loop, EDI 835 | 4–6 Weeks | Low (Highly structured text formats) |
| Payer Portals | Custom RESTful APIs, Web Scraping | 6–10 Weeks | High (Payer end-points shift frequently) |
2. EHR and Clinical System Integrations
Enterprise electronic health record connections represent the single largest engineering cost center due to proprietary vendor program requirements.
Specifically, computing your true EHR integration cost denial prevention metric means accounting for specialized credential provisioning and testing sandboxes.
- Vendor Environments: Navigating an Epic integration denial prevention cost pipeline requires your developers to build within strict SMART on FHIR authorization parameters.
- System Customization: Creating a parallel Cerner integration cost denial prevention module requires mapping internal patient identification tables against legacy data stores.
- Modern API Routing: Deploying a global FHIR R4 API integration cost model simplifies web-native access to patient problem lists and care conditions.
- Legacy Conversions: Translating clinical data from old HL7 CDA integration cost structures requires building continuous data pipeline converters.
3. Billing, PMS, and Clearinghouse Integrations
Billing utility integrations bridge the conceptual gap between real-time clinical documentation and outbound electronic billing files.
Therefore, your development timelines depend directly on how smoothly your platform intercepts active financial files before final submission.
- Format Verification: Building an automated EDI 837 validation cost module screens structural transaction files for mandatory data fields before transmission.
- Clearinghouse Pipelines: Negotiating a clearinghouse integration cost setup allows the AI engine to pause problematic vouchers during active processing.
- Administrative Sync: Wiring the software straight into local practice management integration cost frameworks aligns patient charts with active statements.
- Live Claim Status: Programming automated loops captures real-time response data to track active claim-status indicators and incoming payment changes.
For a deeper breakdown of connected claims workflows, see our guide on [AI Healthcare Claims Processing Software Development].
4. Payer API and Portal Workflows
Direct communication connections to insurance carriers eliminate the slow, manual phone calls traditionally required to verify treatment rules.
However, building these direct pipelines remains highly expensive because commercial insurance companies do not use a single, unified communication standard.
- Gateway Connections: Calculating your total payer API integration cost requires accounting for custom security tokens and variable call volumes.
- Utilization Management: Automating a prior authorization checking cost pipeline requires connecting the software directly to dynamic insurer rule portals.
- Insurance Validation: Installing an eligibility verification automation cost module screens active patient enrollment records prior to the medical encounter.
- Custom Risk Frameworks: Creating a payer-specific denial model cost layer isolates shifting rule differences between major commercial carriers.
In summary, integration complexity dictates whether an intelligent financial engine succeeds in a live hospital environment. Connecting to electronic health records provides clinical context, billing loops capture administrative metrics, and payer channels confirm active insurance contracts.
Denial Prevention AI Cost by Platform Type
Healthcare denial prevention AI build cost changes by platform type. A single-provider workflow tool costs less than a multi-payer RCM company platform.
A commercial SaaS product costs the most because it needs multi-tenant security, configurable payer logic, usage analytics, customer onboarding, and scalable model operations.
1. Strategic Budget Allocation by Platform Scope
| Platform Type | Estimated Build Cost | Best Fit | Primary Architecture Driver |
| Rules-only prevention MVP | $75,000–$140,000 | Small group or focused pilot | Deterministic conditional logic filters |
| Internal AI prevention platform | $120,000–$420,000+ | Hospitals, large physician groups | Live EHR and billing system workflows |
| Specialty-specific platform | $180,000–$500,000+ | Oncology, orthopedics, radiology | High-complexity medical documentation NLP |
| Multi-payer RCM platform | $280,000–$650,000+ | RCM firms, billing aggregators | Cross-portfolio historical trend analysis |
| Commercial SaaS platform | $450,000–$750,000+ | Healthcare software vendors | Multi-tenant security and configurable logic |
2. Building Internal and Specialty-Specific Solutions
Hospital networks require an integrated software core that interfaces directly with local electronic health records to score claims before submission.
Specifically, budgeting for an internal system means evaluating your true AI claims denial prevention development cost against the volume of your active providers.
- Custom Frameworks: Designing a machine learning denial prevention platform cost layout requires calculating data engineering fees for historical claim records.
- Clinical Depth: Specializing the platform for high-complexity departments like oncology or orthopedics requires constructing intensive natural language processing lines to read charts.
- Workflow Deployment: Installing native alerts directly into active billing queues eliminates staff friction by keeping users in familiar interfaces.
3. Scaling Commercial SaaS and Multi-Payer Platforms
Commercial software platforms demand an enterprise-grade technical footprint to securely isolate data across thousands of independent corporate tenants.
Therefore, calculating your final denial prevention platform scalability cost requires planning for elastic computing clusters and advanced usage monitoring APIs.
- Multi-Tenant Security: Implementing complete database segregation rules prevents data leaks between competing hospital networks using the same software engine.
- Logical Configurability: Engineering an adaptive rules dashboard lets individual customers modify their specific commercial carrier agreements without changing core source code.
- Iterative Capital Allocation: Implementing a structured phased development cost denial prevention model splits the engineering roadmap into manageable financial chunks.
The financial investment required to build an intelligent validation system depends directly on tenant complexity, data volume, and clinical depth.
Simple pilots run on deterministic code, while enterprise SaaS configurations demand sophisticated cloud infrastructure and multi-tenant security frameworks.
Build Denial Prevention AI Platform With Intellivon
Intellivon designs denial prevention AI platforms that help healthcare organizations detect claim risks before submission, reduce preventable denials, and protect revenue without removing human review from the billing workflow.
Every prediction, recommendation, documentation flag, or coding alert is built to remain explainable, traceable, and reviewable by revenue cycle teams.
1. What Intellivon Helps You Build
Intellivon helps you build denial prevention workflows that identify claim risk before it becomes lost revenue.
The platform can review clinical documentation, coding patterns, payer rules, authorization status, medical necessity evidence, and claim history to flag issues before submission.
Core capabilities can include:
- Denial risk scoring: Detect claims likely to be denied based on payer rules, coding patterns, missing documents, authorization gaps, and historical denial trends.
- Documentation gap detection: Flag missing clinical notes, medical necessity evidence, modifiers, diagnosis support, or payer-specific documentation before billing.
- Coding and authorization alignment: Check whether CPT, ICD-10, modifiers, prior authorization details, and charge capture data match payer requirements.
- Payer rule intelligence: Track payer-specific denial patterns, policy changes, documentation rules, and recurring rejection reasons across service lines.
- Human review workflows: Route high-risk claims to billing teams, coders, clinicians, or RCM managers before submission.
- Denial analytics dashboards: Measure denial rate reduction, preventable denial trends, payer behavior, staff productivity, appeal volume, and revenue impact.
2. When to Build a Denial Prevention AI Platform
A custom denial prevention AI platform makes sense when your organization handles high claim volumes, recurring payer denials, complex specialty billing, prior authorization mismatches, or expensive manual claim reviews.
It is also useful when generic claim scrubbers cannot explain why denials keep happening across payers, locations, providers, service lines, or documentation workflows.
3. What You Get Before Full Development Begins
Before engineering starts, Intellivon helps your team define the denial prevention workflow, payer risk patterns, data sources, compliance requirements, AI boundaries, reviewer permissions, and technical scope. This gives revenue, clinical, and technology leaders a clear roadmap before investing in full development.
The early-stage roadmap can include:
- Claim denial pattern and payer trend review.
- EHR, clearinghouse, billing, and RCM integration planning.
- AI risk scoring and documentation review architecture.
- Human approval, exception routing, and audit workflow design.
- MVP scope, cost range, timeline, and rollout roadmap.
4. Why This Matters
AI can reduce denials only when it improves claim quality before submission. A weak implementation may score claims quickly, but still miss documentation, authorization mismatches, payer-specific policy gaps, or coding issues that lead to preventable denials.
If your organization is evaluating denial prevention AI platform development, start with a workflow and denial-readiness review before choosing models or vendors.
Talk to Intellivon to scope your claim risk architecture, payer rule engine, EHR integration requirements, human review workflows, compliance safeguards, analytics dashboard, development cost, and rollout roadmap before committing to a full build.
Conclusion
Denial prevention AI development works best when healthcare teams treat it as revenue-cycle infrastructure, not a standalone prediction model. The goal is to connect claims, payer rules, documentation, authorization data, compliance controls, and review workflows before submission.
Start with the highest-value preventable denial category, prove ROI, then expand carefully. This phased approach improves claim quality, reduces avoidable rework, and protects revenue without adding another disconnected operational layer for teams today.
Things To Know About Denial Prevention AI Development
Q1. How much does denial prevention AI cost to build?
A1. A custom denial prevention AI platform usually costs $120,000–$420,000+ for an internal production build. However, a focused MVP can start near $75,000, while multi-payer SaaS products can exceed $750,000. Costs rise when teams add EHR integration, payer-specific rules, NLP, HIPAA controls, audit trails, and MLOps during rollout and maintenance.
Q2. How long does denial prevention AI platform development take?
A2. A focused denial prevention MVP usually takes 12–16 weeks when the data sources are clear. However, production platforms with EHR integration, payer rules, AI scoring, HIPAA controls, and dashboards usually need 5–9 months. Multi-payer SaaS builds often take 9–15 months because tenant controls, onboarding, and model governance add work.
Q3. Can a HIPAA-compliant denial prevention AI cost less if we avoid clinical notes?
A3. Yes. Avoiding clinical notes can reduce early build cost because the platform handles less unstructured PHI and needs fewer NLP safeguards. As a result, a claims-only MVP can start with eligibility, authorization, coding, and payer rules first. Clinical documentation intelligence can be added later when ROI is clearer.
Q4. Can denial prevention AI stop pre-authorized claims from being denied?
A4. It can reduce this risk, but it cannot remove it completely. Therefore, the platform must compare authorization records, payer policy, CPT codes, diagnosis codes, service dates, and documentation before submission. It should flag mismatches where approval exists, but the final claim may still fail payer adjudication rules later.
Q5. What is the hidden cost competitors rarely explain?
A5. The hidden cost is payer rule decay management. Payer edits, documentation requirements, and denial behavior change often. So, teams need rule versioning, model drift monitoring, retraining, and policy refresh workflows. Without these controls, denial rates can rise again after the first pilot, even when early results look strong.
To Sum Up
- Denial prevention AI costs more than denial prediction because it must correct claim risk before submission, not only forecast it.
- The payer rules engine is often the most underestimated cost layer because NCCI, LCD/NCD, payer policy, and specialty edits require ongoing maintenance.
- A claims-only MVP can reduce early cost by avoiding clinical NLP, but it will not solve medical necessity or documentation-driven denials.
- The best first module is not always the most advanced AI model. It is the denial category with the highest preventable value and fastest correction path.
- Build-vs-buy should be decided by data ownership, payer specificity, integration depth, and long-term total cost of ownership.



