

Key Takeaways:
-
Building an AKASA-style platform requires EHR ingestion, FHIR R4 APIs, and healthcare-specific LLMs.
-
Clinical NLP, confidence scoring, and human-in-the-loop workflows are core production requirements.
-
HIPAA controls, audit trails, and MLOps monitoring ensure long-term accuracy and compliance readiness.
-
A focused MVP starts at $180,000, while enterprise platforms reach $350,000 and above.
-
How Intellivon builds this: scoped RCM workflows first, then expanding into autonomous coding, authorization, denial prevention, and appeals.
AKASA automated their entire healthcare revenue cycle system by replacing rules-based billing logic with LLMs trained on their hospital data. Those models can read clinical documentation, navigate payer portals, and route exceptions to human review autonomously. As a result, the platform delivered a 13% drop in A/R days, 86% efficiency gains, and $30M in ROI.
Teams taking inspiration from this incredible success and building in this space usually end up studying the wrong layer. They analyze AKASA’s workflow steps, automation triggers, and portal navigation, and then try to replicate what is visible on the surface. What determines production performance sits underneath, which includes model selection, client-specific training architecture, and expert-in-the-loop design.
Building a platform like AKASA means making those foundational decisions deliberately. That includes LLM selection by workflow type, client-specific fine-tuning, and autonomous agent design across prior authorization, coding, and claims. Each of those decisions also carries a HIPAA compliance requirement at the inference layer.
At Intellivon, we build these platforms where model selection, training design, and compliance architecture are decided together from day one. This blog covers what the build requires, which includes clarity around LLM architecture, EHR integration, human-in-the-loop design, HIPAA controls, and cost by phase.

What Is AKASA, and Why Are Founders Building Platforms Like It?
AKASA is an AI software platform that takes over the heavy paperwork in hospital billing. Instead of having workers manually type codes, check insurance rules, or look up claim statuses, specialized AI models do the work instantly by reading doctor notes and connecting directly to hospital database systems.
When an insurance rule changes or a claim is too complicated, the platform hands the file to a human billing expert. The AI watches how the human fixes the issue and learns how to do it automatically next time.
1. What AKASA Does
The platform targets the manual, repetitive tasks that happen after a patient sees a doctor.
- Automates medical coding: Reads clinical charts and suggests the right billing codes.
- Tracks insurance approvals: Logs into payer portals to check prior authorization status.
- Follows up on claims: Monitors outstanding insurance balances to see if claims are approved or denied.
- Optimizes documentation: Highlights missing medical data before files are sent to insurance companies.
2. Why It Matters in Healthcare Revenue Cycle Management
Hospital billing departments are losing margins to administrative overhead and complex insurance rules.
- Reduces billing errors: AI stops simple human mistakes that cause immediate claim rejections.
- Lowers cost per claim: Software runs 24/7 without the overhead costs of large manual billing teams.
- Speeds up cash flow: Speeds up the time it takes to get paid by shrinking days in accounts receivable.
- Prevents staffing shortages: Fills operational gaps when hospitals cannot find certified medical coders.
3. Generic RPA vs. AKASA-Style AI Automation
Traditional robotic process automation (RPA) relies on rigid, step-by-step rules to click buttons and paste text. If an insurance website moves a button even one inch to the left, the RPA bot breaks and stops working.
An AKASA-style platform uses computer vision and neural networks to understand the screen layout, meaning it adapts to visual changes just like a human eye.
Generic RPA vs AKASA AI Automation
| Automation Feature | Generic RPA Platforms | AKASA-Style AI Platforms |
| Handling Web Changes | Breaks when UI layouts or portal structures change | Uses computer vision to adapt to interface shifts |
| Reading Free Text | Limited to structured data fields and fixed forms | Processes unstructured notes via generative AI for RCM |
| Fixing Errors | Flags errors for manual IT scripting updates | Routes exceptions to human experts and learns from them |
| Core Technology | Linear, rule-based macros and screen scraping | Large language models and intelligent workflow orchestration |
Traditional RPA requires constant maintenance, whereas advanced AI platforms learn from mistakes and become more stable over time.
4. Specialized GenAI for Clinical and Financial Datasets
Generic AI models cannot handle medical billing because they do not understand complex clinical context or insurance policies.
- Domain-specific training: Models must be trained directly on medical textbooks, doctor narratives, and insurance contracts.
- Accurate code extraction: AI reads unstructured doctor notes to extract precise diagnostic definitions.
- Payer rule matching: The system cross-references medical records with specific insurance rules to ensure coverage.
- Explainable suggestions: Software provides clear reasons for each code suggestion so humans can audit the logic.
5. What To Build if You Want a Platform Like AKASA?
Building a competitor to AKASA means creating an intelligent workflow center, not just a set of simple web scrapers.
- An EHR integration layer: Secure pipelines that read and write data directly into hospital software like Epic and Cerner.
- An AI agent orchestration engine: Multiple specialized microservices that handle different parts of the billing cycle.
- A human-in-the-loop workspace: A clean dashboard where human billers can review claims when the AI is uncertain.
- An MLOps feedback pipeline: Software that tracks human corrections and uses that data to retrain the AI models automatically.
If the model processes a claim with low confidence, it transfers the file to a human specialist, turning every manual fix into training data for the next version of your software.
Why the Market Wants AKASA-Style Revenue Cycle Automation
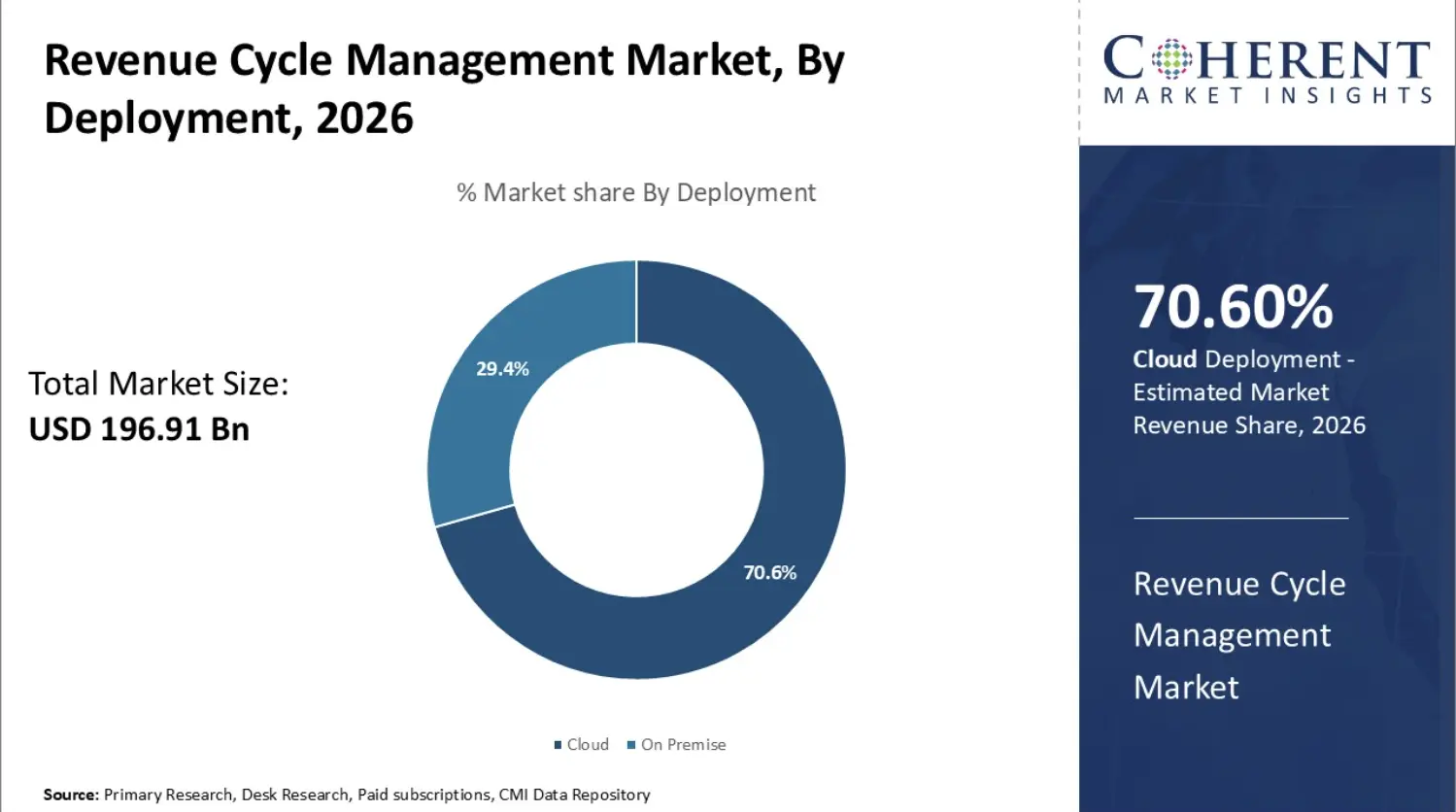
The global revenue cycle management market size is estimated to be valued at 196.91 billion dollars in 2026. Industry data projects this market will reach 440.78 billion dollars by 2033. This growth trajectory represents a compound annual growth rate of 12.2% across the seven-year forecasting period.
Healthcare systems are actively looking for automation that natively integrates with their existing electronic health records rather than disjointed software platforms that demand secondary manual reviews.
Building an autonomous billing platform capitalizes on this urgent demand by solving structural staffing constraints and improving first-pass collection metrics.
1. Manual Workloads and the Healthcare Staffing Crisis
Administrative expenses inside the United States healthcare infrastructure have climbed significantly, highlighting the massive labor-related cost of manual claims processing.
RCM departments are facing severe operational bottlenecks due to widespread labor scarcity.
- Severe personnel gaps: Industry data estimates a massive shortage of healthcare workers, forcing billing teams to operate far below capacity.
- Aggressive staff turnover: Hospital-specific turnover rates continue to challenge human resource departments, with overall healthcare industry turnover averaging around 22.7%.
- Sustained operational lag: Heavy manual pipelines mean employees spend excessive time on repetitive portal lookups rather than pursuing high-value appeals.
2. The Prior Authorization Bottleneck and Rising Payer Complexity
Insurance company rules constantly alter, leading to a massive administrative strain on providers seeking medical necessity approvals before treatments occur.
- Drained medical hours: Providers spend significant amounts of time every single week, often logging over 13 hours, working through the details of millions of prior authorization requests.
- Unnecessary coverage denials: A vast majority of initial prior authorization denials are completely overturned on appeal, revealing significant systemic inefficiencies.
- Compounded financial risk: Brittle payer portals mean manual billing teams struggle to intercept documentation omissions, causing immediate cash flow disruptions.
3. Managing the Claim Denial Epidemic
Initial claim denial rates remain high, changing financial management into an explicit margin-protection function.
- Expensive appeals management: Enterprise hospital networks spend billions of dollars trying to overturn rejected claims.
- Persistent cash degradation: High rejection volumes degrade critical operational metrics like total days in accounts receivable.
- Leakage from human error: Up to 30% of all healthcare spending qualifies as administrative waste or operational inefficiency, which includes expensive manual entry billing errors.
4. Regulatory Catalyst: The CMS Interoperability Mandates
The Centers for Medicare and Medicaid Services established the CMS-0057-F Final Rule, establishing hard implementation rules that mandate electronic healthcare workflows.
- January 1, 2027 API deadline: Impacted payers must deploy production-grade Fast Healthcare Interoperability Resources (FHIR) APIs for patient access, provider data exchange, and prior authorizations. (Source: PilotFish, 2026).
- Accelerated processing timelines: Regulatory updates mandate faster prior authorization turnarounds alongside detailed annual metric reporting.
- Product development windows: These upcoming federal deadlines create an immediate product market for healthcare SaaS startups that build native FHIR-compliant automation layers.
[For a deeper breakdown of tracking shifting healthcare metrics, see our guide on Healthcare Data Interoperability Best Practices.]
5. Why the Software Category Exists Now
This product market exists today because traditional robotic process automation fails under the structural complexity of modern healthcare reimbursement networks. Legitimate market value requires a self-healing architecture that moves past rigid scripts to execute straight-through claim processing.
How Does AKASA Make Money? (Revenue and Business Model)
AKASA monetizes its enterprise revenue cycle automation platform through a hybrid B2B pricing framework that scales with institutional data volume and operational complexity.
Because healthcare systems require predictable expense models, platforms in this space combine steady base subscription access with performance-linked or volume-based escalators.
AKASA currently deploys its technology across more than 650 hospitals and 6,500 outpatient facilities nationwide, securing major enterprise accounts including the Cleveland Clinic, Duke University Health System, and Johns Hopkins Medicine.
1. Core Monetization Streams for Revenue Cycle Software
Enterprise AI vendors avoid flat public pricing because software implementation depth is strictly dependent on hospital size, net patient revenue (NPR), and specific electronic health record architectures.
Core Monetization Streams
| Revenue Stream | How It Works | Why It Matters for Builders |
| Enterprise SaaS Fees | Health systems pay annual recurring base fees to access the workflow orchestrator. | Establishes predictable annual recurring revenue (ARR) to fund continuous development. |
| Module-Based Pricing | Separate workflows like prior authorization and medical coding are priced as standalone add-ons. | Enables a land-and-expand sales model to lower initial hospital onboarding friction. |
| Implementation Fees | One-time upfront charges cover custom FHIR API and native EHR integration engineering. | Offsets the initial cost of engineering custom pipelines for legacy hospital software. |
| Usage-Based Automation | Fees scale directly with the volume of claims processed or tasks executed by AI agents. | Aligns software pricing with tangible hospital transaction volume. |
| Expert-in-Loop Services | Hybrid billing services bundle human exception handling directly with the software license. | Overcomes trust barriers by guaranteeing operational safety for high-risk billing tasks. |
2. Structuring Pricing Variables for Enterprise Health Systems
A variable monetization architecture allows the base software license to scale up as the health system derives measurable financial value from the platform.
- Volume-based scaling: Annual platform licensing scales alongside total annual claim submissions or patient accounting throughput, ensuring small community hospitals and major networks are billed proportionally.
- Performance-aligned modules: Back-end features like denial recovery frequently use a contingency fee model where the software vendor captures a direct percentage of additional revenue successfully recovered.
- Transactional event fees: Mid-cycle tools like prior authorization automation charge a flat fee per cleared transaction, turning software usage into a predictable operational cost.
3. How a Startup Makes Money When Building an AKASA Alternative
Startups entering the revenue cycle automation market should structure their initial contracts around volume-based subscription tiers, deriving roughly 85% of total revenue from recurring software access.
Remaining revenues should come from one-time professional service implementation fees to cover custom EHR data mapping.
This architectural layout allows product teams to turn specific AI workflow modules on or off remotely, giving you complete flexibility to adapt your monetization model to match customer contract demands.
What Product Modules Does AKASA Offer?
AKASA is a collection of specific software tools that handle different parts of hospital billing. This modular setup gives engineering teams a clear plan for how to build a competing software platform.
1. Breaking Down the Product Modules
The platform splits its features into different tools so hospitals can buy only what they need.
- Prebill Optimization Suite: This tool connects medical coding and clinical documentation teams. It catches paperwork errors before the hospital sends the bill to the insurance company.
- Coding Optimizer: This module reads patient charts and suggests accurate medical codes. It highlights quotes from the doctor’s notes to show exactly why it suggested a specific code.
- CDI Optimizer: A dedicated clinical documentation improvement assistant. It finds missing information in a patient record and asks the doctor to clarify details before billing.
- AI Advisor: A research tool built for billing teams. Workers can type plain-English questions to look up complex insurance rules or find old billing documents quickly.
- Auth Status: This module logs into insurance portals automatically to check on pending prior authorization requests, which cuts down on phone calls.
- Claim Status: This tool automatically checks if submitted claims are approved, denied, or stuck. It organizes the hospital work queue so humans only work on broken claims.
- Claim Attachment Automation: This module automatically finds supporting medical records inside the EHR and uploads them to insurance portals to resolve complex claim denials.
AKASA Modules
| AKASA-Style Module | Workflow It Supports | Build Complexity |
| Prebill Optimization | Coding, CDI, and billing data validation | High |
| Coding Optimizer | ICD-10-CM and CPT code suggestions | High |
| CDI Optimizer | Tracking gaps in medical record details | High |
| AI Advisor | Search and text retrieval for internal billing rules | Medium |
| Auth Status | Checking insurance portals for prior approvals | Medium |
| Claim Status | Checking claim approval logs and sorting worker tasks | Medium |
| Claim Attachment Automation | Gathering medical PDFs and uploading them to portals | High |
2. What Your Minimum Viable Product (MVP) Should Include
If you are a startup trying to launch an alternative platform, do not try to build every single module at the same time. Start with a focused product that solves one clear administrative bottleneck.
- Build Claim Status and Auth Status first: These modules are easier to develop because they focus on portal data entry and screen checking. They provide immediate financial value to hospitals by saving hours of manual labor.
Akasa - Add Coding and CDI modules later: These tools require advanced clinical AI training pipelines and deeper integrations. Saving them for version two keeps your initial launch timeline realistic.
Our development teams at Intellivon prefer this phased assembly style. We build the core data pipelines first, allowing you to deploy working portal automation tools while your engineering team refines the complex language models needed for advanced medical coding.
What Makes AKASA Different From Traditional RCM Software?
Traditional billing software helps hospital teams track claims manually through static dashboards and basic work queues.
An AKASA-style platform goes much further by using advanced machine learning models to read clinical charts, handle complex portal communication, and automate entire administrative workflows.
Instead of just organizing the manual work left for human billers, an AI-native system executes the tasks autonomously and presents clear, evidence-based recommendations when human review is needed.
Breaking Down the Architecture Differences
To build a truly competitive product, you must understand why legacy revenue cycle software cannot match the capabilities of an AI-native automation system.
Building another static database wrapper with a shiny user interface will not solve the operational issues hospitals face today.
Architecture Difference Breakdown
| Operational Feature | Traditional RCM Software | AKASA-Style AI Platforms |
| Workflow Routing | Uses rigid, hard-coded rules to push tasks into manual human employee queues. | Employs intelligent workflow orchestration to automate tasks or route them to clinical AI agents. |
| Data Interpretation | Requires structured data entry fields and manual keyword searching to process files. | Uses a healthcare-specific LLM to comprehend unstructured clinical narratives. |
| Payer Connections | Relies on slow, basic electronic data interchange transfers or brittle scraping macros. | Deploys autonomous payer portal automation that adapts dynamically to website changes. |
| Decision Logic | Operates on static, checkbox-based logic paths that require constant manual IT adjustments. | Offers explainable AI recommendations backed by clear audit trails and clinical evidence. |
This ensures your software delivers direct administrative relief, moving past simple data visualization to execute actual billing workflows.
Core Workflows an AKASA-Style AI Platform Must Automate
An AKASA-style AI platform must automate the specific billing workflows where clinical evidence, insurance guidelines, coding logic, and manual data entry create the most operational friction. Instead of attempting to replace entire billing departments at once, developers should build specialized automation modules that target high-volume, error-prone tasks.
Automating these touchpoints directly improves first-pass resolution rates and lowers the overall cost per claim for hospital networks.
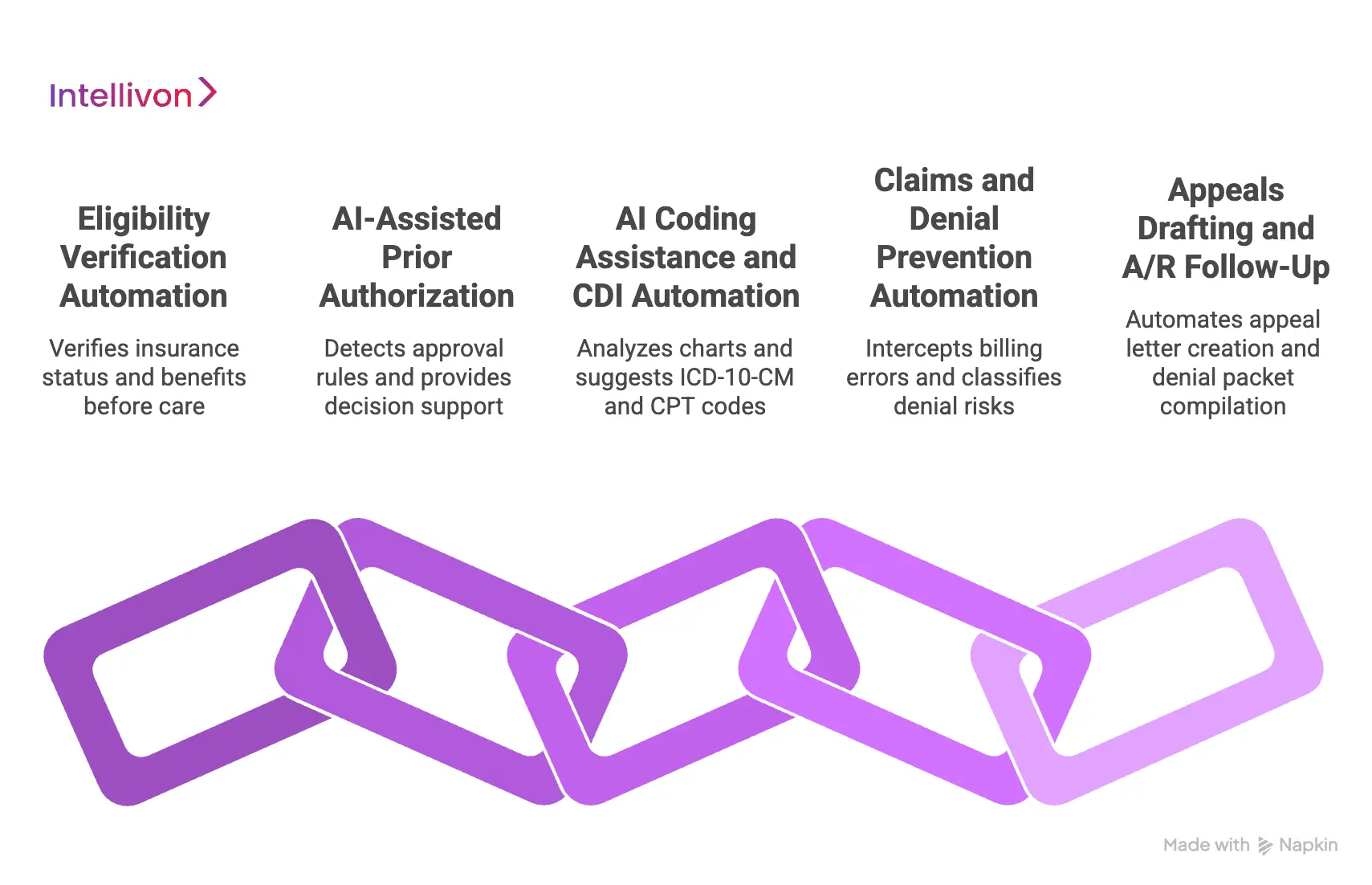
1. Eligibility Verification Automation
This module verifies insurance active status, specific plan benefits, coverage effective dates, and real-time patient financial responsibilities before a patient receives medical care.
- Technical execution: The software queries insurance databases using secure FHIR R4 APIs and standard electronic data interchange (EDI) transactions to extract structured benefit summaries.
- Failure consequence: Skipping automated verification causes hospitals to submit claims under inactive policies, which triggers immediate eligibility denials and extends collection timelines.
- Intellivon approach: We build multi-threaded API connectors that cross-reference insurance responses against hospital registration records. When data conflicts occur, the platform routes the claim to a human registrar while logging the conflict into the MLOps training loop.
2. AI-Assisted Prior Authorization
This system automatically detects insurance approval rules at the moment a doctor places a medical order, providing direct prior authorization decision support.
- Technical execution: The AI parses unstructured medical necessity documentation to pull clinical evidence, and then submits it directly via automated payer portal automation scripts when direct APIs are unavailable.
- Failure consequence: Manual authorization management leads to severe treatment delays, scheduling backlogs, and costly write-offs for unauthorized medical services.
- Intellivon approach: Our engineering team designs these modules to align with upcoming federal rules, ensuring your platform is fully compatible with the mandatory electronic workflow mandates going into effect on January 1, 2027.
3. AI Coding Assistance and CDI Automation
This engine reads clinical charts to handle complex ICD-10-CM automation and provide precise CPT code suggestions for billing departments.
- Technical execution: Natural language processing models analyze physician notes, validate code combinations against NCCI edits automation rules, and drive continuous clinical documentation improvement workflows.
- Failure consequence: Inaccurate manual coding leads to upcoding compliance audits or downcoding revenue leakage, both of which damage hospital margins.
- Intellivon approach: We implement a permanent coding audit trail within the database layer. This architecture saves the exact clinical text snippets used by the AI to make a recommendation, giving hospital compliance officers complete transparency.
4. Claims and Denial Prevention Automation
This module uses an intelligent payer rules engine and automated charge capture automation to intercept billing errors before files leave the facility.
- Technical execution: The system checks every claim against historical insurance denial records, automatically classifying denial root cause risks to fix issues instantly.
- Failure consequence: Operating without proactive checks results in high baseline rejection rates, forcing staff into a reactive cycle of chasing old revenue.
- Intellivon approach: We build predictive scoring systems that replicate the performance of enterprise networks. For context, similar implementations have helped community health networks successfully reduce prior authorization denials by 22% and non-covered service denials by 18%.
5. Appeals Drafting and A/R Follow-Up
This back-end tool automates the creation of comprehensive appeal letter documents and compiles required medical history attachments when claims are rejected.
- Technical execution: Generative AI models draft personalized appeal arguments based on specific insurance contract language and bundle them into digital denial packets.
- Failure consequence: Unappealed claims turn into permanent bad debt write-offs, while slow follow-up cycles increase overall days in AR metrics.
- Intellivon approach: We enforce a strict human-in-the-loop review step for all AI-generated text. The software creates the complete appeal packet automatically, but requires a certified biller to click an approval button before electronic submission.
Once your core workflow automation scope is fully defined, your engineering focus must shift to creating a secure backend architecture that safely isolates data processing from the AI decision layers.
Architecture for a Custom AI RCM Automation Platform
A custom AI RCM automation platform should use a layered architecture that separates data ingestion, workflow orchestration, AI inference, deterministic rules, human review, analytics, and compliance logging.
This structural division keeps autonomous decisions completely traceable while allowing the platform to scale fluidly across hospitals, medical specialties, insurance payers, and active software modules.
For context, industry research highlights that only a small portion of medical prior authorizations are fully electronic through standard X12 278 networks.
Engineering Your Software Infrastructure Layers
To build an enterprise-grade platform, your engineering team must map out clear data processing stages.
Each tier should focus on a specific operational goal to ensure the background system remains stable as data loads scale.
Architecture Layer
| Platform Layer | Core System Responsibilities | Primary Technology Stack Components |
| Data Ingestion | Extracts inbound text from electronic health records, diagnostic PDFs, insurance portal pages, historical claim logs, and electronic remittance files. | Apache Kafka pipelines, AWS Textract OCR engines, secure SFTP servers, Webhook listeners |
| Interoperability | Manages direct structural connections with outside software utilities and financial clearinghouses using legacy and modern formatting structures. | HL7 integration engines, FHIR R4 APIs, X12 EDI parsers (270/271, 276/277, 278, 837, 835) |
| Normalization | Matches patient identities across systems, classifies medical encounters, normalizes text definitions, and maps terms to standard payer taxonomies. | Python data processing suites, PostgreSQL tables, Elasticsearch engines, and custom semantic mappers |
| Workflow Orchestration | Controls dynamic data queue routing, monitors system state machines, tracks customer SLA performance limits, and manages technical exceptions. | Apache Airflow, Temporal.io orchestration engines, Redis message queues, RabbitMQ clusters |
| AI Decisioning | Runs clinical natural language processing, orchestrates healthcare-specific LLMs, tracks confidence scoring, and generates explainable AI recommendations. | PyTorch frameworks, Hugging Face transformers, NVIDIA Triton inference servers, custom scoring microservices |
| Rules and Policy | Validates code configurations against an active payer rules engine, manages NCCI edits automation, and updates medical necessity logic files. | Drools rules engine, JSON schema verification engines, Git-based configuration versioning systems |
| Human Review | Powering the human-in-the-loop RCM dashboard workspace, handling task acceptance and rejection queues, and maintaining the coding audit trail. | React frontend views, Node.js backend services, secure GraphQL query layers, JWT verification modules |
| Governance and Analytics | Operates the central MLOps pipeline, runs model drift detection, and compiles operational revenue cycle KPIs like straight-through processing rates. | Prometheus tracking tools, Grafana monitoring views, MLflow model registries, Snowflake analytics warehouses |
By enforcing this layered structure, your development team can safely isolate experimental machine learning components from your mission-critical integration adapters. This architecture ensures that a model update or an unexpected web layout shift never brings down your core medical data pipelines.
The underlying software architecture should focus on making billing automation safe before it focuses on making processing fast.
AI Model Stack Needed to Develop an AI Platform Like AKASA
To develop an AI platform like AKASA, your machine learning stack must combine healthcare-specific LLMs, clinical NLP, document extraction models, and token-weighting algorithms. No single baseline model can safely manage the extreme text lengths and varied formats found in hospital billing pipelines.
Instead, you need a collection of specialized models working alongside deterministic validation systems. This layout ensures that your software can process complex doctor narratives while maintaining absolute financial accuracy.
1. Clinical NLP and Document Understanding
The bottom layer of your artificial intelligence stack must convert messy, unstructured hospital data into clean, structured digital information.
- Targeted clinical extraction: Specialized named-entity recognition models pull specific text items from patient records, including exact diagnostic terms, medications, treatments, lab results, and provider notes.
- Processing unstructured notes: This layer uses advanced computer vision and text parsing to read scanned documentation, converting free-form text blocks into structured data inputs for your systems.
- Powering mid-cycle workflows: This precise data extraction serves as the primary technical fuel for your clinical documentation improvement (CDI) automation and medical necessity workflows.
2. Healthcare-Specific LLM Layer
Generic foundational models cannot manage medical billing because they lack exposure to complex billing definitions and specific insurance rules.
- Deep context modeling: Advanced billing systems utilize specialized models trained directly on millions of anonymized clinical records and financial data files to comprehend specific hospital contexts.
- Overcoming context window limits: Modern production pipelines use architectures like Attention-based Multiple Instance Learning (MIL) to split massive 50,000-word clinical records into small chunks for your core models.
- Automating communication tasks: These customized language layers analyze clinical text segments to draft comprehensive appeal letters, explain complex code selections, and compile detailed clinical evidence packets for insurance companies.
3. Task-Specific AI Models
Besides large language layers, you need a group of smaller, highly optimized models designed to calculate specific operational probabilities.
- Predictive risk scoring: Dedicated classification networks analyze completed claims before submission to generate an accurate denial risk score.
- Detecting authorization rules: Light machine learning classifiers read scheduling fields to determine prior authorization requirement thresholds across varied insurance plans.
- Tracking financial leakage: Background algorithms scan itemized hospital logs alongside final bills to instantly highlight charge capture gaps and missing billable items.
4. Deterministic Rules Engine
Do not use generative AI models to handle fixed, mathematical billing compliance steps. LLMs are probabilistic engines that can hallucinate, making them fundamentally unsafe for calculating strict financial rules or legal edits.
- Enforcing absolute boundaries: Hard-coded validation engines manage fixed data tasks like checking NCCI edits, automation rules, confirming insurance enrollment dates, and tracking filing deadlines.
- Structuring system logic: The rules engine acts as an unyielding boundary layer, blocking any claim code suggestion that fails basic national regulatory billing requirements.
5. Feedback and Fine-Tuning Loop
Your machine learning infrastructure must include a structured MLOps pipeline to manage model drift detection and handle constant updates to insurance guidelines.
- Recording human interactions: The platform logs every single click, text alteration, and code change completed by human specialists in your human-in-the-loop workspace.
- Refining model weights: These human validation signals act as direct supervised training data, running through automated fine-tuning loops to retrain your models on complex edge cases.
- Protecting processing stability: This continuous learning infrastructure ensures your platform adapts dynamically to shifting interface rules, dropping software maintenance costs by up to 60%.
The underlying model stack only functions successfully when your integration layers deliver completely clean, real-time healthcare data from hospital networks.
EHR, Payer, Clearinghouse, and Portal Integrations Required
A healthcare AI workflow automation platform needs bi-directional integrations across electronic health records, insurance clearinghouses, payer networks, and clinical analytics databases. Without these permanent data channels, an artificial intelligence engine becomes an isolated dashboard that merely suggests billing tasks rather than completing them safely.
Building an operational system requires establishing read and write permissions across your customers’ entire software environment. This setup allows your software agents to pull clinical documentation and submit polished claims autonomously.
1. EHR Workflow Integration
Your platform must hook directly into core hospital electronic health record systems to read doctor notes and update billing files.
- Supported platforms: Build connection endpoints for market-leading systems, including Epic, Oracle Health (Cerner), Meditech, athenahealth, eClinicalWorks, and NextGen.
- Operational functionality: Your software agents need backend access to read physician narratives and write real-time status alerts back into the native billing queues.
2. FHIR and HL7 Data Streams
Using standard medical communication protocols allows your platform to receive real-time clinical events as they happen across the hospital network.
- Core data messaging: Implement secure HL7 data feeds (ADT for patient admissions, ORM for orders, and ORU for lab results) to track patient movement.
- Modern API frameworks: Utilize FHIR R4 APIs and SMART on FHIR protocols to render your dashboard interface directly within the doctor’s existing workspace, while Epic MyChart integrations can provide patient-facing visibility for authorization updates.
3. Payer Network and Prior Authorization Access Points
Your system must connect directly with insurance companies to submit medical necessity evidence and check approval statuses.
- Federal mandate alignment: To ensure long-term regulatory compliance, you must align your prior authorization models with the upcoming federal data exchange guidelines.
- Protocol stack requirements: This alignment requires incorporating HL7 Da Vinci implementation guides, specifically Coverage Requirements Discovery (CRD), Documentation Templates and Rules (DTR), and Prior Authorization Support (PAS).
4. Claims Handling and Electronic Payment Posting
Your back-end system needs to communicate directly with medical clearinghouses to track where bills stand and post financial updates.
- Transaction processing: Establish robust interfaces with financial clearinghouses to manage outbound X12 837 claim submissions and parse inbound X12 835 electronic remittance files.
- Automated remediation: Your background services must process these clearinghouse status files instantly to automate ledger updates and trigger immediate denial remediation scripts.
5. Enterprise Analytics and Business Intelligence Layers
To help hospital leaders make business decisions, your software must pipe its processing data into central data warehouses.
- Data storage hubs: Route all processed financial data and processing events into scalable storage environments like Snowflake, Google BigQuery, or Amazon Redshift.
- Reporting tools: This centralized storage structure allows you to build real-time dashboard views inside tools like Power BI, Tableau, or Looker to display critical client revenue cycle KPIs.
Once these foundational integration points are fully established, your product rollout must move through controlled development milestones rather than attempting a broad, all-at-once launch.
How to Build a Platform Like AKASA Step by Step
Building an AI-native revenue cycle platform requires a disciplined engineering roadmap that values operational stability over theoretical model accuracy. Instead of building every product module simultaneously, developers must follow a staged assembly strategy.
Each development milestone must establish clear programmatic data boundaries to keep medical data secure and platform logic auditable.
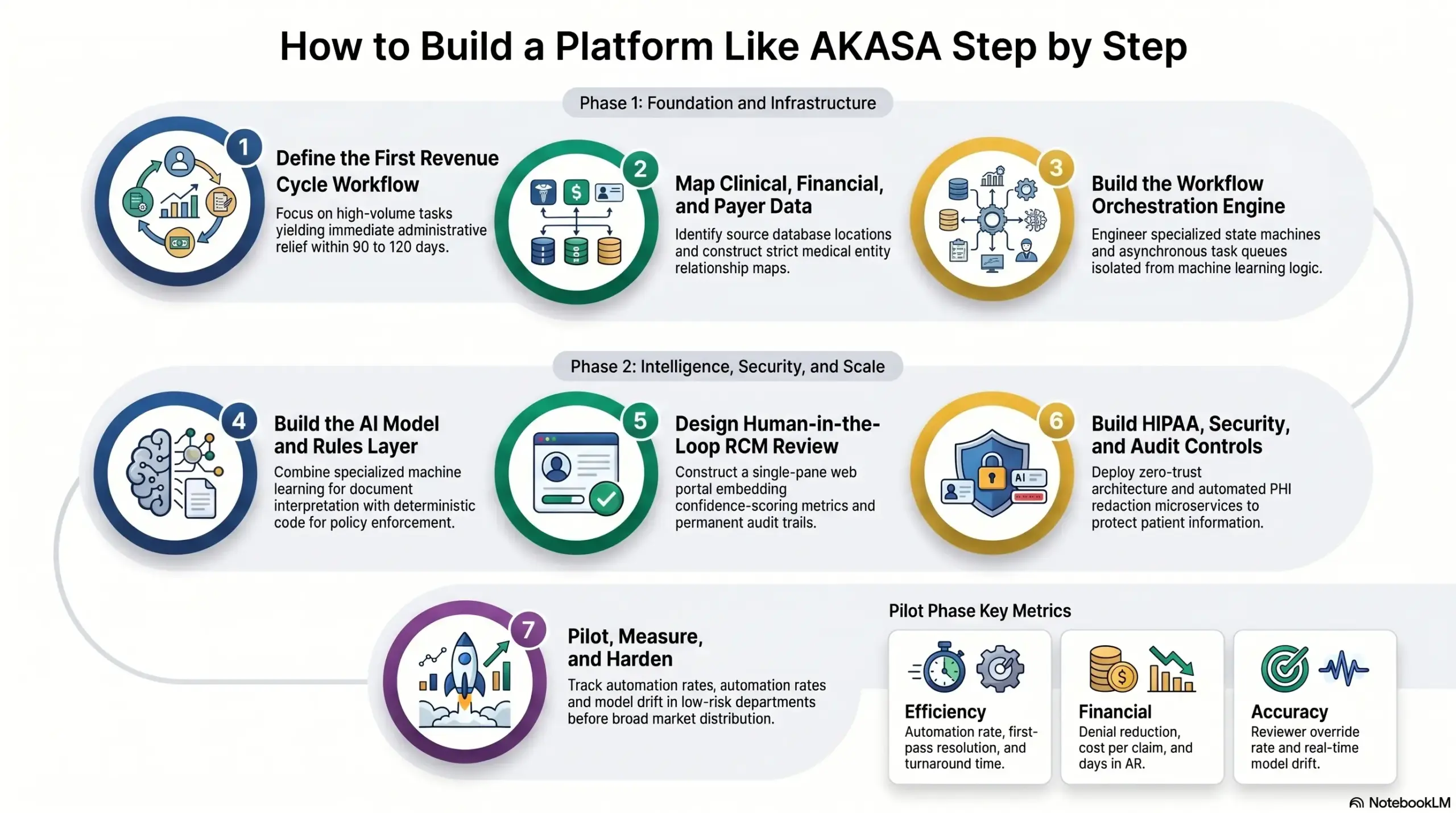
Step 1 — Define the First Revenue Cycle Workflow to Own
Start by choosing one revenue cycle workflow where automation can create measurable value within 90 to 120 days. Additionally, the best starting points are eligibility verification, prior authorization, coding assistance, denial prevention, claim status, or appeals.
- Technical execution required: Engineers must document the current manual workflow steps, define specific user access permissions, and script precise payer-by-payer interaction variations. This preparation requires translating manual billing click-paths into a programmatic event map with tracked performance baselines.
- Consequences of failure: Skipping this focused scoping phase results in an overly broad product surface where your core machine learning pipelines lack clear task boundaries. Consequently, your MVP fails to deliver verifiable financial returns, causing hospital operations leaders to reject the platform.
- The Intellivon methodology: We initiate product engineering with an exhaustive workflow discovery, revenue leakage analysis, and automation scoring framework before writing backend infrastructure code. This validation step isolates high-volume billing tasks that yield immediate administrative relief.
After your first workflow scope is locked down, your development team must map out the underlying medical, financial, and payer data pipelines.
Step 2 — Map Clinical, Financial, and Payer Data Inputs
The platform needs a complete data map before any AI model is trained. At the same time, for RCM automation, the input layer usually includes EHR notes, orders, diagnoses, CPT and ICD-10-CM codes, eligibility files, payer policies, claims, remittance data, denial history, and staff action logs.
- Technical execution required: Developers must identify all source database locations, build an enterprise-grade medical entity relationship map, and construct strict data minimization filters. This stage requires building background document classifiers and normalizers to align raw hospital texts with standard insurance plan tax tables.
- Consequences of failure: Operating without a structured data map forces your models to generate financial recommendations from incomplete clinical datasets. This deficiency causes predictive denial scores to become highly unreliable, while making it impossible to generate clear audit trails for hospital compliance officers.
- The Intellivon methodology: Our backend architects implement a comprehensive data readiness matrix during early database construction. This framework cleanly separates required medical record fields from optional enrichment data, protecting system processing speeds from ingestion bottlenecks.
Once your primary data streams are fully mapped, you must assemble the central workflow coordination engine.
Step 3 — Build the Workflow Orchestration Engine
The workflow engine controls how tasks move from intake to automation, review, submission, exception, and reporting.
Additionally, for autonomous revenue cycle platform build projects, this layer matters as much as the AI model because it decides when the system acts, waits, escalates, or blocks submission.
- Technical execution required: Engineers write specialized state machines, asynchronous task queues, and SLA alert rules using distributed coordination tools like Temporal.io. The engine enforces worklist prioritization thresholds, exception routing pathways, and automated network retry parameters.
- Consequences of failure: Skipping an independent orchestration service forces your automation scripts to execute without operational safeguards or system visibility. When web layouts shift, broken transactions disappear into unmanaged backend errors, destroying hospital team trust in your application.
- The Intellivon methodology: We engineer the workflow orchestration layer as an independent microservice, completely isolated from machine learning model logic. This modular design pattern prevents background model updates from freezing active hospital data transmission pipelines.
With stable orchestration utilities running, your product team can deploy its core artificial intelligence models and deterministic business rules.
Step 4 — Build the AI Model and Rules Layer
The AI layer should combine healthcare-specific LLMs, clinical NLP, classification models, and deterministic rules. LLMs should summarize, extract, and explain.
At the same time, rules engines should enforce hard payer, coding, and compliance logic. This split protects the platform from unsafe model-only decisions.
- Technical execution required: Data scientists build a dedicated clinical NLP processing pipeline to run diagnostic entity extraction and generate automated CPT code suggestions. Simultaneously, developers mount a separate rules engine to check transactions against updated NCCI edits and active insurance coverage policies.
- Consequences of failure: Relying solely on large language models introduces financial risks because probabilistic networks can hallucinate fake billing parameters. When deterministic insurance rules are treated as flexible text suggestions, your platform outputs invalid claims that trigger immediate compliance audits.
- The Intellivon methodology: We enforce a hybrid engineering strategy that uses specialized machine learning models for document interpretation and deterministic code layers for final policy enforcement. Every output passes through automated validation checks before hitting human worklists.
The next engineering milestone requires designing a high-fidelity workspace where human specialists can verify machine recommendations.
Step 5 — Design Human-in-the-Loop RCM Review
Human review should not be an afterthought. It should be designed into every high-risk workflow from the start.
At the same time, a platform like AKASA needs reviewer queues, confidence thresholds, evidence links, accept/reject actions, and audit trails so automation improves throughput without removing clinical and billing judgment.
- Technical execution required: UI engineers construct a single-pane web portal that embeds confidence-scoring metrics directly into billing worklists. The interface automatically creates a permanent coding audit trail by highlighting the exact sentences in the medical chart that triggered the AI suggestion.
- Consequences of failure: Forcing hospital teams to accept black-box machine conclusions without visible text evidence causes immediate deployment rejections from risk-averse compliance officers. Furthermore, failing to log user edits deprives your engineering team of the data required to train future software versions.
- The Intellivon methodology: We categorize system processing capabilities into four clear operational automation tiers: auto-complete, recommend-only, human-review-required, and blocked. This transparent routing taxonomy allows hospital administrators to gradually increase system autonomy as processing precision ticks upward.
Your human-in-the-loop interface layout must seamlessly feed into your platform’s core security and regulatory compliance modules.
Step 6 — Build HIPAA, Security, and Audit Controls
A HIPAA-compliant AI platform must protect PHI across storage, transmission, model inference, logs, vendor access, and reviewer workflows.
At the same time, security should include encryption, access control, audit logs, PHI de-identification, zero-trust architecture, BAA compliance, incident response, and model governance.
- Technical execution required: System administrators enforce strict role-based access controls, multi-factor login checks, and immutable database audit logs. The data ingestion layer must deploy automated PHI redaction microservices to strip identifying variables before streaming data to external model endpoints.
- Consequences of failure: Weak security design can cause personal health information to leak into public model logs, leaving hospital networks vulnerable to severe regulatory fines. Furthermore, operating without signed Business Associate Agreements (BAAs) stops enterprise sales conversations instantly during initial security evaluations.
- The Intellivon methodology: Our security squad installs production-grade encryption parameters and zero-trust data access microservices directly into the root software layer before processing live medical files. This preventative protection strategy ensures your SaaS application clears strict enterprise institutional procurement reviews.
The final phase of product launch requires launching a controlled testing environment to measure financial returns and monitor model performance.
Step 7 — Pilot, Measure, and Harden the Platform
The pilot should prove measurable RCM outcomes before broader rollout. At the same time, the strongest pilots track automation rate, reviewer override rate, denial reduction, first-pass resolution rate, cost per claim reduction, days in AR improvement, turnaround time, and model drift. These metrics decide whether the platform is ready to scale.
- Technical execution required: Product managers launch your software within a single, low-risk department to compare processing output directly against historical baseline metrics. Engineers assemble an MLOps monitoring pipeline to track real-time model drift and flag drops in inference accuracy.
- Consequences of failure: Broadening system distribution before verifying software performance in a live medical environment causes hidden model errors to scale rapidly across your customer footprint. This exposure triggers high denial rates on initial submissions, ruining your product market reputation.
- The Intellivon methodology: We treat initial pilot datasets as an active engineering foundry to harden background workflows, refine confidence thresholds, and polish user experience views. This rigorous feedback strategy ensures your platform achieves high straight-through processing rates before entering broad market distribution.
Once your system performance metrics stabilize during pilot testing, you can build out your long-term software development and maintenance budgets.
AKASA-Style AI Platform Development Cost
AKASA-style AI platform development cost usually ranges from $180,000 to $750,000+, depending on workflow scope, EHR integrations, payer connectivity, AI model depth, compliance requirements, and whether you are building an internal automation platform or a commercial RCM SaaS product.
For a platform like AKASA, the cost depends on how much operational risk the platform carries. At the same time, a tool that only recommends next steps costs less than a system that submits authorization requests, validates coding edits, drafts appeals, or routes work across multiple hospital departments.
| Development Phase | Estimated Cost | What It Covers |
| Product discovery and RCM workflow mapping | $15,000–$35,000 | Workflow scope, user roles, revenue leakage analysis, MVP roadmap |
| UX/UI for RCM teams and reviewers | $20,000–$45,000 | Worklists, dashboards, exception queues, reviewer screens |
| Data ingestion and normalization layer | $35,000–$90,000 | EHR data, payer data, claims, remittance, document processing |
| Workflow orchestration engine | $45,000–$110,000 | State machines, task routing, SLA tracking, queue management |
| AI model development | $60,000–$180,000 | Clinical NLP, LLM workflows, denial scoring, evidence extraction |
| Payer rules and coding validation engine | $35,000–$100,000 | Payer rules, NCCI edits, ICD-10-CM, CPT, medical necessity logic |
| EHR, clearinghouse, and payer integrations | $50,000–$180,000 | FHIR R4, HL7, X12, API connections, portal fallback |
| HIPAA security and compliance controls | $35,000–$90,000 | RBAC, encryption, audit logs, PHI controls, BAA readiness |
| MLOps, monitoring, and analytics | $30,000–$85,000 | Model drift, KPI dashboards, alerts, production reporting |
| QA, pilot, deployment, and hardening | $35,000–$85,000 | Test cases, user acceptance, edge-case tuning, and release management |
Ongoing maintenance usually costs 18%–28% of the initial build cost per year. At the same time, this budget covers payer rule updates, model monitoring, integration maintenance, cloud infrastructure, security reviews, workflow optimization, and support for new customer environments.
For example, a $400,000 platform may require $72,000–$112,000 per year to keep it secure, accurate, and production-ready.
Get Your AKASA-Style AI Platform Cost Estimate
Building a custom AI RCM automation platform requires clear cost planning across workflows, integrations, AI models, compliance, and rollout. For this, Intellivon can help you estimate the investment required for your platform roadmap before development begins.
Conclusion
Building a platform like AKASA is a serious infrastructure commitment that requires combining secure EHR connectivity, healthcare-specific LLMs, and deterministic payer logic. Additionally, for founders, the most reliable roadmap is not copying every feature at launch.
Instead, focus on a high-value workflow wedge like prior authorization or claim status tracking to prove automation safely. Expanding into a broader autonomous revenue cycle platform should only happen after your core workflows earn trust.
Build an AKASA-Style Healthcare AI Platform With Intellivon
Intellivon helps healthcare SaaS founders, RCM companies, and enterprise teams build custom healthcare AI automation platforms around real workflows, not generic AI demos. At the same time, for an AKASA-style build, the roadmap should start with workflow scope, architecture, compliance controls, integration planning, model design, and measurable revenue cycle KPIs.
With 500K+ engineering hours, ex-MAANG engineers, and deep experience across AI, healthcare platforms, SaaS systems, API integrations, and enterprise software development, Intellivon helps teams build controlled healthcare AI infrastructure for prior authorization, coding, claims, denials, appeals, and revenue operations.
A. Define The Right Healthcare AI Automation Scope
Before development starts, we help you identify which revenue cycle workflows should be automated first and which still need human review.
We help you plan:
- Prior authorization, coding, claims, denial, and appeal workflows
- AI use case prioritization based on operational value
- Human-in-the-loop review points for high-risk decisions
- MVP scope, rollout phases, and KPI measurement
This keeps the platform focused on measurable workflow improvement, not disconnected AI features.
B. Design The Platform Architecture Around RCM Operations
Healthcare AI automation platforms need a secure architecture that connects clinical, billing, payer, and financial data without breaking daily operations.
Your platform can include:
- EHR, clearinghouse, payer, and billing integrations
- Healthcare-specific LLM and clinical NLP workflows
- HIPAA-compliant AI platform architecture
- Audit logs, access controls, and workflow dashboards
This gives your team a foundation that can support automation across multiple revenue cycle functions.
C. Build AI Models Teams Can Review And Trust
AI should support RCM teams with evidence, confidence scores, and clear recommendations. At the same time, it should not create black-box outputs that teams cannot verify.
Your platform can include:
- Clinical NLP for documentation extraction
- LLM workflows for summaries and appeal context
- Denial prediction and claim risk scoring
- MLOps pipelines for monitoring and model updates
Every model is designed to keep automation explainable, trackable, and production-ready.
Ready To Build An AKASA-Style Healthcare AI Platform?
If you are planning to build a healthcare AI revenue cycle platform with capabilities around prior authorization, coding, denial prevention, claims, or appeals, Intellivon can help you define the roadmap before development begins.
At the same time, we will help you map workflows, plan integrations, design secure architecture, build AI models, set up monitoring, and estimate cost before the first development sprint.
Things To Know About Building a Platform Like AKASA
Q1.How much does it cost to build a platform like AKASA?
A1. A platform like AKASA usually costs $180,000 to $750,000+ to build. At the same time, a focused MVP covering one workflow, such as prior authorization or denial prevention, sits near the lower range. Additionally, a full autonomous RCM SaaS platform with EHR integrations, healthcare-specific LLMs, payer rules, HIPAA controls, and MLOps moves toward the higher range.
Q2. How long does it take to build autonomous RCM software?
A2. A focused MVP usually takes 4–7 months, while a full enterprise platform takes 9–18 months. Therefore, the timeline depends on EHR access, payer integration complexity, model validation, compliance documentation, and pilot readiness. At the same time, teams should avoid promising full autonomy before they prove one workflow safely.
Q3. Should founders build or buy an AKASA-style platform?
A3. Founders should buy when they need operational improvement within one organization. At the same time, they should build when the AI RCM platform is the product, the business model depends on workflow ownership, or existing vendors cannot support the target specialty. Additionally, a build makes sense when proprietary data and product differentiation justify the compliance and integration burden.
Q4. Can an AI prior authorization automation platform build projects to reduce denials safely?
A4. Yes, but only when the system combines payer rules, clinical evidence extraction, human review, and audit trails. Therefore, founders worry less about the AI demo and more about adoption, integration, trust, job impact, and data governance. The safest model automates low-risk tasks first and escalates uncertain cases.



