

Key Takeaways:
-
Enterprise AI RCM software must be built as a governed revenue infrastructure, not a billing chatbot.
-
The build starts with workflow mapping, EHR integration, data normalization, and payer-rule design.
-
Custom builds range from $70,000 to $270,000 with 15 to 25% annual maintenance costs.
-
HIPAA controls, MLOps, human review workflows, and phased rollout are non-negotiable production requirements.
-
Intellivon positions platforms around denial prevention, coding support, authorization workflows, and audit-ready financial control.
Revenue cycle management is the financial lifecycle of every patient encounter, running from eligibility verification and prior authorization at intake to payment posting and denial resolution at the back end. Several hospitals still run this chain on legacy billing tools that are not compatible with the current complexity of payers. This is because billing teams verify eligibility, assign ICD-10-CM and CPT codes from clinical documentation, and investigate denials only after they return, one encounter at a time.
As volume scales, this model becomes a structural constraint on cash flow and erodes long-term ROI. According to the AHA’s 2024 administrative cost report, hospitals spend an estimated $40 billion annually on billing and collections, and care denials for Medicare Advantage claims grew 55.7% between 2022 and 2023. Therefore, tools that cannot read unstructured clinical notes before submission will compress your margins and erode the financial confidence of the teams running the cycle.
An enterprise AI revenue cycle management software changes this outcome. It reads unstructured clinical documentation, assigns coding recommendations with confidence scoring, applies payer-specific logic pre-submission, and routes exception cases to human review. The software does all this within a compliance architecture that is built to sustain expansion under payer scrutiny.
At Intellivon, we build healthcare AI systems where claims logic, payer rules engines, and clinical NLP need to work together in production. This blog covers what building that platform actually requires from the ground up.

What is an Enterprise AI Revenue Cycle Management System?
Enterprise AI revenue cycle management is a hospital financial operations system that uses AI, automation, payer rules, and secure integrations to manage revenue workflows from patient registration to final payment reconciliation.
It connects patient access, documentation, coding, claims, denials, payments, and analytics into one controlled operating layer. Unlike generic billing software that relies on brittle, manually maintained logic chains, this system continuously adapts to changing payer behavior patterns.
A. AI RCM vs. Generic Billing Software
Traditional billing systems serve as passive databases that require manual administrative entry at every major operational checkpoint.
In contrast, an intelligent revenue platform dynamically validates claims data against active payer rule engines before submission occurs.
RCM vs. Generic Billing Software
| Capabilities | Generic Billing Software | Enterprise AI RCM |
| Data Processing | Manual data entry and static rule validation | Real-time automated data extraction and validation |
| Payer Rule Updates | Manual software script re-writing | Autonomous machine learning rule adjustment |
| Denial Management | Reactive tracking after receiving rejections | Predictive modeling to stop denials before submission |
Transitioning to an intelligent orchestration layer allows engineering teams to phase out legacy batch-processing infrastructure entirely. This shift changes financial operations from a reactive cleanup process into a predictive, real-time data workflow.
B. Front-End, Mid-Cycle, and Back-End RCM Infrastructure
An AI revenue system handles three main jobs: checking patients in, reading doctor notes, and processing payments.
1. Front-End: Checking Patients In
The software starts working the moment a patient schedules a visit. It uses patient registration automation to instantly scan insurance cards, run an insurance eligibility verification check, and handle the prior authorization workflow before the patient ever sees a doctor.
2. Mid-Cycle: Reading Doctor Notes
Once the doctor treats the patient, the AI uses natural language processing, which is just software that can read text, to look over the medical notes.
It helps with clinical documentation improvement and computer-assisted coding to match the treatment with the exact ICD-10-CM coding automation and CPT code assignment needed for the bill.
3. Back-End: Sending Bills and Tracking Money
Finally, the system runs the automated claims submission workflow to send the bill to the insurance clearinghouse, which is the network that delivers bills to payers.
When the insurance company responds, the software automatically processes the digital receipt, handles ERA processing, and alerts your team if a bill is underpaid.
This three-step setup stops financial leaks by catching mistakes immediately. Connecting these steps ensures the hospital tracks money smoothly from the moment a patient walks in until the bank deposit clears.
Now that we know how this system works, the next step is looking at the actual software parts you need to build it.
Why Hospitals Build AI RCM Software Instead Of Buying More Point Tools
Hospitals are increasingly choosing integrated AI RCM platforms over more point tools because the market is rewarding workflow orchestration, not isolated automation.
The latest market signals show rapid AI RCM growth, rising provider adoption, and a clear preference for unified platforms that reduce denial leakage, staffing burden, and integration sprawl.
Grand View Research valued the global AI RCM market at $20.63 billion in 2024. That figure is projected to reach $70.12 billion by 2030, a 24.16% CAGR across five years. The growth reflects health systems actively shifting budgets away from manual billing operations and into AI infrastructure.
Hospitals build AI RCM software when fragmented tools no longer match their payer mix, EHR environment, specialty workflows, denial patterns, or compliance requirements. A custom build gives technical teams control over data flow, rules logic, AI behavior, audit trails, and workflow ownership.
The Problem with Buying Vendor Tools
Buying generic software is faster at first, but it often creates tool sprawl. Tech leads often complain that vendor tools only handle one slice of billing and fail to talk to each other. When eligibility, coding, and denials sit in separate tools, you lose visibility, and data gets trapped in silos.
Problem With Buying Vendor Tools
| Decision Area | Buy Vendor RCM Tool | Build Custom AI RCM Software |
| Workflow fit | Standardized | Hospital-specific |
| Data ownership | Vendor-limited | Internal control |
| AI transparency | Varies by vendor | Designed into the system |
Building your own platform makes sense when you need total data ownership and a system tailored to your exact local insurance rules.
The strongest build cases appear when hospitals map AI to the full revenue cycle, not one isolated workflow.
Where AI Fits Across The Hospital Revenue Cycle
AI fits best in revenue cycle workflows where data volume, repetitive review, payer variation, and documentation complexity slow human teams down. The strongest use cases include eligibility checks, authorization routing, CDI, coding support, claim scrubbing, denial prediction, appeals drafting, payment reconciliation, and underpayment recovery.
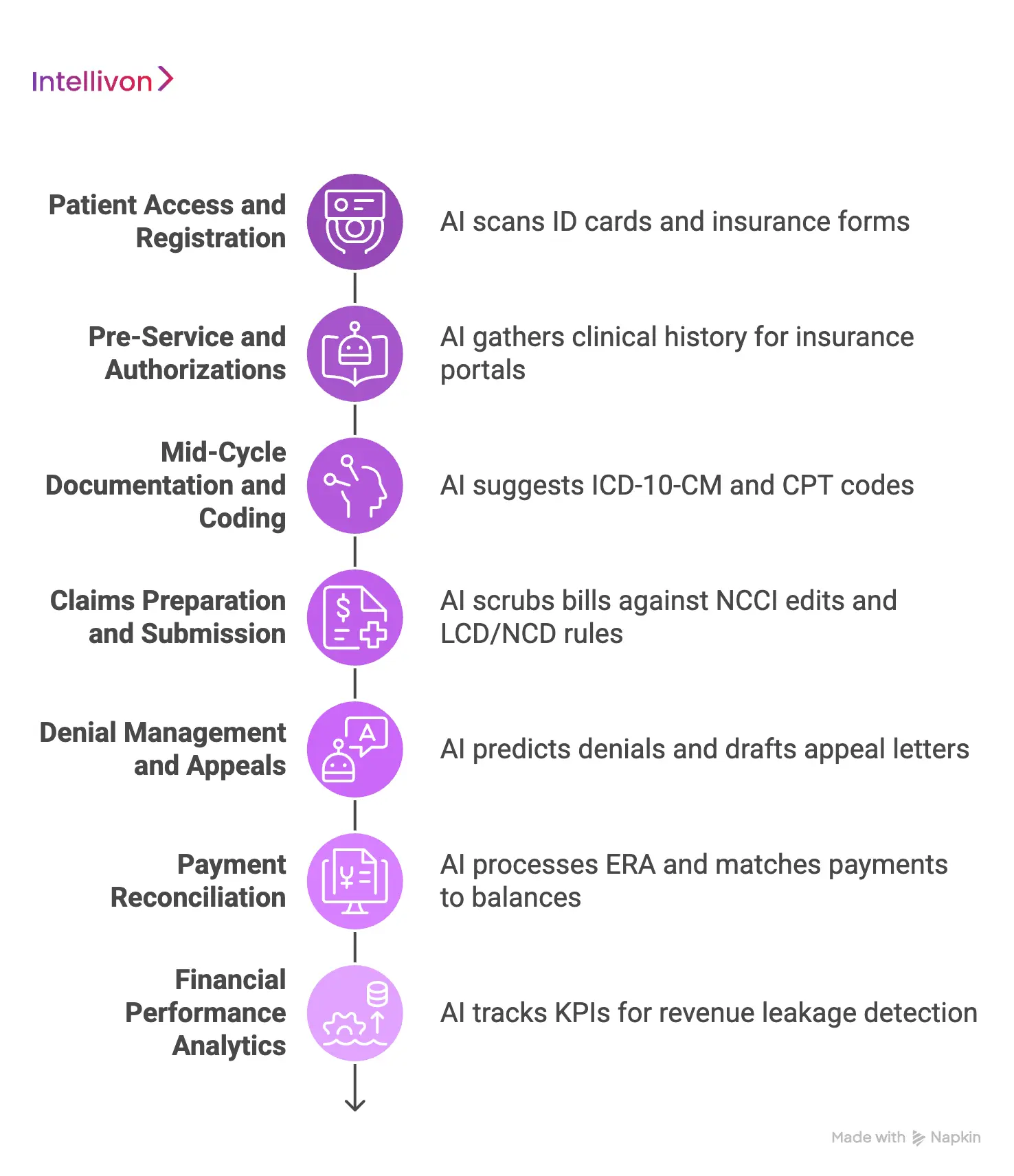
1. Patient Access and Registration
The front end of the billing cycle handles patient registration automation and instant insurance eligibility verification. AI software scans photo ID cards and insurance forms immediately when a patient checks in.
By matching this data against active health insurance networks, the system stops identity errors and uncovers inactive policies before a medical chart is even opened.
2. Pre-Service and Authorizations
Getting approval for a medical procedure requires a strict prior authorization workflow and automated medical necessity checking. The software automatically gathers clinical history from doctor notes and pushes it directly into specific insurance portals.
This stops care delays by highlighting missing medical documentation before the hospital schedules a surgery or treatment session.
3. Mid-Cycle Documentation and Coding
Middle-office billing workflows rely on natural language processing to handle clinical documentation improvement and computer-assisted coding tasks.
As doctors type their charts, the AI reads the unstructured clinical text to suggest highly accurate ICD-10-CM coding automation choices.
It also handles CPT code assignment to make sure every performed procedure is logged correctly for the bill.
4. Claims Preparation and Submission
Sending clean bills requires automated charge capture automation alongside a rigorous, rule-guided claims submission workflow. The software automatically scrubs every bill against official NCCI edits to check for bundled procedures.
Additionally, it verifies local LCD / NCD compliance rules to make sure the hospital meets specific geographic insurance requirements before final delivery.
5. Denial Management and Appeals
When insurance companies refuse to pay, the system deploys a predictive denial prediction model and automated denial root cause analysis. The software reads insurance rejection text to categorize why the bill failed.
It then handles appeals automation by pulling historical clinical records and drafting custom appeal letters for human billing teams to review.
6. Payment Reconciliation
Closing out invoices requires automated ERA processing and secure, end-to-end payment reconciliation. The application ingests digital check stubs from banks and matches them against open balance sheets.
If an insurance company pays less than its contracted amount, the platform flags the transaction for underpayment recovery so the hospital can recoup missing funds.
7. Financial Performance Analytics
Advanced analytical tools provide instant revenue leakage detection by tracking core operational performance indicators. The software monitors your first-pass acceptance rate to see how many bills clear on the first submission.
By watching net days in AR and the overall cost to collect, finance leads can spot exactly which insurance company workflows need adjustment.
Deploying these smart tools across all seven stages eliminates the communication gaps that plague legacy hospital billing setups. This unified approach keeps data clean and accessible from initial patient contact to final balance reconciliation.
After workflow mapping, the architecture must separate transaction logic, AI inference, human review, and audit controls.
Enterprise AI Revenue Cycle Management Software Architecture
Enterprise AI revenue cycle management architecture should separate integration, data normalization, workflow orchestration, payer rules, AI inference, human review, analytics, and security into modular layers.
This prevents billing logic, model outputs, PHI access, and audit events from becoming tangled inside one fragile system. Breaking the code into isolated services ensures that updating a single insurance rule will never crash your entire patient database.
The Modular RCM Technical Blueprint
Building a production-ready billing engine requires organizing your codebase into clear functional tiers. The table below details what happens inside each architectural layer and the specific technologies needed to run them.
Modular RCM Technical Blueprint
| Operational Layer | Internal System Process | Core Technical Stack |
| Integration Layer | Pulls and pushes data across different systems using EHR API integration protocols. It manages native Epic integration and Cerner integration setups to sync records. | FHIR document API, HL7 CDA, and secure Webhooks |
| Data Normalization Layer | Cleans messy hospital data and transforms demographics, encounter data, charges, clinical notes, and payer policies into a single clean format. | Apache Spark, Python data pipelines, and PostgreSQL |
| RCM Microservices Architecture | Runs independent software programs for separate billing tasks like eligibility, prior authorization, coding, claims, denials, and appeals. | Docker containers, Kubernetes, and Node.js microservices |
| Event-Driven Architecture | Tracks real-time billing triggers like claim-created, authorization-required, code-suggested, denial-predicted, and ERA-received. | Apache Kafka, RabbitMQ, and event messaging lines |
| Payer Rules Engine | Runs deterministic checks to catch bundled codes using NCCI edits. It evaluates active LCD / NCD compliance and handles medical necessity checking. | Drools, Python rule blocks, and custom SQL verification |
| AI Processing Layer | Deploys NLP and specialized LLM networks to handle text classification, risk prediction, entity extraction, and automatic appeal letter summarization. | PyTorch, Hugging Face clinical models, and AWS SageMaker |
| Human Review Layer | Measures machine output with a clear confidence scoring system. It routes low-confidence bills to exception queues and handles override tracking. | React dashboards, Redis queues, and human feedback loops |
| Governance Layer | Keeps an unalterable coding audit trail and logs every instance of PHI access while running model drift monitoring to keep AI models accurate. | OpenSearch, Prometheus metrics, and immutable ledger DBs |
| Analytics Layer | Calculates historical AR aging, monitors the first-pass acceptance rate, and tracks the overall hospital cost to collect. | ClickHouse database, Tableau APIs, and Python analytics |
[For a deeper breakdown of revenue automation architecture, see our guide on How to Build an AI Revenue Automation Platform.]
Separating your software code into distinct, independent blocks protects data integrity and makes future system updates straightforward. This clean structural design ensures the billing platform remains stable even as underlying insurance regulations change.
Architecture only works when the platform has the right hospital-grade feature set.
AI Models Required For Revenue Cycle Software Development
AI revenue cycle software needs a hybrid model stack, not one general model. Hospitals usually need OCR, clinical NLP, classification models, denial prediction, coding recommendation models, payment variance detection, LLM-assisted summarization, and deterministic rules that override AI where billing logic must be exact.
Deploying this multi-model approach ensures your financial platform remains both flexible and highly accurate.
The Revenue Cycle AI Model Map
Building a production platform requires matching specific software engines to distinct financial tasks. The table below outlines the core machine learning models, their target tasks, and what triggers human intervention.
The Revenue Cycle AI Model Map
| AI Capability | Best-Fit Use Case | Human Review Trigger |
| OCR (Optical Character Recognition) | Reads PDFs, scanned payer letters, and insurance forms | Low extraction confidence score |
| Clinical NLP | Handles CDI, documentation review, and medical necessity tasks | Missing medical record evidence |
| Coding Model | Generates ICD-10-CM and CPT suggestions from charts | Complex multi-specialty cases |
| Denial Prediction Model | Calculates pre-submission risk scoring for bills | High-risk claim flag |
| LLM Summarization | Builds appeal drafts and summarizes long payer letters | Policy-cited decision check |
| Payment Variance Model | Finds underpayment issues and tracks payment gaps | Payer contract mismatch flag |
| Rules Engine | Checks NCCI edits and local LCD / NCD compliance | Absolute rule—no AI override allowed |
Implementation Requirements for Core Models
Modern billing platforms rely on specialized machine learning tools to handle complex clinical documents.
To ensure high accuracy, engineering teams must build clear boundaries around how these models extract data, predict risks, and surface answers.
- LLM Document Summarization: Large language models must focus strictly on text summarization and evidence retrieval tasks. These models pull specific sentences from lengthy insurance contracts to back up appeal letters automatically.
- NLP Fact Extraction: Natural language processing software must extract structured data from unorganized doctor notes. The engine looks for concrete variables like medication dosages, treatment dates, and specific clinical diagnoses.
- Predictive Risk Scoring: Predictive algorithms analyze previous insurance rejections to calculate denial risks before a bill leaves the hospital. This scoring lets billing teams prioritize high-value accounts receivable (AR) cases that are likely to pay quickly.
- Confidence Scoring Thresholds: Every machine output requires an internal confidence score to determine automation versus human review. If an automated code suggestion falls below a 85% confidence score, the system routes the bill to a human workspace.
- Explainable AI Recommendations: The platform must display the exact sentence from the doctor’s notes that caused a specific code suggestion. Showing clear source evidence allows human auditors to verify billing compliance instantly.
[For a deeper breakdown of coding workflows, see our guide on How to Build an AI Medical Coding Platform.]
Using a mixed model stack protects your hospital from the unpredictable answers common in general chat tools. This architecture keeps your billing logic grounded in verifiable clinical documentation and active insurance rules.
Even the best model fails if the platform cannot exchange data with EHRs, clearinghouses, and payer systems.
Integration Requirements For EHRs And Clearinghouses
AI RCM software must integrate with hospital EHRs, practice management systems, clearinghouses, payer APIs, document repositories, and finance systems. The core integration stack should support FHIR, HL7, CDA, X12 EDI, EHR APIs, clearinghouse transactions, and secure file exchange.
Getting these data channels connected correctly stops administrative lag and feeds your automation models a steady stream of clean operational data.
1. Epic EHR System Connection
Connecting directly to Epic requires using the App Market portal to hook into native web service layers. You must set up real-time programming hooks that sync patient schedules, clinical charts, and billing buckets automatically.
The platform reads clinical events instantly to trigger background coding checks without forcing the billing staff to log into a separate screen.
2. Oracle Health and Cerner Synchronization
Interfacing with Cerner architectures requires using the Millennium platform APIs and standard system data feeds. Because Cerner installations often vary wildly by hospital location, your software must use a flexible data-mapping layer to match fields accurately.
This layer standardizes diverse hospital chart formats so your background AI models receive the exact text parameters they expect.
3. FHIR Document API Core Access
The platform uses the HL7 FHIR R4 standard to query specific clinical notes, lab results, and patient histories directly from the record database. By pulling data through predefined structural fields, the AI software skips messy screen-scraping techniques entirely.
This secure data access provides the clean text foundations needed to run accurate automated necessity checking before a bill is built.
4. HL7 CDA Legacy Data Transfers
Many regional hospitals still share clinical data using older Clinical Document Architecture files. To handle these setups, the system runs continuous background parsing engines that convert older text files into modern, searchable databases.
This step makes sure that unstructured physician summaries from outside networks can still be used to back up your internal documentation review.
5. X12 270 and 271 Eligibility Verification
Checking insurance coverage requires sending electronic X12 270 inquiry files to payer networks and receiving X12 271 response files instantly.
The software automates this check during nightly batch jobs before a patient arrives for care. If a policy is found to be inactive, the system immediately flags the record so your intake team can update the information.
6. X12 278 Prior Authorization Mapping
Automating approval workflows requires formatting clinical justifications into standard electronic X12 278 request files. At the same time, the platform bundles the doctor’s notes, matches them to the insurance company’s guidelines, and submits the data straight to the payer portal.
This pipeline monitors response codes closely, shortening overall approval turnaround times from weeks down to minutes.
7. X12 837 Claim Submissions
Sending bills out requires compiling patient data, institutional fees, and medical codes into complete X12 837 transaction files. At the same time, the application runs internal compliance checks across this data block to fix formatting errors before final delivery.
This upfront review ensures the claim meets strict technical standards before it ever reaches an outside clearinghouse network.
8. X12 835 Electronic Remittance Advice
When an insurance carrier makes a payment choice, they return an X12 835 file containing detailed deposit and rejection data. Additionally, the software ingests this receipt automatically to handle ERA processing and balance matching tasks.
Therefore, the application uncovers hidden underpayments immediately by comparing the actual paid amount against the hospital’s original contract rate rules.
9. Clearinghouse Network Integration
Connecting to massive clearinghouse networks like Waystar or Change Healthcare requires using secure internet communication channels. At the same time, the platform uses these connections to deliver clean claims batches and pull down raw rejection reports hourly.
Therefore, integrating directly via web services allows your engineering team to clear out slow, old-fashioned text file uploads entirely.
10. Direct Payer API Connections
While older systems rely on slow electronic data files, modern health insurance networks are shifting quickly toward direct web API access. At the same time, CMS has pushed major payer API implementation deadlines to January 1, 2027, under the interoperability and prior authorization final rule.
Building native API connections now allows your system to get instant automated approval decisions from major commercial insurers.
Connecting these various data pipelines eliminates the manual file handling steps where billing information frequently gets corrupted. This end-to-end integration ensures that your automated software models can pull clinical text and push financial claims without hitting walls.
Once data moves across systems, HIPAA controls need to shape every engineering decision.
HIPAA-Compliant Revenue Cycle Software Controls
HIPAA-compliant revenue cycle software must protect PHI through administrative, physical, and technical safeguards. For AI RCM platforms, that means encryption, access controls, audit logs, PHI tokenization, vendor governance, BAA coverage, secure model inference, retention policies, and incident response workflows.
Setting up these defensive barriers protects patient privacy and saves your hospital from costly regulatory fines.
1. Understanding the HIPAA Security Rule
The HIPAA Security Rule says hospitals must use appropriate administrative, physical, and technical protections to keep digital health data secure. So, when building AI software, your engineering team cannot treat compliance as a final checkmark.
Instead, you must design security rules straight into the database layer so the software safeguards data automatically.
2. Core Data Protections and Engineering Controls
Keeping a custom billing platform compliant requires isolating sensitive patient data from your main AI processing layers. So, use these specific data controls to secure your system:
- PHI Tokenization: The software strips out names, social security numbers, and birth dates from medical records before sending them to large language models. The system replaces this private text with randomized tracking keys, keeping the data anonymous.
- Zero-Trust Architecture: Your system must assume every device and user is a security risk until proven otherwise. The platform checks digital credentials constantly, ensuring no single user can access the entire hospital network without continuous authorization.
- Role-Based Access Control: The platform restricts software views based on job descriptions. Intake staff can view patient registration data, medical coders can view clinical notes, and AI background processes can only look at anonymous data streams.
- Encryption Setup: All health data must be scrambled using AES-256 keys while sitting in your databases. When data moves across the web to insurance clearinghouses, it must travel through encrypted TLS 1.3 channels to stop data theft.
- Strict BAA Requirements: You must sign a Business Associate Agreement with every cloud provider or database vendor you use. This legal document ensures that your outside infrastructure partners follow the exact same privacy rules that your hospital does.
3. Monitoring AI Decisions and Audits
AI systems can change how they handle data over time, which requires continuous operational oversight. This is why setting up automated monitoring blocks keeps your models accurate and compliant:
- Immutable Coding Audit Trail: The software saves every single automated code suggestion to a permanent log file. If a human worker overrides an AI billing recommendation, the platform records the employee’s name, the date, and their reasoning.
- Model Drift Monitoring: Background tools track the performance of your machine learning models hourly. If a model’s clinical accuracy drops because a payer changes its form layout, the system alerts your developers to retrain the code.
- Data Minimization Pipelines: Your software should only ingest the minimum amount of text needed to process a specific bill. The platform automatically blocks out unrelated medical history, like old family histories or unrelated lab results.
- Model Access Boundaries: The system must never use live patient charts to train public AI models. All internal model adjustments must happen within secure, isolated sandboxes that have no contact with the outside internet.
Building these tracking structures directly into your software ensures your financial operations pass federal audits without issue. This defensive design protects your organization from data leaks while allowing your automated billing pipelines to run smoothly. At the same time, compliance should be built into each step of the software roadmap.
How To Develop AI Revenue Cycle Software For Hospitals
To develop AI revenue cycle software for hospitals, start with workflow discovery, then design the architecture, build the integration layer, configure payer rules, develop AI models, create human review queues, implement HIPAA controls, test against real claims, and roll out through a phased pilot.
This systematic method keeps your engineering milestones closely aligned with real billing office needs. Therefore, taking a structured approach prevents your software developers from building expensive functions that do not match how hospital billers actually work.
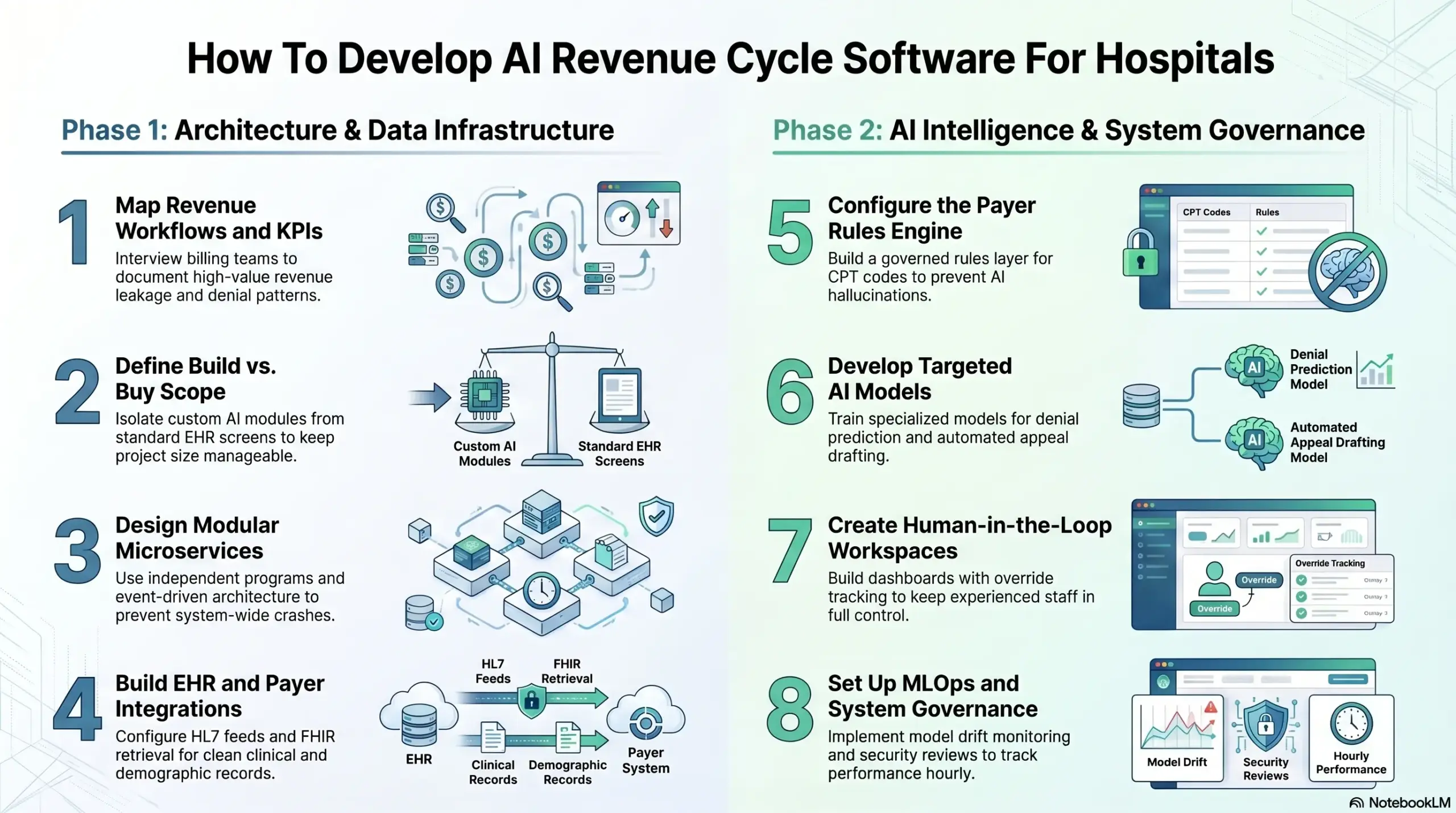
Step 1 — Map Revenue Workflows and KPIs
Start by mapping the hospital’s current workflows, payer mix, denial patterns, and core financial metrics like your first-pass acceptance rate. This layout creates your software blueprint.
- Technical Scope: Interview billing and coding teams to map patient registration, eligibility, prior authorization, and payments. Document high-value revenue leakage points and specific insurance denial codes.
- What Goes Wrong: Skipping this phase means you might optimize low-value tasks while major financial leaks stay completely untouched.
- Intellivon Approach: We start with deep workflow and claims-data discovery before mapping software architecture, matching the build to actual hospital operations.
Step 2 — Define Build vs. Buy Scope
Define what should be custom-built or left inside existing systems before engineering begins to keep your project size manageable.
- Technical Scope: Isolate custom AI modules from standard EHR screens. Decide which modules remain in legacy billing systems and map vendor integration boundaries.
- What Goes Wrong: The project quickly becomes too expensive and bloated as developers try to rebuild standard database features.
- Intellivon Approach: Intellivon focuses the custom build strictly around high-friction workflows like denial prediction, coding support, and underpayment recovery to save you time and budget.
Step 3 — Design Modular Microservices
Design the platform as independent software programs—or microservices—for eligibility, authorizations, coding, and claims.
- Technical Scope: Establish clear service boundaries and set up a real-time event-driven architecture using tools like Apache Kafka. Separate heavy AI processing from standard transaction databases.
- What Goes Wrong: In a single, lumped codebase, an update to a front-end rule can easily crash your entire back-end bank reconciliation tables.
- Intellivon Approach: We isolate rules, workflows, AI models, and audit logs so you can update single components without taking the entire hospital platform offline.
Step 4 — Build EHR and Payer Integrations
Build your data pipelines early because AI billing software depends entirely on clean clinical, demographic, and payment records.
- Technical Scope: Set up secure EHR API integration channels with Epic and Cerner. Use FHIR document retrieval and HL7 feeds while configuring electronic X12 270/271, 278, 837, and 835 transactions.
- What Goes Wrong: Staff will end up copying data between Windows by hand, which slows down adoption and causes data entry errors.
- Intellivon Approach: Our team completes integration setup before finalizing AI models because model quality depends on reliable data exchange.
Step 5 — Configure the Payer Rules Engine
A payer rules engine validates claims against insurance requirements, NCCI edits, and local LCD / NCD policies.
- Technical Scope: Create a versioned database layer to hold specific payer guidelines. Build workflows that check CPT codes, modifiers, and authorization requirements before bills leave the hospital.
- What Goes Wrong: Relying on AI prompts alone to remember insurance rules causes hallucinations and high denial rates.
- Intellivon Approach: Intellivon builds payer logic as a hard-coded, governed rules layer next to AI models, ensuring complete compliance.
Step 6 — Develop Targeted AI Models
Develop specialized AI models for specific financial decisions rather than making broad automation claims.
- Technical Scope: Train a localized denial prediction model. Build natural language processing tools for computer-assisted coding and tie them to LLMs for automated appeal drafting.
- What Goes Wrong: Generic models deliver weak automation, missing complex underpayments, and nuanced insurance rejections.
- Intellivon Approach: We pair custom models with confidence scoring thresholds so the system flags uncertain outputs for human review.
Step 7 — Create Human-in-the-Loop Workspaces
Human review is mandatory for complex claims, low-confidence coding recommendations, and high-value financial disputes.
- Technical Scope: Build clear dashboards split by employee roles. Set up override tracking and display the exact source sentences that caused an AI recommendation.
- What Goes Wrong: Medical coders will ignore automated suggestions entirely if they cannot see the underlying logic behind the software’s decisions.
- Intellivon Approach: Intellivon designs AI as a secure decision support tool for human billers, keeping your experienced staff in full control.
Step 8 — Set Up MLOps and System Governance
Launch the billing platform with model drift monitoring, active security reviews, and live performance tracking.
- Technical Scope: Establish automated MLOps pipelines to handle model updates. Track performance drops hourly and funnel operational metrics into a central KPI dashboard.
- What Goes Wrong: The system may perform well during an initial pilot but degrade quietly in production as insurers change their forms.
- Intellivon Approach: We treat launch day as the beginning of platform governance, embedding automated monitoring tools to keep your system accurate.
This clean development path protects your hospital from technical debt and keeps your data completely secure. Therefore, building in clear stages ensures your platform delivers a high return on investment.
AI RCM Software Development Cost For Hospitals
AI RCM software development for hospitals with Intellivon usually costs $50,000 to $300,000, depending on workflow scope, EHR integration depth, payer connectivity, AI model complexity, HIPAA controls, and enterprise deployment requirements.
A focused MVP may start with denial prediction, claims validation, or payment posting automation. Additionally, a larger hospital-grade platform may include EHR workflows, EDI 837/835, payer rules, AI models, audit controls, and executive KPI dashboards.
AI RCM Software Development Cost Breakdown With Intellivon
| Development Phase | Estimated Cost | What Intellivon Covers |
| Discovery, workflow mapping, and KPI audit | $3,000–$8,000 | We review your RCM workflows, payer mix, denial patterns, claim flow, system landscape, and MVP priorities. |
| Product strategy and UX design | $4,000–$12,000 | We design user roles, dashboards, review queues, exception workflows, CFO views, and admin controls. |
| Backend and workflow engine | $8,000–$32,000 | We build task routing, claim states, rules workflows, APIs, user permissions, and platform logic. |
| EHR, FHIR, HL7, and clearinghouse integrations | $8,000–$38,000 | We connect EHRs, FHIR APIs, HL7 feeds, clearinghouses, and relevant healthcare data systems. |
| EDI 837/835 and payer transaction workflows | $6,000–$28,000 | We support claim submission, remittance processing, eligibility checks, claim status, and payer data movement. |
| AI model development | $8,000–$50,000 | We build NLP, denial prediction, CAC support, LLM summarization, AR prioritization, and payment variance models. |
| Payer rules engine and compliance logic | $5,000–$22,000 | We configure payer edits, LCD/NCD logic, medical necessity checks, contract rules, and claim validation logic. |
| HIPAA security and audit controls | $5,000–$24,000 | We implement RBAC, encryption, PHI controls, audit logs, access permissions, and compliance-ready documentation. |
| Analytics, KPI dashboards, and ROI reporting | $3,000–$14,000 | We track denial rate, clean claim rate, days in AR, net collection rate, cost per claim, and workflow performance. |
| Testing, QA, and validation | $4,000–$18,000 | We test claims workflows, AI outputs, integrations, compliance controls, edge cases, and platform reliability. |
| Pilot launch and optimization | $3,000–$18,000 | We support rollout, user training, monitoring, feedback loops, workflow refinements, and early performance tracking. |
| Scope buffer and implementation adjustments | $3,000–$36,000 | We account for integration changes, payer-rule updates, dashboard refinements, compliance needs, and launch support. |
Total estimated development cost with Intellivon: $50,000–$300,000
The lower end works for a focused AI RCM MVP with limited integrations and one or two automation workflows. At the same time, the higher end applies when hospitals need deeper EHR connectivity, EDI workflows, payer-rule logic, AI model development, HIPAA controls, analytics, and production rollout support.
Ongoing Maintenance With Intellivon
Plan for 15%–25% of the initial build cost annually for payer-rule updates, model drift monitoring, integration maintenance, compliance reviews, security patches, workflow improvements, and platform support.
For example, a $100,000 AI RCM software build may need $15,000–$25,000 per year in maintenance. At the same time, a $300,000 enterprise-grade build may need $45,000–$75,000 per year, especially if it includes AI models, EHR integrations, EDI 837/835 workflows, payer-rule logic, and HIPAA audit controls.
Planning an AI revenue cycle software build for your hospital, RCM company, or healthcare SaaS platform? Intellivon can help you estimate the cost based on your workflow scope, payer mix, EHR integrations, AI modules, HIPAA controls, compliance requirements, and launch timeline.
Cost planning becomes more useful when it is tied to your actual RCM workflows, not a generic software range. Contact Intellivon to discuss your AI RCM software development roadmap and get a build estimate for your platform.
Conclusion
Enterprise AI revenue cycle management works when hospitals treat it as production infrastructure, not a feature layer. At the same time, the strongest platforms connect registration, eligibility, prior authorization, CDI, coding, claims, denials, payments, analytics, and compliance into one governed system.
For CTOs and product leaders, the practical decision is not whether AI belongs in RCM. At the same time, it is where AI should automate, where rules should control, where humans must review, and how the architecture will keep improving after launch.
A custom build makes sense when integration depth, payer-rule ownership, AI transparency, and long-term revenue control matter more than short-term software convenience.
Build Enterprise AI RCM Software With Intellivon
Intellivon builds enterprise AI revenue cycle management software around hospital workflows, secure healthcare integrations, payer-rule logic, explainable AI recommendations, human review, HIPAA controls, and measurable revenue outcomes.
With 500K+ engineering hours, ex-MAANG engineers, and deep experience across AI, healthcare platforms, SaaS systems, API integrations, and enterprise software development, Intellivon helps teams move from fragmented RCM tools to scalable AI-powered revenue cycle infrastructure.
A. Define The Right RCM Automation Scope
Before development starts, we help you define which revenue cycle workflows should be automated first and which workflows still need human review.
This includes mapping front-end, mid-cycle, and back-end RCM operations across patient access, eligibility verification, prior authorization, charge capture, coding, claims scrubbing, denial management, payment posting, and AR follow-up.
We help you plan:
- MVP feature scope
- Front-end RCM workflows
- Mid-cycle coding and documentation flows
- Back-end claims and payment workflows
- Build vs buy decisions
- AI automation opportunities
- Denial reduction priorities
- ROI assumptions
- KPI measurement plan
- Compliance and rollout requirements
This keeps the first version focused, practical, and tied to measurable revenue cycle outcomes.
B. Design The Platform Architecture Around Hospital Operations
Enterprise AI RCM software needs an architecture that can support real hospital complexity. This means the platform must handle clinical data, claims data, payer rules, payment files, user roles, audit logs, and AI recommendations without creating another disconnected system.
Intellivon designs AI RCM platforms around a modular, scalable architecture.
Your platform can include:
- RCM microservices architecture
- Event-driven workflow design
- EHR and clearinghouse integration
- Data normalization layer
- Claims workflow orchestration
- Payer-rule processing
- Audit-ready system design
- Role-based dashboards
- Revenue analytics infrastructure
- Admin and configuration controls
This gives your revenue teams a platform that supports daily operations, not just isolated automation features.
C. Build AI Models That Billing Teams Can Trust
AI should help billing, coding, finance, and denial teams make faster decisions with better context. At the same time, it should not create black-box outputs that teams cannot verify.
Intellivon builds AI models with evidence, confidence scoring, review thresholds, and explainable recommendations so teams can understand why a claim, code, denial, or payment variance was flagged.
Your AI RCM platform can include:
- NLP extraction from clinical documentation
- LLM summarization for claim and appeal context
- Denial prediction models
- Coding support workflows
- CAC support
- Payment variance detection
- AR prioritization
- Confidence scoring
- Explainable AI recommendations
- Human review queues
Every AI workflow is designed to support revenue teams while keeping critical decisions reviewable and auditable.
D. Integrate With Healthcare Revenue Systems
AI revenue cycle management software depends on accurate data movement across clinical, payer, billing, and finance systems.
That is why Intellivon plans integrations early. At the same time, we help connect your platform with the systems needed to validate coverage, process claims, review documentation, submit transactions, track denials, post payments, and measure revenue performance.
We support integrations across:
- Epic
- Cerner / Oracle Health
- FHIR APIs
- HL7 CDA
- HL7 interfaces
- Clearinghouses
- EDI 837 workflows
- EDI 835 workflows
- Payer APIs
- Practice management systems
- Finance systems
- Data warehouses and BI tools
These integrations help your AI RCM platform move revenue workflows from patient access to claim submission, denial prevention, payment reconciliation, and executive reporting.
This helps your platform support enterprise healthcare buyers, hospital teams, payer-facing workflows, and regulated revenue operations with confidence.
Ready To Build Enterprise AI Revenue Cycle Management Software?
If you are planning to build enterprise AI revenue cycle management software, Intellivon can help you define the right roadmap before development begins.
We will help you identify the best RCM automation opportunities, map front-end, mid-cycle, and back-end workflows, plan EHR and payer integrations, design secure architecture, build explainable AI models, and create a scalable platform around real revenue outcomes.
Ready to build a controlled AI revenue infrastructure for your hospital or healthcare business? Contact Intellivon today to discuss your project.
Things To Know About Enterprise AI Revenue Cycle Management
Q1.How much does enterprise AI revenue cycle management software cost?
A1. Enterprise AI revenue cycle management software usually costs $150,000 to $450,000+ for a hospital-grade custom build. At the same time, a narrower MVP may sit near the lower range. A full platform with EHR integrations, clearinghouse workflows, denial prediction, coding support, HIPAA controls, and MLOps moves toward the higher range.
Q2. How long does it take to build AI revenue cycle software?
A2. A focused AI RCM MVP usually takes 4–6 months. At the same time, a production hospital platform takes 8–12 months, especially when it includes Epic or Cerner integration, EDI workflows, payer rules, LLM support, human review, HIPAA controls, and model monitoring.
Q3. Can HIPAA-compliant revenue cycle software use LLMs safely?
A3. Yes, HIPAA-compliant revenue cycle software can use LLMs safely when PHI controls, access rules, audit logs, BAAs, secure inference, data minimization, and human review are built into the architecture. At the same, LLMs should summarize, retrieve, and draft. They should not make unsupported billing decisions alone.
Q4. Build vs buy hospital RCM software: what is the decision rule?
A4. Buy when your workflows are standard, your volume is moderate, and vendor configuration solves the problem. At the same time, build when your payer mix, specialty rules, EHR environment, denial patterns, data ownership needs, or AI transparency requirements create strategic value that generic platforms cannot support.
Q5. Can AI denial management software development reduce denials without damaging data quality?
A5. Yes, AI denial management software can reduce denials when it uses governed data pipelines, payer-specific rules, confidence scoring, and human review. At the same time, buyers worry about no-code AI agents creating messy integrations, so the platform must prove data lineage, review logic, and auditability from day one.



