

Key Takeaways:
-
Healthcare data API development connects priority systems through FHIR R4 resources and HL7 v2 mapping.
-
API gateway setup, authentication, audit logs, terminology mapping, and consent rules are foundational requirements.
-
The first build excludes full HIE, deep EMPI cleanup, broad payer exchange, and every EHR workflow.
-
Focused first builds cost $50,000 to $150,000, covering priority healthcare system connections and standards-based APIs.
-
How Intellivon builds healthcare data APIs as controlled interoperability foundations that prove exchange value before expanding.
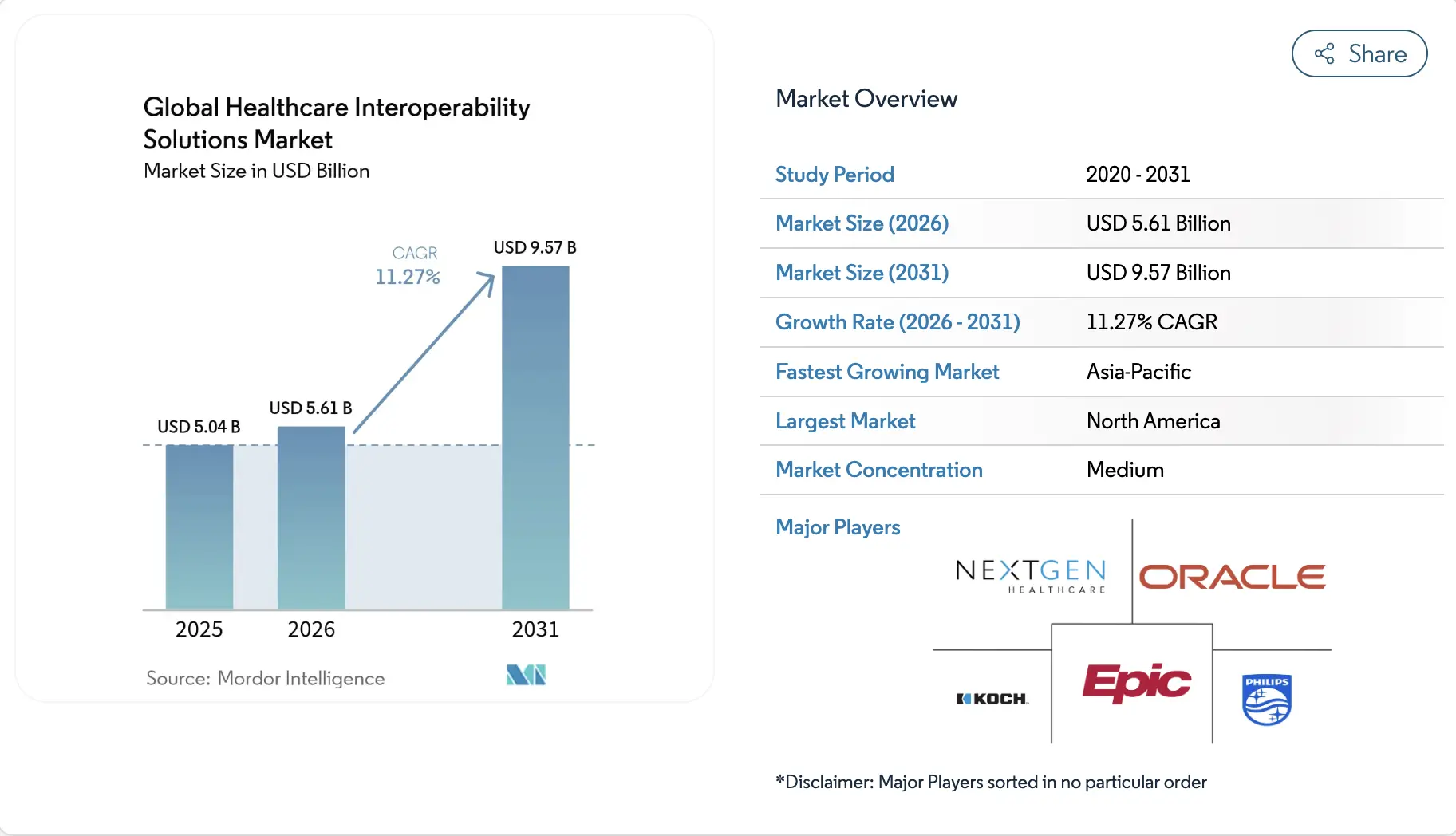
Building a healthcare data interoperability platform typically costs between $50,000 and $150,000 for an initial release. This budget can cover the main healthcare data API development layer. This includes FHIR architecture, some HL7 integration, API security, audit logs, basic terminology mapping, and compliance-ready access controls.
The final cost varies based on the number of systems you connect, the quality of your source data, and whether your EHR environment supports FHIR. A single-workflow build may lean toward $50,000. At the same time, A more robust production release with FHIR APIs, HL7 feeds, consent logic, monitoring, and testing will approach $150,000.
Many teams underestimate terminology normalization. So, if you do not plan for SNOMED CT, LOINC, and RxNorm mapping early on, the platform may transfer data but fail to make it useful for clinicians.
Intellivon builds these platforms around practical exchange needs, not oversized infrastructure. This blog outlines the cost by phase, helping you define the build clearly before selecting a development partner.
What is a Healthcare Data Interoperability Platform?
A healthcare data interoperability platform is a specialized software layer that connects separate clinical and financial systems. It standardizes fragmented data from Electronic Health Records (EHRs), laboratories, and insurance databases into unified, compliant formats like FHIR R4 or R5.
This infrastructure enables secure, automated data exchange between legacy networks and modern applications. For engineering leadership, it eliminates custom point-to-point connections, simplifies compliance, and establishes a single source of truth for clinical operations.
The Billion-Dollar Opportunity For Building Such a Platform
The global market for healthcare interoperability is expanding rapidly due to shifting federal rules and infrastructure modernization. Organizations that invest in custom platform development secure long-term scalable advantages. At the same time, the underlying financials reflect a highly profitable enterprise software sector.
1. Core Catalysts Accelerating Market Demand
Four critical regulatory and operational shifts are forcing enterprise health networks to rebuild their data exchange strategies immediately.
- Federal Compliance Mandates: The Centers for Medicare & Medicaid Services (CMS) interoperability rules require health plans to deploy standardized APIs. This includes specific mandates for automated prior-authorization data exchange.
- Value-Based Care Adoption: Accountable Care Organizations (ACOs) require real-time data from external labs, pharmacies, and clinics to accurately track patient outcomes.
- The Demand for AI-Ready Data: Enterprise AI agents and predictive clinical models require highly structured data. Legacy data formats must be converted into clean, standardized repositories before models can safely process them.
- National Interoperability Networks: The rollout of the Trusted Exchange Framework and Common Agreement (TEFCA) establishes strict nationwide frameworks for secure, cross-network clinical data sharing.
2. Direct ROI and Economic Benefits
Building a dedicated data integration platform directly improves an organization’s bottom-line performance across multiple distinct cost centers.
- Elimination of Redundant Testing: Real-time clinical data access prevents duplicate lab work and diagnostic imaging. This lowers the total cost of care within risk-bearing insurance contracts.
- Reduced Administrative Overhead: Eliminating manual phone calls, faxes, and custom scripts streamlines basic operations. Automated workflows greatly lower the cost of payer-to-provider data exchange.
- Enhanced Contract Reimbursements: Clean data pipelines allow health systems to close care gaps faster. This directly increases incentive payouts from value-based payer agreements.
[For a deeper breakdown of data architecture and compliance engineering, see our guide on How to Create an EHR-Agnostic Interoperability Layer].
3. Industry Benchmarks: Proven Market Leaders
Several enterprise platforms have validated this market model by achieving massive scale and deep integration across the healthcare ecosystem.
- 1upHealth: A cloud-native pioneer leveraging a modern per-call API pricing model to deliver low-cost FHIR interoperability at massive scale.
- InterSystems (HealthShare): A veteran player focused on heavy enterprise data ingestion and complex terminology mapping for massive hospital networks.
- Epic Systems & Oracle Cerner: The dominant legacy EHR vendors who have built internal API layers to support broader clinical data pipelines.
Building a healthcare data interoperability platform is a highly strategic, high-yield opportunity. Forced demand from federal rules combined with clear financial benefits makes it a necessity for modern healthcare enterprises.
To succeed, engineering teams must focus directly on cloud-native deployments, scalable FHIR R4 or R5 servers, and strict automated compliance controls.
What Healthcare Data API Development Costs at $50,000–$150,000
Healthcare data API development costs $50,000–$150,000 when scoped as a focused first build rather than an enterprise interoperability program.
This range supports priority API development, basic FHIR exchange, limited HL7 mapping, core security, audit logging, and a controlled launch for high-value workflows.
1. Phase Budgets and Exclusions
| Development Tier | Budget Range | Primary Focus | Key Exclusions |
| Foundational Pilot | $50,000–$80,000 | Single workflow, 1–2 data sources | HL7 ingestion, advanced mapping |
| Production Release | $80,000–$120,000 | 2–4 systems, basic normalization | Bulk data APIs, EMPI logic |
| Advanced Data Hub | $120,000–$150,000 | 3–5 systems, consent workflows | Full HITRUST, TEFCA network |
2. The $50,000–$80,000 Platform Scope
This foundational tier establishes an initial [healthcare data API development] footprint to validate data exchange workflows. It is designed for pilots, narrow partner data exchanges, or proof-of-concept builds connecting to standard data sources.
- Integrates 1–2 source systems.
- Supports 5–8 core FHIR R4 resources like Patient and Observation.
- Uses standard OAuth 2.0 or token-based authentication.
- Deploys a lightweight API gateway and basic logging.
3. The $80,000–$120,000 Platform Scope
This mid-tier range covers the [healthcare API platform development cost] for a stable, production-ready release. It supports digital health applications and specialty networks requiring active clinical data pipelines.
- Connects 2–4 separate source systems.
- Processes 8–15 FHIR R4 resources with API versioning controls.
- Implements light HL7 v2 ingestion for ADT messages.
- Features role-based access control and system alerting dashboards.
4. The $120,000–$150,000 Platform Scope
This scope manages custom healthcare interoperability software cost variables for larger networks handling live patient interactions. It provides a highly compliant architectural foundation that avoids future engineering dead ends.
- Ingests data across 3–5 disparate systems.
- Maps 15–25 FHIR resources and supports bulk data APIs.
- Integrates SMART on FHIR protocols and consent management.
- Applies basic patient matching algorithms for identity resolution.
5. Exclusions and Cost Drivers
This initial budget range cannot absorb nationwide network connectors or expensive enterprise data cleansing tools. The primary cost drivers moving budgets upward include data source variety, terminology mapping depth, and strict auditing mandates.
- Excludes enterprise master patient index (EMPI) architectures.
- Omits TEFCA, CommonWell, and Carequality network integrations.
- Defers specialized HITRUST or SOC 2 Type II certification auditing costs.
- Drives up the [API security cost healthcare] allocation when using zero-trust designs.
This cost range works only when the first platform has a strict boundary. Next, the architecture should show how a smaller build can still support future growth.
The Platform Architecture Behind a $50,000–$150,000 Build
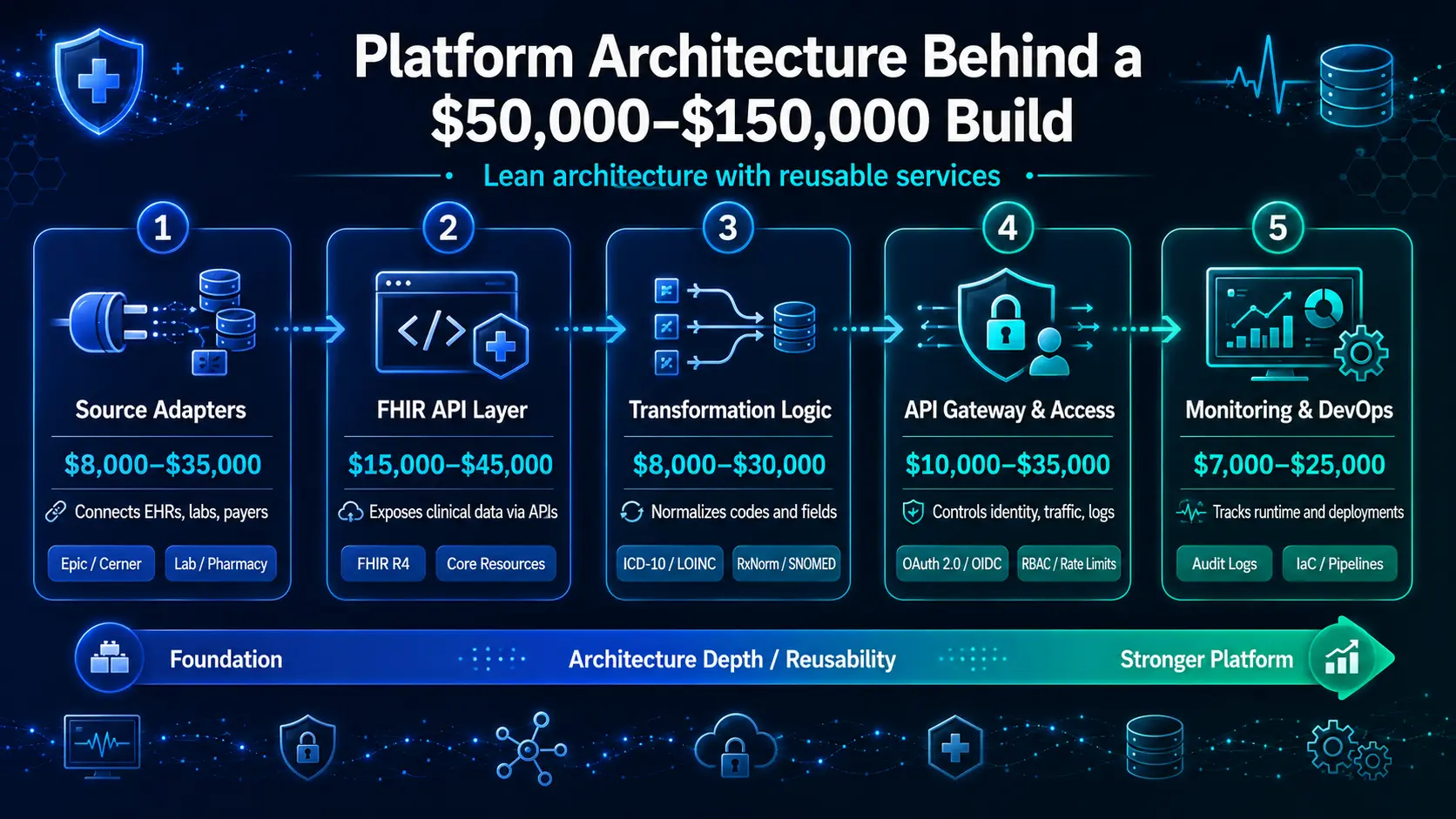
A $50,000–$150,000 healthcare interoperability platform needs a lean architecture with reusable services. The first build should include source adapters, a FHIR API layer, lightweight transformation logic, API security, audit logs, monitoring, and deployment workflows.
It should avoid overbuilding enterprise data warehouses, full EMPI programs, or large-scale HIE capabilities.
1. Layer-by-Layer Architectural Component Breakdown
| Layer Module | Estimated Budget | Primary Technical Responsibility | Core Architectural Standard |
| Source Adapters | $8,000–$35,000 | Ingest and translate unstructured system data | System-specific API connections |
| FHIR API Layer | $15,000–$45,000 | Expose clinical models via RESTful endpoints | RESTful FHIR R4 Specification |
| Transformation Logic | $8,000–$30,000 | Normalize incoming codes to standard tables | Unified Terminology Mapping |
| API Gateway & Access | $10,000–$35,000 | Manage routing, identity, traffic, and logs | OAuth 2.0 / OIDC Frameworks |
| Monitoring & Devops | $7,000–$25,000 | Provide runtime tracking and deployment pipelines | Immutable Log & Infrastructure-as-Code |
2. Source System Adapter Layer
The source system adapter layer connects the platform to EHRs, labs, payer systems, pharmacy tools, or partner databases. In a first build, this layer should stay limited to the highest-value systems because every new source adds mapping, testing, vendor coordination, and support cost.
- Covers endpoints for Epic FHIR API integration cost models, Cerner FHIR API cost controls, or specialized Meditech interoperability cost pathways.
- Manages dedicated athenahealth API integration interfaces alongside high-priority external data pipelines.
- Restricts connectivity to core channels like a targeted lab results exchange cost scope or a narrow pharmacy data integration cost footprint.
- Defers complex remote patient monitoring integration cost lines and unmapped digital health app integration cost requirements to future iterations.
Platform Cost Note: Allocate approximately $8,000–$35,000 specifically for source system adapter modules within the initial project structure.
Once systems connect, the platform needs a consistent API layer.
3. FHIR API and Resource Layer
The FHIR API layer exposes structured clinical data through standard resources that applications can read, write, or query. For the first build, the platform should support only the resources needed for the chosen workflow instead of trying to model the entire clinical record.
- Focuses development strictly on immediate FHIR R4 API development cost line items to maintain speed and predictability.
- Maps a concise set of five vital clinical profiles: Patient, Encounter, Observation, Condition, and MedicationRequest.
- Includes specialized financial objects such as Coverage, Claim, and ExplanationOfBenefit exclusively when building out active payer data workflows.
- Sets up structured search parameters and explicit schema validation rules while charting future FHIR R5 implementation cost trajectories.
Platform Cost Note: Budget around $15,000–$45,000 to cover primary FHIR server development cost components and core FHIR resource modeling cost tracks.
For a deeper look into structuring workflows, see our analysis on [AI Healthcare Claims Processing Software Development].
FHIR gives structure, but data still needs transformation before it becomes usable.
4. Lightweight Data Transformation Layer
The transformation layer converts source data into the platform’s canonical structure before exposing it through FHIR APIs or partner endpoints. In a first build, this layer should cover only priority fields, core code sets, and high-value workflow data.
- Restricts the initial healthcare data pipeline cost to essential message routing, payload parsing, and batch ingestion tasks.
- Coordinates simple data quality management cost metrics by dropping structural duplicates at the inbound API perimeter.
- Normalizes incoming demographic codes and local diagnostic findings through basic clinical data normalization cost frameworks.
- Connects translation engines to static dictionary sets including ICD-10 normalization, LOINC code mapping, RxNorm mapping, and SNOMED CT mapping fields.
Platform Cost Note: Plan an expenditure of $8,000–$30,000 for building this baseline ETL pipeline healthcare cost layer. Transformation must sit behind a secure access layer.
5. API Gateway, Security, and Access Layer
The API gateway controls how applications, users, and partners access healthcare data. This layer manages authentication, authorization, rate limits, versioning, audit logs, and API analytics. Even a small platform needs this layer because PHI exchange cannot depend on informal access rules.
- Restricts access requests to hardened industry-standard patterns using verified OAuth 2.0 and OpenID Connect protocols.
- Protects database memory boundaries against unexpected volume spikes by implementing mandatory API rate limiting cost structures.
- Enforces data access control protocols using strict role-based access control cost filters built into the routing controller.
- Generates live administrative visibility dashboards via integrated API analytics cost modules and clean API versioning cost pathways.
Platform Cost Note: Set aside $10,000–$35,000 to engineer this integrated API gateway healthcare cost and developer portal cost healthcare API foundation. After access is controlled, the system needs operational visibility.
6. Monitoring, Audit, and Deployment Layer
The monitoring and audit layer proves that the platform works safely in production. It tracks API usage, failed requests, latency, access events, mapping errors, uptime, and deployment changes. This layer prevents the first build from becoming an unsupported custom interface.
- Implements continuous background system scanning routines to capture critical monitoring and alerting cost exceptions.
- Records every active data interaction inside a tamper-proof repository to satisfy legal audit trail immutability cost rules.
- Displays transactional health and performance anomalies through a simplified integration analytics dashboard cost console.
- Utilizes standardized container setups to handle basic high availability cost interoperability and automated deployment cost interoperability platform steps.
Platform Cost Note: Dedicate a budget of $7,000–$25,000 to implement baseline disaster recovery interoperability cost plans and release management tools.
The architecture should stay lean, but it cannot be casual. Next, the standards layer decides how much FHIR, HL7, CDA, and payer exchange belongs in the first build.
FHIR, HL7, CDA, and Payer API Scope in the First Build
FHIR, HL7 v2, CDA, and payer APIs should be scoped separately because they create different costs. A $50,000–$150,000 build can support FHIR-first exchange with limited legacy mapping.
It cannot usually modernize every HL7 feed, parse every CDA document, and support full payer interoperability in one phase.
1. Core Data Standards and Budget Mapping
| Data Standard | Implementation Complexity | Cost Allocation Range | Ideal Use Case |
| FHIR R4 APIs | Native RESTful standard | $15,000–$45,000 | Modern web apps, patient access |
| HL7 v2 Feeds | Legacy pipe-delimited | $20,000–$50,000 | Real-time EHR event triggers |
| CDA Documents | Monolithic XML parsing | $10,000–$25,000 | Summaries of care, referrals |
| Payer & Claims | Financial validation | $25,000–$50,000 | Eligibility, prior-auth tracking |
2. FHIR R4 API Scope
FHIR R4 should be the default standard for the first platform because it supports modern API-based data exchange. The first release should focus on resources that directly support the selected workflow, such as patient demographics, encounters, observations, medications, conditions, practitioners, and coverage.
- Streamlines development pipelines by matching standard US Core implementation profiles out of the box.
- Deploys basic patient access API components alongside structured provider directory API endpoints.
- Embeds SMART on FHIR implementation cost variables to manage third-party app authentication safely.
- Defers complex CDS Hooks integration cost lines and intensive FHIR bulk data API cost elements unless they are critical for core day-one operations.
Scope Financial Note: Pure FHIR-only MVPs typically fit near a $50,000–$90,000 range when connecting to clean, modern source endpoints.
FHIR handles modern exchange, but hospitals still depend on older messaging.
3. HL7 v2 Scope
HL7 v2 should enter the first build only when the platform needs real-time feeds such as admissions, discharges, transfers, lab results, orders, or scheduling updates. Each HL7 feed adds mapping, routing, exception handling, and testing effort.
- Establishes dedicated socket connections to capture Admission, Discharge, and Transfer (ADT) data blocks.
- Processes transactional clinical results by mapping standard Observation Report (ORU) messaging strings.
- Coordinates background plumbing through a focused Mirth Connect implementation cost or Rhapsody integration cost track.
- Builds explicit error-queuing components and message-replay mechanics to prevent data loss during network drops.
Scope Financial Note: Integrating one or two tightly controlled HL7 feeds can fit inside an $80,000–$150,000 deployment budget.
Document exchange should be treated differently from real-time message exchange.
4. CDA Document Exchange Scope
CDA exchange should stay limited in the first build unless referral records, discharge summaries, or transition-of-care documents drive the core use case. Basic CDA storage is affordable. Structured extraction from CDA documents raises cost because documents vary across sending organizations.
- Minimizes initial software friction by storing raw XML files inside a secure clinical data repository.
- Indexes metadata fields including patient identifiers, author timestamps, and document types for basic search.
- Controls the [HL7 CDA document exchange cost] line by performing section-level parsing instead of deep narrative field extraction.
- Logs explicit data provenance parameters to maintain clear tracking of original medical records.
Scope Financial Note: Baseline CDA document indexing can fit near a $10,000–$25,000 scope, whereas granular data parsing should move to later phases.
Payer exchange adds another layer because payer APIs carry claims, coverage, and authorization data.
5. Payer and Claims API Scope
Payer APIs should be included only when the first build targets eligibility, coverage, prior authorization status, claims data, or payer-provider data exchange. These workflows need stricter validation because administrative data affects approvals, billing, reporting, and patient financial workflows.
- Manages targeted [payer-to-provider data exchange cost] structures to confirm real-time insurance validation.
- Connects administrative infrastructure to track automated claims data exchange cost lines.
- Minimizes manual utilization review bottlenecks by routing via a specific prior authorization API cost framework.
- Maps distinct financial FHIR resources like Coverage, Claim, and ExplanationOfBenefit directly to local billing tables.
Scope Financial Note: A highly focused, narrow payer API workflow can fit inside the $120,000–$150,000 tier if clinical scope remains highly limited.
Payer workflows increase compliance exposure, so they should not be added casually.
6. What Standards Should Be Deferred
The first build should defer standards or workflows that do not support the first business outcome. Full TEFCA participation, broad HIE connectivity, DICOM imaging exchange, large payer networks, and advanced FHIR Bulk Data exports can exceed the budget when included too early.
- Postpones the heavy [DICOM integration cost] and deep imaging data exchange cost pipelines to later development phases.
- Avoids early financial inflation by pushing out formal TEFCA participation cost and general Trusted Exchange Framework cost onboarding.
- Defers broad external networking paths like DirectTrust integration cost or general HIE connectivity cost hooks.
- Removes advanced data architecture tracks such as a full FHIR data lake architecture cost or complex event-driven architecture cost interoperability models.
The standards mix determines whether the budget stays realistic. The next section should turn that scope into a phase-by-phase cost breakdown.
Phase-by-Phase Healthcare API Platform Development Cost
Healthcare API platform development cost should be planned across discovery, architecture, API development, data mapping, security, testing, and deployment.
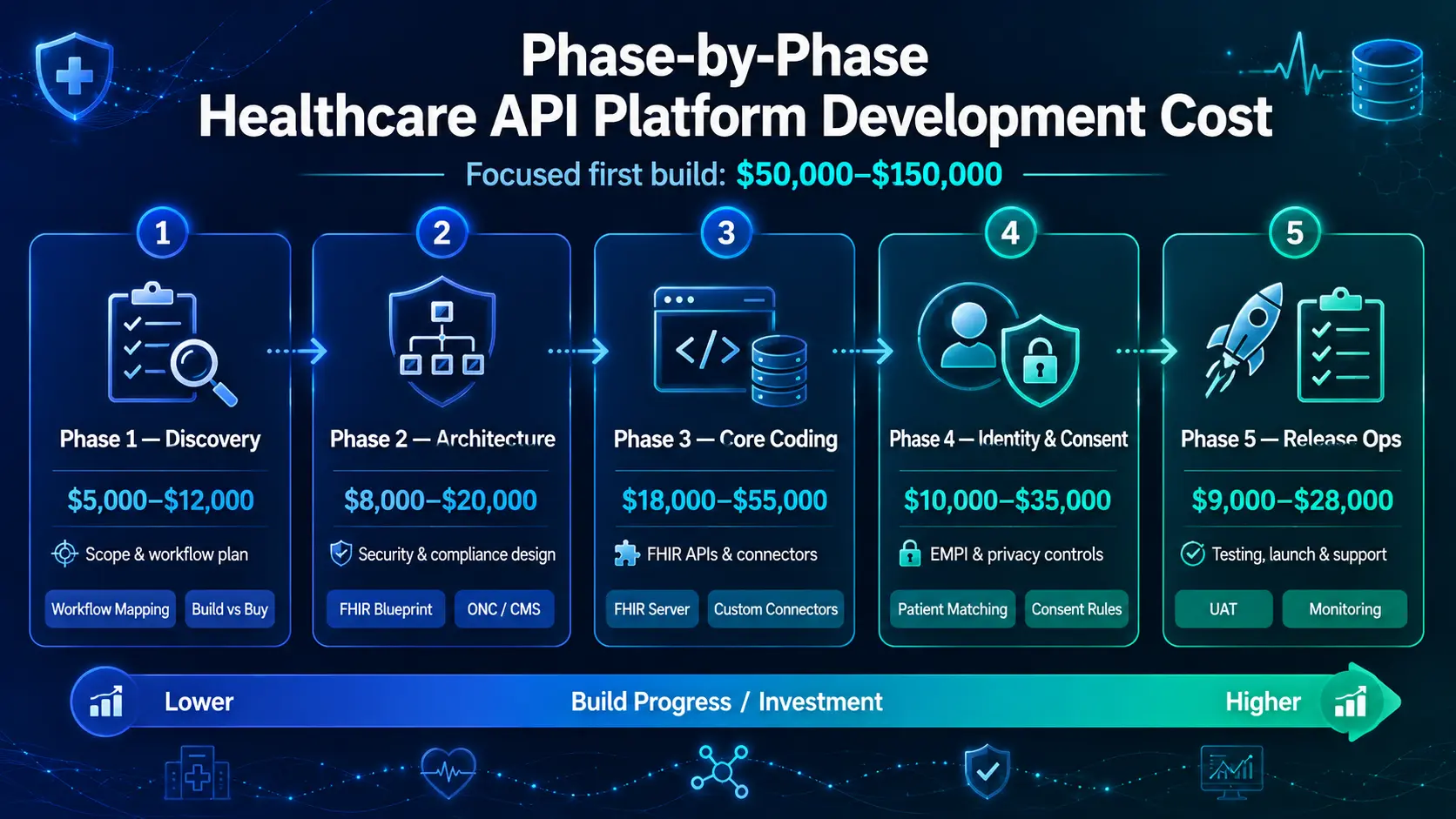
A controlled first build costs $50,000–$150,000 when each phase has a defined scope, acceptance criteria, and deferred-feature list before development begins.
Phase Budgets and Technical Deliverables
| Phase Name | Estimated Cost | Core Technical Milestone |
| Phase 1: Discovery | $5,000–$12,000 | Scoping matrix & build vs. buy framework |
| Phase 2: Architecture | $8,000–$20,000 | Security blueprint & ONC/CMS mapping |
| Phase 3: Core Coding | $18,000–$55,000 | Functional FHIR server & custom connectors |
| Phase 4: Identity & Consent | $10,000–$35,000 | Baseline EMPI engine & privacy filters |
| Phase 5: Release Ops | $9,000–$28,000 | UAT validation, automated pipelines, & support |
Phase 1 — Discovery and Platform Scope: $5,000–$12,000
Discovery usually costs $5,000–$12,000 for a focused interoperability build. This phase defines the first workflow, source systems, API users, data classes, compliance exposure, vendor access, success metrics, and exclusions. It prevents the project from expanding into a full enterprise platform too early.
- Documents detailed workflow mapping diagrams and complete source system inventory matrices.
- Performs comprehensive data access reviews alongside initial compliance checklist structuring.
- Formalizes explicit API consumer roles and analyzes current-state legacy interface parameters.
- Runs a thorough [build vs buy healthcare interoperability platform cost] review to build the first-release backlog.
After scope, architecture turns the plan into an engineering model.
Phase 2 — Architecture and Compliance Design: $8,000–$20,000
Architecture and compliance design usually costs $8,000–$20,000. This phase defines the API layer, FHIR resources, security model, data flows, hosting approach, audit requirements, consent logic, and future expansion path. It reduces rework by solving core design choices before development starts.
- Locks down the primary architecture design cost track and cloud environment selection framework.
- Generates clear API gateway layout blueprints and standalone FHIR server database schema designs.
- Configures advanced security architecture frameworks mapped directly to active HIPAA controls.
- Addresses long-term [ONC interoperability compliance platform cost] items and [CMS interoperability rule compliance cost] markers.
- Embeds explicit data access control cost definitions within the core technical routing logic.
For a deeper breakdown of data infrastructure design, see our guide on [AI Healthcare Claims Processing Software Development].
Once the architecture is approved, engineering can start with the most valuable exchange layer.
Phase 3 — API, FHIR, and Connector Development: $18,000–$55,000
API, FHIR, and connector development usually costs $18,000–$55,000 in the first build. This phase creates the endpoints, source adapters, data requests, response formats, error handling, authentication hooks, and documentation needed for real system exchange.
- Directs core resources to handle immediate FHIR interoperability platform development cost components.
- Purchases or builds foundational modules to cover the HL7 FHIR platform build cost allocation.
- Coordinates custom source adapters, structured error handling systems, and active endpoint controllers.
- Publishes machine-readable API documentation and builds a custom developer portal cost healthcare API framework.
- Assembles the base data plumbing layer under an isolated integration engine development cost pathway.
APIs need clean data mapping before users can trust the output.
Phase 4 — Data Mapping, EMPI, and Consent Logic: $10,000–$35,000
Data mapping, basic EMPI logic, and consent workflows usually cost $10,000–$35,000 in a first build. This phase makes exchanged data usable, traceable, and safe. The scope should stay limited to priority fields and core privacy rules.
- Manages core clinical data normalization cost variables across localized database structures.
- Standardizes data translations through a centralized, high-efficiency terminology mapping cost model.
- Launches a lightweight master patient index cost layout with basic duplicate record management.
- Embeds an explicit consent management platform cost module to handle patient consent workflow cost events.
- Isolates behavioral health data compliance fields via automated data segmentation for privacy cost filters.
After mapping and consent, testing determines whether the platform is ready for production.
Phase 5 — Testing, Deployment, and First-Year Support: $9,000–$28,000
Testing, deployment, and first-year support usually cost $9,000–$28,000 inside a $50,000–$150,000 platform. This phase validates data accuracy, access control, API behavior, audit trails, performance, source changes, and support workflows before the platform handles production traffic.
- Manages financial overhead for the active testing phase cost interoperability segment.
- Absorbs live infrastructure launch costs via a structured deployment cost interoperability platform budget.
- Runs high-volume API performance tests, isolated security evaluations, and final User Acceptance Testing (UAT).
- Implements automated regression tests alongside live system monitoring dashboards and support books.
- Supplies a foundational first-year maintenance plan to protect core operations.
A credible budget shows what each phase buys. Next, compliance must be built into the cost model instead of treated as a final checklist.
Compliance Controls That Shape HIPAA and ONC Platform Cost
A HIPAA-compliant interoperability platform development cost depends on how the platform protects PHI, manages access, stores audit logs, documents consent, and supports federal interoperability expectations.
A first build should include practical controls for HIPAA, CMS interoperability rules, ONC HTI-1 alignment, information blocking awareness, and secure partner access.
1. Compliance Domain Expense and Baseline Allocation
| Regulatory Focus | Base Compliance Driver | Practical Coding Cost | Mandatory Tech Control |
| HIPAA Security | 45 CFR Parts 160 & 164 | $8,000–$25,000 | AES-256 data-at-rest & TLS 1.3 transport |
| CMS Interoperability | CMS-0057-F Mandates | $5,000–$20,000 | FHIR Da Vinci CDex electronic prior-auth |
| ONC HTI-1 Rule | USCDI v3 Stand-up | $4,000–$15,000 | 13 evidence-based DSI source attribute fields |
| Sensitive Data Seg. | 42 CFR Part 2 Boundaries | $8,000–$30,000 | Granular consent engine & tagging tables |
| Audit & Assurance | Log Immutability | $5,000–$20,000 | Append-only write-once cryptographic logs |
2. HIPAA and PHI Security Controls
HIPAA controls should be part of the first build because the platform exchanges Protected Health Information (PHI) across systems. The core requirements include encryption, access control, user permissions, audit logs, backup policies, vendor agreements, and monitoring. Skipping these controls creates rework and legal exposure.
- Implements multi-layered data encryption interoperability cost provisions utilizing native AES-256-bit storage and TLS 1.3 transport structures.
- Configures fine-grained access filtering by accounting for realistic role-based access control cost application parameters.
- Validates vendor parameters by anchoring developer pipelines behind explicit BAA requirements interoperability vendors checklists.
- Keeps testing processes safe by utilizing isolated, strict production environment separation boundaries.
Compliance Financial Note: Plan an expenditure of $8,000–$25,000 to embed initial [PHI security interoperability platform] safety layers.
HIPAA protects data. ONC and CMS influence exchange behavior.
3. CMS Interoperability Rule Readiness
CMS interoperability rule readiness matters when the platform supports payer access, patient access, provider access, prior authorization, or coverage data exchange. The first build should map which CMS API expectations apply now and which belong in future phases.
- Directs core resources to address the urgent [CMS interoperability rule compliance cost] guidelines.
- Resolves automated clinical data tracking demands to handle the latest [patient access API compliance cost] frameworks.
- Integrates standardized HL7 FHIR Da Vinci Clinical Data Exchange (CDex) workflows to support modern electronic prior-authorization guidelines.
- Standardizes outbound payloads by aligning local financial resources with strict payer interoperability compliance cost parameters.
Compliance Financial Note: Dedicate a budget of $5,000–$20,000 for CMS readiness in a focused payer or patient access build.
ONC rules matter when certified health IT and information access are involved.
4. ONC HTI-1 and Information Blocking Readiness
ONC HTI-1 and information blocking readiness should shape API documentation, access policies, data availability, and technical restrictions. The platform should avoid unnecessary barriers to appropriate data sharing while still enforcing privacy, security, and role-based access.
- Integrates the mandatory US Core Data for Interoperability (USCDI v3) standard directly into core data schemas.
- Handles explicit algorithm transparency parameters by exposing the 13 required evidence-based Decision Support Intervention (DSI) fields.
- Allocates coding resources to handle specific [ONC interoperability compliance platform cost] fields and exception-logging mechanisms.
- Prevents financial penalties by eliminating arbitrary data export delays to support modern [information blocking compliance cost] requirements.
Compliance Financial Note: Allocate $4,000–$15,000 to complete initial ONC framework mapping and runtime error verification blocks.
Some privacy domains need stronger segmentation than general medical data.
5. 42 CFR Part 2 and Sensitive Data Segmentation
42 CFR Part 2 and sensitive data segmentation increase cost when the platform exchanges substance use disorder, behavioral health, reproductive health, or other restricted data. These workflows need granular consent, data tagging, role restrictions, and audit-proof.
- Integrates specific database structures to absorb the complex [42 CFR Part 2 compliance cost] rules.
- Builds precise tag filters to isolate sensitive substance use disorder data compliance records at the ingestion perimeter.
- Enforces explicit purpose-of-use constraints across the core [data segmentation for privacy cost] layer.
- Programs dynamic real-time validation triggers to process behavioral health data compliance checkmarks and instant consent revocations.
Compliance Financial Note: Budget around $8,000–$30,000 if your core initial production release must manage sensitive patient cohorts.
Compliance also depends on how the platform proves every action later.
6. Audit Logs, Pen Testing, SOC 2, and HITRUST Planning
Audit and assurance costs depend on how formal the first release must be. Basic audit logging should be included in every platform. SOC 2, HITRUST, and deep penetration testing may be planned early but executed in later phases if the budget is limited.
- Directs engineering resources to cover basic [audit trail immutability cost] parameters via cryptographic, append-only database schemas.
- Outlines strict access log retention parameters to preserve a clear record of administrative and partner interactions.
- Schedules the necessary groundwork for future, large-scale [penetration testing cost interoperability] assessments.
- Defers the heavy documentation expenses tied to a full [SOC 2 compliance cost] or [HITRUST certification cost interoperability] audit.
Compliance Financial Note: Plan a baseline budget of $5,000–$20,000 to implement standard system assurance trails.
Compliance is not separate from architecture. It changes which APIs can exist, who can access them, and what evidence the platform must preserve.
Data Normalization, EMPI, and Consent Costs Inside the Platform
Data normalization, EMPI, and consent costs decide whether the platform exchanges useful data or just moves messy records faster. A $50,000–$150,000 build can support basic mapping, limited patient matching, and first-stage consent logic. Deep enterprise cleanup should be planned as a later phase.
1. Ingestion Logic and Data Cleansing Allocations
| Processing Engine | Budget Range | Primary Technical Target | Key Technical Limitation |
| Data Normalization | $8,000–$30,000 | Convert string outputs to standard shapes | Restricts schema filters to 25 fields |
| Terminology Engine | $7,000–$25,000 | Map cross-system medical code spaces | Uses static dictionary lookups only |
| Baseline EMPI | $8,000–$30,000 | Match demographic keys across EHRs | Relies on deterministic rule trees |
| Consent Controller | $7,000–$25,000 | Enforce opt-in/opt-out payload gates | Excludes real-time element redaction |
| Provenance Tracking | $5,000–$18,000 | Stamp metadata origins onto payloads | Limits tracking to base system IDs |
2. Clinical Data Normalization Scope
Clinical data normalization turns source-specific fields into consistent, usable data. The first build should normalize only the data needed for the selected workflow. Trying to normalize the entire clinical record within $150,000 usually creates budget pressure and delays launch.
- Integrates baseline [clinical data normalization cost] elements directly into the inbound pipeline controller.
- Establishes strict data quality management cost metrics by enforcing basic structural schema checking.
- Manages the foundational [healthcare data pipeline cost] to handle incoming JSON and XML payloads.
- Designs a lightweight ETL pipeline healthcare cost module to parse, clean, and validate core data fields.
- Supports both real-time data exchange cost rules and batch data integration cost schedules without adding data warehouse overhead.
Operational Cost Note: Allocate $8,000–$30,000 to implement this focused field-level validation and error-flagging framework.
Normalization becomes harder when code systems vary across sources.
3. Terminology Mapping Scope
Terminology mapping should focus on the codes that directly support the first workflow. A medication workflow may need RxNorm. At the same time, a lab workflow may need LOINC. Additionally, a diagnosis workflow may need ICD-10 and SNOMED CT. Mapping every code set at once exceeds the first-build scope.
- Budgets the necessary [terminology mapping cost] to translate disparate source values into common terminology sets.
- Connects active code translation modules to handle standard SNOMED CT mapping cost rules for clinical findings.
- Embeds explicit LOINC code mapping cost parameters to support clean laboratory and diagnostic results exchange.
- Standardizes medication records by linking system libraries to clear RxNorm mapping cost pathways.
- Manages basic [ICD-10 normalization cost] targets to align diagnostic tracking across provider boundaries.
Operational Cost Note: Plan an expenditure of $7,000–$25,000 for first-stage terminology mapping and local code dictionary normalization.
After data has meaning, the platform must know which patient record it belongs to.
4. Basic EMPI and Patient Matching Scope
Basic EMPI logic helps match patient records across connected systems. A first build can support deterministic matching, simple duplicate flags, and manual review queues. At the same time, full probabilistic matching and large-scale duplicate cleanup usually need a later budget.
- Balances the core master patient index cost allocation by focusing exclusively on high-confidence demographic fields.
- Deploys a lean enterprise master patient index EMPI cost module that reads names, dates of birth, and genders.
- Implements a strict [patient matching algorithm cost] using deterministic if-then rule configurations.
- Handles basic duplicate record management cost needs by routing unverified records to a manual review queue.
- Links separate Medical Record Numbers (MRNs) across connected electronic health record instances without merging databases.
Operational Cost Note: Budget around $8,000–$30,000 for building this baseline record linkage and identity verification engine.
Even correctly matched data still needs consent controls.
5. Consent Management Scope
Consent management controls whether a user, app, or partner can access a specific type of data. A first build should support simple consent rules, role-based visibility, purpose-of-use logic, and audit logs. More advanced segmentation can follow after launch.
- Absorbs the core [consent management platform cost] inside the secure network perimeter.
- Programs an automated [patient consent workflow cost] to document electronic opt-in or opt-out selections.
- Enforces data access control cost parameters at the API router layer to protect sensitive information.
- Connects explicit [data segmentation for privacy cost] tags to block unauthorized document discovery.
- Captures real-time consent revocation events and records purpose-based access permissions within the system log.
Operational Cost Note: Plan a target budget of $7,000–$25,000 for this first-release consent and privacy gating foundation.
Consent needs a clear governance rule when different sources disagree.
6. Data Provenance and Clinical Truth Rules
Data provenance records where each data element came from, when it arrived, and which system supplied it. This helps teams resolve conflicting medications, allergies, diagnoses, lab values, or demographics. Even a small platform needs source visibility to prevent unsafe automation.
- Codes explicit source-of-truth rules to determine which system takes priority when data elements conflict.
- Attaches immutable provenance metadata directly onto every processed FHIR resource object.
- Generates clear system conflict flags when multi-source demographics or medication records overlap.
- Assembles a lightweight manual reconciliation queue to let clinical analysts review data contradictions safely.
- Affixes data confidence labels and preserves an active change history to build clean, compliant evidence chains.
Operational Cost Note: Budget $5,000–$18,000 to map baseline source priority matrices and provenance fields.
This layer makes the platform clinically useful. Without it, the APIs may technically work but still deliver confusing or unsafe data.
What Should Stay Out of the First $150,000 Build?
The most important unanswered buyer question is what the first interoperability platform should refuse to exchange.
A $50,000–$150,000 build succeeds when leaders define a minimum viable exchange boundary. This means choosing which systems, data classes, users, and workflows enter phase one, and which intentionally wait.
1. Phase-One Strategic Exclusion Framework
| Exclusion Focus | Core Technical Asset | Alternative Strategy | Primary Risk If Included |
| Data Scope | Full imaging and narrative notes | Section-level metadata parsing | Severe mapping delays |
| Integrations | Comprehensive multi-EHR networks | Single primary clinical connector | Exploding vendor support overhead |
| Access Model | Public developer marketplace | Hardened static API partner keys | Expanded security threat surface |
| Intelligence | Autonomous AI agent routing | Human-in-the-loop validation | Regulatory compliance exposure |
2. Exclude Low-Value Data Classes First
The first build should exclude data classes that do not support the target workflow. If the platform supports care gap outreach, it may not need imaging data. At the same time, if it supports eligibility checks, it may not need full clinical notes. Scope discipline protects the budget.
- Evaluates data utility strictly by checking if the specific attribute directly impacts the immediate transactional outcome.
- Eliminates heavy unstructured payloads that require custom, multi-layered natural language processing models.
- Minimizes downstream engineering burdens by filtering out raw, non-critical medical device telemetry.
- Postpones the integration of deep historical archive data, legacy unstructured clinical summaries, and full imaging data exchange workflows.
- Consequently, developers can focus entirely on high-yield, structured demographic and foundational clinical blocks.
Data classes are only one boundary. Systems also need limits.
3. Limit Source Systems to the Highest-Value Connections
The first build should connect the fewest systems needed to prove operational value. Each additional EHR, lab, payer, pharmacy, or device platform adds vendor coordination, data variation, testing effort, and monitoring requirements. At the same time, more systems rarely make the first build safer.
- Restricts initial ingestion endpoints to the cleanest, most accessible native API sources available.
- Prioritizes connections with low vendor friction and well-documented transport sandboxes.
- Standardizes initial data logic by deploying one primary electronic health record connector alongside one lab network.
- Deers complex multi-facility rollouts, external pharmacy hubs, and remote patient monitoring integration cost lines.
- Therefore, the engineering team establishes an ironclad, repeatable data pipeline without triggering compounding architectural bottlenecks.
After systems, the team must choose which API consumers get access.
4. Restrict API Consumers in Phase One
The first build should limit API consumers to known applications, users, or partners. Public developer access, third-party app ecosystems, and broad partner onboarding increase security, documentation, support, and monitoring costs. At the same time, controlled consumers reduce risk.
- Limits gateway registration boundaries to explicitly named internal systems and verified corporate partners.
- Enforces strict, static role assignments via a pre-configured role-based access control cost layer.
- Replaces complex multi-tenant onboarding paths with a simple, manually managed API key distribution protocol.
- Postpones the deployment of an open developer portal cost healthcare API infrastructure element.
- Subsequently, the platform reduces immediate security monitoring overhead while maintaining a clean, highly defensible perimeter.
A smaller access model makes compliance easier.
5. Defer Advanced AI Until the Data Layer Works
Advanced AI should not dominate the first build unless the workflow specifically needs it. Patient matching support, data quality detection, and basic NLP can help. However, predictive models, clinical summarization, and autonomous workflow routing need clean data, governance, and review processes first.
- Restores technical balance by positioning AI tools as helpful infrastructure helpers rather than decision makers.
- Utilizes narrow machine learning models strictly to surface real-time terminology mapping cost recommendations.
- Implements background data anomaly detection rules to catch broken payloads before they corrupt downstream storage.
- Defers complex clinical summarization engines, predictive risk scoring modules, and autonomous prior authorization API cost routing tools.
- In addition, this approach keeps the platform grounded in usable data, not unverified AI promises.
This keeps the platform grounded in usable data, not AI promises.
6. Use a “Phase-One Refusal List” in the Blog
A phase-one refusal list gives CTOs a practical governance tool. It states what the first build will not exchange, automate, expose, or certify. This section will make the article more original because competitors rarely help buyers say no before development begins.
Furthermore, applying this tool forces immediate alignment across clinical, administrative, and engineering teams.
| Do Not Include in Phase One | Why It Should Wait | Future Phase Trigger |
| Full EMPI Cleanup | Demands excessive, custom data quality management cost overhead | When core transactional data validation rates hit 98% |
| Full HIE Connectivity | Triggers massive, multi-vendor coordination and governance hurdles | After local provider-to-provider data exchange cost targets stabilize |
| Deep CDA Extraction | Document variation creates extreme string parsing friction | When specific document workflows demonstrate explicit operational ROI |
| Public Developer Portal | Creates unsustainable administrative, support, and security burdens | When external partner connection demand crosses ten active integrations |
| Full AI Decisioning | Requires perfectly cleaned, highly governed clinical data lakes | After a validated, fully audited clinical training dataset exists |
For an architectural guide on structuring these deferred engineering modules, see our comprehensive guide HIPAA-Compliant AI Healthcare App Development
This section gives the target reader a decision tool, not just information. It also protects Intellivon’s positioning by showing practical judgment.
Healthcare Interoperability Platform TCO and ROI
A healthcare interoperability platform total cost of ownership includes the first build, cloud services, API monitoring, vendor changes, support, security updates, terminology updates, and future integration waves.
Consequently, a $50,000–$150,000 build should also show ROI through faster data access, reduced manual work, and reusable exchange infrastructure. Therefore, enterprise leaders must evaluate long-term financial commitments alongside immediate operational advantages.
1. Amortized Ownership and System Return Targets
| Financial Component | Annual Budget Metric | Core Operational Driver | Primary Return Source |
| First-Year TCO | Build + 15%–25% overhead | Baseline licensing and cloud scaling | Automated chart retrievals |
| Ongoing Maintenance | 18%–30% of base build cost | FHIR versioning and patching updates | [Duplicate testing reduction ROI] |
| Workflow Expansion | $5,000–$80,000 per module | New EHR endpoints and AI data logic | Deep [care gap closure cost] drops |
2. First-Year TCO Model
First-year TCO includes the initial build plus cloud hosting, monitoring, support, security reviews, and small enhancement work. For a $50,000–$150,000 platform, first-year TCO usually adds 15%–25% above build cost if the release remains focused. Furthermore, calculating this total requires engineering teams to compile multiple hidden hosting and management layers early.
- Hosting Infrastructure: Covers baseline costs for cloud components like an API gateway, a dedicated FHIR server, and an integration engine.
- System Observability: Funds high-performance application logs and continuous background performance monitoring tools.
- Operational Support: Secures dedicated developer support hours to handle ongoing vendor API adjustments and minor terminology mapping updates.
Subsequently, engineering leads can stabilize the immediate post-launch ecosystem without running out of capital.
3. Ongoing Maintenance Cost
Ongoing maintenance usually costs 18%–30% of the initial build per year. For a $50,000 build, annual maintenance may run $9,000–$15,000. Meanwhile, for a $150,000 build, annual maintenance may run $27,000–$45,000. Therefore, software infrastructure should never be treated as a static expense after deployment.
- Security Patching: Delivers continuous software security updates to protect the data gateway against evolving cyber threats.
- API Versioning: Manages regular API version updates and handles sudden, breaking vendor electronic health record schema updates.
- Data Integrity: Validates ongoing custom FHIR profile updates via rigorous regression testing routines to avoid payload delivery errors.
Consequently, maintaining an active, error-free platform requires structured engineering oversight.
4. ROI Sources for the First Build
ROI should come from specific workflow improvements, not vague interoperability claims. The first platform may reduce manual chart retrieval, duplicate data entry, referral delays, eligibility checks, lab result chasing, partner onboarding time, or reporting work. Accordingly, applying a clear interoperability ROI calculation helps teams justify the initial infrastructure capital.
- Clinical Workflow Efficiency: Drives a major [clinical workflow efficiency ROI] step by eliminating tedious, manual telephone calls and fax communications.
- Care Coordination Savings: Yields fast [care coordination cost savings] across risk-bearing contracts by terminating unneeded, repetitive medical procedures.
- Population Health Performance: Lowers the total [population health integration cost] by feeding standardized clinical data straight into administrative reporting systems.
Thus, health networks can fast-track their value-based care interoperability cost recovery through automated quality measure reporting cost metrics.
5. Expansion Cost After the First Build
Expansion cost depends on whether the first build created reusable services. Adding one new FHIR resource may be inexpensive. Meanwhile, adding a new EHR, payer, consent model, or terminology domain costs more because each introduces mapping, testing, and governance work. Therefore, the architectural baseline dictates your future development speed.
- New EHR System Integration: Requires an allocation of $15,000–$60,000 depending on endpoint customization parameters.
- New Real-Time HL7 Feed: Costs $8,000–$30,000 to cover custom socket routing and Mirth exception scripting.
- Advanced AI Agent Workflows: Demands $20,000–$80,000 to construct highly accurate clinical data extraction logic.
Subsequently, building on top of a highly modular core reduces the cost of adding extra partner applications.
6. Board-Level Budget Message
The board-level message should state that $50,000–$150,000 funds a controlled first interoperability build, not a finished enterprise exchange network. The goal is to prove one valuable exchange workflow, create reusable infrastructure, and reduce risk before larger funding rounds. In addition, framing this narrative transparently ensures sustainable stakeholder support.
Meanwhile, this precise phrasing protects engineering teams from scope creep. TCO clarity helps prevent underfunding after launch. It also helps readers compare custom builds against managed platforms.
Build vs Buy Healthcare Interoperability Platform Cost
A build vs buy healthcare interoperability platform cost analysis depends on whether the organization needs speed, control, customization, or long-term ownership. Buying can work for standard exchange.
Building makes sense when workflows need custom data mapping, consent logic, payer integration, AI-ready pipelines, or reusable healthcare data infrastructure. Consequently, leadership teams must match their engineering talent to long-term licensing trajectories.
1. Procurement and Engineering Vector Analysis
| Procurement Vector | Time-to-Market Window | Initial Capex Range | 5-Year Amortized Friction |
| Pure Commercial Buy | 30 to 60 Days | Low upfront, high license fees | Drastic vendor lock-in overhead |
| Pure Custom Build | 6 to 9 Months | $50,000–$150,000 baseline | Gradual internal debt absorption |
| Cloud-Native Hybrid | 90 to 120 Days | $35,000–$95,000 baseline | Highly predictable data scaling |
| Native EHR Utility | 15 to 30 Days | Near zero infrastructure fees | Severe multi-source blockages |
2. When Buying Is Better
Buying is better when the organization needs standard FHIR access, basic patient access APIs, simple EHR connectivity, or fast compliance support. This route can reduce launch time because the vendor already provides core infrastructure, documentation, and managed service operations.
Furthermore, it protects thin software squads from spending months constructing commodity network pipes.
- Delivers immediate, out-of-the-box compliance profiles targeting standard patient access rules.
- Offloads continuous schema security patch management to dedicated vendor engineering centers.
- Eliminates heavy internal server monitoring requirements by shifting runtime burdens outwards.
- Avoids the need to hire specialized, niche healthcare integration specialists early in the cycle.
- Consequently, teams can launch basic connectivity pipelines within fixed, highly predictable procurement cycles.
Buying becomes less attractive when workflow control matters.
3. When Building Is Better
Building is better when the platform must support custom workflows, multiple source systems, payer-provider exchange, consent rules, AI readiness, or data ownership. A custom build gives the team more control over architecture, integration logic, governance, and future expansion.
Meanwhile, it prevents recurring, per-user subscription fees from eating away at long-term operating margins.
- Establishes direct structural control over core enterprise health data interoperability cost centers.
- Tailors internal record matching rules by applying a highly specialized, custom patient matching algorithm.
- Protects strategic software intellectual property by keeping all clinical translation assets fully in-house.
- Supports advanced, non-standard workflow hooks linking local legacy databases to multi-tenant user portals.
- Therefore, a controlled first custom build can fit comfortably within a strict $50,000–$150,000 budget boundary.
Many teams should not choose a pure build or pure buy model.
4. When Hybrid Is Best
Hybrid is best when the team wants faster launch without giving up control. This may combine managed cloud healthcare services, open-source integration engines, custom APIs, and internal data governance.
It is often the strongest option for a $50,000–$150,000 first build. Furthermore, this architectural strategy bypasses foundational storage engineering.
- Leverages production-ready data stores like Azure Health Data Services or AWS HealthLake instances.
- Processes complex, pipe-delimited legacy streams by embedding a highly stable Mirth Connect engine layer.
- Constructs specialized translation logic around native Google Cloud Healthcare API schemas.
- Merges custom local consent rules directly into enterprise cloud gateway configurations.
- Subsequently, developers spend zero time building base databases and focus entirely on higher-value data transformations.
The platform should also be compared against doing nothing or relying only on EHR-native APIs.
5. When EHR-Native APIs Are Enough
EHR-native APIs may be enough when the workflow needs limited read access, one EHR, and standard resource coverage. This is often the lowest-cost route. However, it can become limiting when the organization needs cross-system normalization, patient matching, payer exchange, or AI-ready data.
In addition, it restricts external software utility to the limits of a single vendor’s schedule.
- Extracts standard clinical profiles including demographics, simple medication lists, and vital signs.
- Minimizes initial infrastructure investments by executing queries straight against existing Epic or Cerner endpoints.
- Services basic, read-only digital health application utilities with minimal engineering friction.
- Fails immediately when forced to consolidate data across competing provider environments.
- Accordingly, this option can sit below $50,000 when the transaction scope remains extremely narrow.
Choosing between building and buying hinges entirely on your need for architectural control versus speed to compliance. Managed platforms solve standard exchange quickly, but custom builds protect proprietary data pipelines and eliminate heavy recurring licensing fees.
Balancing your long-term roadmap against upfront resources keeps development agile without introducing vendor lock-in.
Build a Healthcare Data API Platform With Intellivon
Intellivon helps healthcare teams build secure healthcare data API platforms that connect EHRs, labs, payers, patient apps, and external partners.
At the same time, a focused first build usually costs $50,000–$150,000, depending on FHIR scope, HL7 integration, terminology mapping, consent workflows, audit controls, and deployment needs.
A. Start With the First Data Exchange Problem
Intellivon begins by defining the exact workflow your platform must support first. This could be patient access, lab result exchange, payer data sharing, referral data, care gap reporting, or provider-to-provider exchange. This keeps the build focused, useful, and easier to approve.
B. Design the FHIR and Integration Architecture
The team designs the platform around FHIR R4/R5 APIs, HL7 feeds, API gateways, authentication, access controls, and monitoring. This helps you avoid one-off integrations that work for one use case but become expensive when new systems or partners are added.
C. Build Data Normalization Into the Platform
Intellivon treats terminology mapping as part of the core build. SNOMED CT, LOINC, RxNorm, ICD-10, and local code mapping are planned early so the platform does more than move data. It makes the data usable for clinical, operational, and reporting workflows.
D. Add Compliance Controls Before Launch
The platform is built with HIPAA-ready access controls, audit logs, encryption, consent logic, API security, and role-based permissions. For payer or patient access use cases, Intellivon also maps the build against CMS and ONC interoperability requirements before deployment.
E. Prepare the Platform for Future AI and Analytics
Once the data layer is clean and governed, the platform can support future AI and analytics use cases. These may include patient matching, care gap detection, clinical summarization, prior authorization evidence retrieval, risk scoring, and population health reporting.
Talk to Intellivon to scope your healthcare data API development roadmap, estimate your first-build cost, and define the FHIR, HL7, compliance, and data normalization layers before development begins.
Conclusion
Healthcare data API development is a practical infrastructure investment, not just a technical upgrade. A focused platform can connect EHRs, labs, payers, and care tools through secure FHIR APIs, HL7 integration, terminology mapping, consent controls, and audit-ready workflows.
When teams scope the build clearly, they can control cost, protect compliance, improve data usability, and create a foundation for future analytics, automation, and better clinical decisions.
Things To Know About Healthcare Data API Development
Q1. What is the healthcare data interoperability platform build cost for an MVP?
A1. The healthcare data interoperability platform build cost for an MVP usually sits between $50,000 and $90,000. This range works when the platform connects one primary system, supports limited FHIR resources, and validates one high-value workflow. Therefore, teams can prove exchange value before funding broader integrations, deeper mapping, and enterprise controls.
Q2. What is the FHIR interoperability platform development cost?
A2. FHIR interoperability platform development cost usually ranges from $50,000 to $120,000 for a focused first build. However, the budget increases when the platform needs custom FHIR profiles, SMART on FHIR, CDS Hooks, Bulk Data APIs, payer resources, or detailed conformance testing. These choices expand architecture, mapping, and validation work overall.
Q3. How long does healthcare data API development take?
A3. Healthcare data API development usually takes 8 to 16 weeks for a focused first build. A $50,000 to $80,000 project may take 8 to 10 weeks. Meanwhile, a $120,000 to $150,000 build with HL7, consent, mapping, testing, and deployment support may need 12 to 16 weeks for safer launch planning.
Q4. What is the best build vs buy healthcare interoperability platform cost rule?
A4. Buy when the workflow is standard, and the vendor already supports it. Build when you need custom mapping, consent logic, payer exchange, AI-ready data, or long-term ownership. However, choose hybrid when you need managed infrastructure for speed and custom workflow logic for control, integration depth, and future expansion in later phases.
To Sum Up:
- A $50,000–$150,000 healthcare interoperability build should not promise full enterprise exchange. It should prove one valuable workflow with reusable architecture.
- FHIR reduces integration friction, but it does not remove the cost of HL7 mapping, terminology normalization, consent, audit logs, and testing.
- The most strategic first-build decision is what the platform refuses to exchange. Scope control protects both budget and compliance.
- Annual maintenance should be planned at 18%–30% of the initial build because APIs, mappings, standards, and vendor systems keep changing.
- AI should come after the platform can deliver clean, governed, traceable healthcare data. Otherwise, models amplify integration problems instead of solving them.



