Key Takeaways:
-
AI prior authorization platforms require six development stages from workflow mapping to deployment.
-
The platform must pull clinical data at order entry and apply payer-specific criteria automatically.
-
FHIR R4, EHR integration, and X12 278 transactions are non-negotiable technical requirements for ePA.
-
CMS-0057-F compliance demands audit trails, explainable AI, and human review workflows throughout.
-
How Intellivon builds AI prior authorization platforms from payer-criteria mapping through production deployment.
Prior authorization systems in hospitals have run into roadblocks because of the incompetent workflows set in place by traditional software. What has changed is the infrastructure required to solve it, which is payer-specific criteria that update quarterly, FHIR Prior Authorization APIs that CMS now mandates, clinical documentation requirements that vary by procedure and plan, and real-time decision timelines that manual review cannot meet.
Building a custom AI prior authorization platform is the decision organizations reach when their PA volume, payer mix, or product requirements have outgrown traditional software systems.
At Intellivon, we build AI prior authorization platforms as healthcare infrastructure, starting with payer-criteria mapping and clinical workflow discovery before any architecture decisions are made. This blog post draws from our experience and covers how we build such platforms, from start to finish.
What Is an AI Prior Authorization Platform?
An AI prior authorization platform is healthcare software that automates the entire PA process. It detects authorization requirements at order entry, assembles clinical evidence, and submits requests through the right payer channels. At the same time, the platform tracks decisions in real time and flags denial risks before a claim leaves the system.
A. What PA Means in Provider and Payer Workflows
Prior authorization is an approval process that health insurance companies (payers) use to control costs. Here, doctors (providers) must prove that a planned treatment or medical test is truly necessary before the insurance company agrees to pay for it. This process forms a core part of utilization management, which is how insurance companies review medical care to ensure it matches their official coverage rules.
To get this approval, clinic staff spend hours tracking down patient details and matching them to complex rule engines. This administrative burden slows down operations and introduces specific risks across the clinical timeline:
- Workflow disruptions: Administrative staff must stop their daily tasks to search for specific medical rules, fill out long forms, and fax records to different insurance companies.
- Timeline mismatches: Staff must manually sort and track urgent vs standard authorization paths to ensure life-threatening cases get fast approval while standard orders wait in line.
- Care delays: Patients frequently face long wait times to start critical treatments while the hospital waits for the insurance company to return an approval stamp.
B. AI Prior Authorization Platform Vs Traditional PA Software
Traditional prior authorization software works like an electronic post office or a digital form aggregator. This system gives workers an online screen to type data into, but a human still has to read the patient’s chart, copy the information, and paste it into the insurance form manually.
An AI-driven platform replaces this manual copying by using clinical NLP (Natural Language Processing), which is software that reads and understands human handwriting and typed medical text. This creates a highly automated data pipeline:
Comparison: Traditional Portals vs. Intelligent AI Platforms
| Capability | Traditional PA Software | AI Prior Authorization Platform |
| Data Ingestion | Manual data entry requires human staff to copy and paste data from the EHR into portal fields. | Automated extraction; uses clinical NLP to read and extract facts from unstructured charts and PDFs. |
| Criteria Matching | Manual lookup; staff must open separate payer portals to read through medical necessity PDFs. | Automated cross-referencing; a programmatic engine matches clinical text against live payer rules. |
| Error Handling | Reactive; rejections happen after submission when the payer notices missing information. | Proactive; pre-submission validation engines flag missing clinical details before the packet leaves. |
| Turnaround Time | Days to weeks; limited by manual processing speed and back-and-forth paper trails. | Real-time to hours; instant processing of clean claims through digital submission networks. |
This architectural leap from manual portal clicking to an automated intelligence layer is precisely why health systems are transitioning away from basic form-aggregating software.
C. Where ePA Fits Into the Prior Authorization Lifecycle
Electronic prior authorization (ePA) is the basic digital highway used to send data back and forth between the hospital and the insurance company. This software handles secure data transmission, but it does not evaluate whether the clinical documentation requirements actually justify the medical procedure.
The AI platform serves as the intelligent brain that sits on top of this ePA transport highway. At the same time, it manages the complex data preparation and tracking across the entire lifecycle:
- Upstream intelligence: The AI gathers the correct patient records, extracts the right medical codes, and builds a complete evidence packet before hitting the send button.
- Data transport: The system packages the evidence into standard formats, like old-school X12 278 EDI messages or modern FHIR R4 APIs, and sends it across the ePA network.
- Downstream tracking: The software runs background checks for authorization expiry tracking, alert engines, and status updates, so no approved window closes before the patient gets care.
D. What Platform Automates vs What Humans Review
A smart platform divides tasks between machine automation and human clinical expertise to keep operations running quickly. This software handles the repetitive, clear-cut administrative work that follows exact logic rules.
Whenever the software hits a gray area or a complex medical decision, it creates an exception route. Therefore, the platform automatically passes those nuanced cases to a human utilization review nurse or doctor:
Task Allocation: Machine Automation vs. Human Clinical Expertise
| Operational Task | Automated by AI Platform | Routed for Human Review |
| Eligibility & Plan Rules | Instantly checks active insurance coverage and flags if a specific CPT code requires authorization. | Handles edge-case coverage disputes or out-of-network exceptions requiring direct negotiation. |
| Evidence Extraction | Scans charts to pull out structured codes, lab values, and standard medication histories. | Synthesizes highly complex, multi-year medical charts for rare or orphan disease treatments. |
| Criteria Validation | Confirms if standard clinical metrics (e.g., blood pressure, BMI) meet the base payer rules. | Evaluates subjective physician notes when a patient doesn’t perfectly fit standard medical criteria. |
| Denial Management | Resolves administrative rejections caused by simple clerical omissions or mismatched codes. | Directs peer-to-peer clinical appeals and writes custom arguments for medical necessity denials. |
By automating these predictable administrative layers, the platform frees your high-value clinical staff to focus exclusively on cases where human judgment is truly irreplaceable.
E. How the Platform Connects Workflows
The platform breaks down the walls that usually separate medical charting, appointment scheduling, and final billing. At the same time, it ensures that every department works from the exact same real-time insurance tracking data.
Additionally, when a doctor enters a new treatment order into the medical record, the software instantly runs a background check to confirm if an approval is required.
According to a nationwide survey by the American Medical Association, 94% of physicians state that these manual administrative steps cause severe delays in patient care (Source: AMA, 2024).
By handling these checks instantly in the background, the platform secures approvals days before the patient arrives. This seamless workflow connection provides a clear bridge into why building this modern infrastructure matters now.
Why Your Organization Needs PA Platforms Right Now
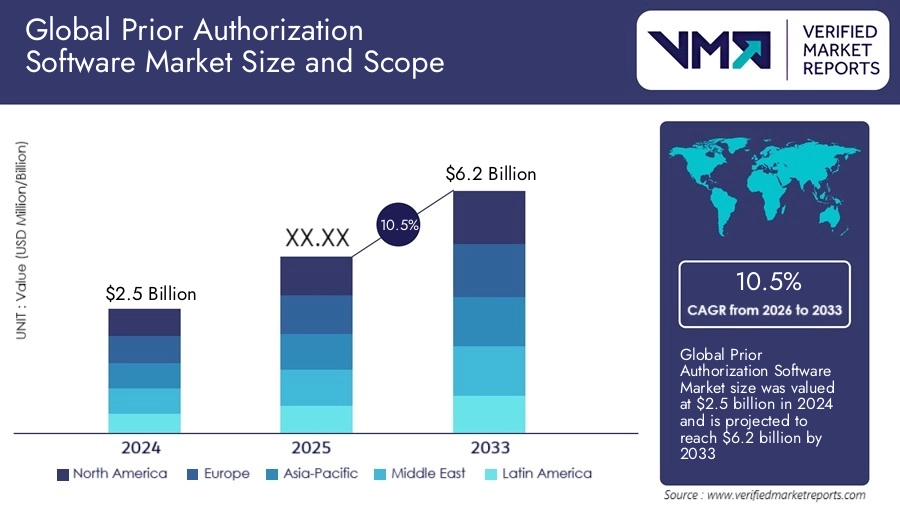
This rapid growth highlights an urgent shifting point for healthcare providers, revenue cycle companies, and digital health startups.
Therefore, relying on slow, hand-operated approval workflows has become an immediate threat to your operational cash flow, legal compliance, and daily staff retention.
1. Why Urgency Matters
The total volume of required insurance approvals rises every year, making manual data collection impossible to sustain.
When clinic teams handle these complex files by hand, it takes days to compile the evidence, which stalls hospital operations and hurts care delivery.
Deploying automation cuts down this processing delay, protecting the clinic’s timeline and ensuring patients get treated faster.
- Rising administrative burden: Medical insurance rules are growing highly complex, forcing billing clerks to spend hours hunting down specific clinical charts.
- Delayed scheduling and access: Long validation delays freeze patient scheduling, forcing people to wait weeks for critical surgeries or therapies.
- Staff workload and burnout: Front-line intake coordinators are completely overwhelmed by the constant paperwork, causing high employee turnover across the industry.
2. Business Impacts (Revenue, Denials, and Compliance)
Failing to secure a clean prior authorization before delivering medical care leads directly to unpaid claims and permanent revenue loss.
HFMA reported that initial claim denials climbed to nearly 12% in 2024, based on Kodiak Solutions data.
Building an intelligent tracking platform catches these documentation gaps early, stopping revenue leakage before treatments are ever scheduled.
- Denial prevention and revenue protection: Missing details in an authorization packet lead to instant medical rejections that stall hospital cash collections.
- Authorization turnaround time matters: Federal guidelines now require faster decision turnarounds, making slow manual preparation a major operational liability.
- Compliance and public reporting: The Centers for Medicare & Medicaid Services (CMS) requires insurance plans to publicly report their approval and denial metrics on their websites.
3. Market & Regulatory Context
The federal government has established strict compliance mandates under the landmark CMS-0057-F Interoperability and Prior Authorization final rule. This regulation forces insurance payers to speed up their operational response windows while adopting open data sharing networks.
Healthcare organizations must modernize their IT architectures immediately to connect with these new government-mandated infrastructure tracks.
- CMS-0057-F mandate: This law forces insurance companies to deliver final authorization decisions within 72 hours for urgent cases and 7 calendar days for standard requests (Source: CMS, 2024).
- Demand for electronic prior authorization: Payers must open production-ready Fast Healthcare Interoperability Resources (FHIR) APIs to receive structured electronic submissions (Source: CMS, 2024).
- Payer and provider digitization pressure: Medical networks are rapidly replacing rigid legacy software with modern, modular systems to handle real-time medical data transfers.
4. The Real Technical Challenge: Managing Rule Decay
Most basic software tools fail because they focus only on sending the final document quickly, completely ignoring the problem of rule decay.
Rule decay happens when an insurance company changes its underlying coverage rules, which instantly breaks old, rigid automation systems.
When these hidden rule changes occur without warning, even a lightning-fast submission portal will generate automatic rejections and expensive administrative rework.
For example, a hospital might deploy a basic automation tool that cuts its initial form submission time by 50%. However, if that system cannot read incoming payer updates, it will keep sending outdated clinical evidence packets that cause instant insurance denials.
A truly sustainable architecture requires an active rules ingestion layer that updates itself dynamically to keep your automation paths accurate.
This critical need for stable, self-updating data pipelines highlights exactly why custom development is the safest strategic path forward.
The Payer-Rule Drift Problem PA Automation Tools Miss
The biggest hidden failure point in prior authorization automation is payer-rule drift. This happens when an insurance company changes its internal medical policies, drug guides, or processing steps faster than your software updates them.
Basic systems that are built to hit submission endpoints quickly fail to actually track these constant downstream rule changes. When your automation runs on outdated information, it leads directly to instant medical rejections and expensive manual rework.
1. Payer Policy Changes
Insurance companies rewrite their clinical documentation guidelines frequently. This means an automated packet that passed checks last month will fail today because the base rules changed without notice.
- Sudden updates: Payers edit their medical logic without warning, meaning old data rules fail instantly.
- Manual tracking limits: Front-line teams cannot read through hundreds of pages of daily policy text to find these changes.
- Automation breakdown: A system that relies on fixed templates cannot adapt when an insurance plan updates its baseline care rules.
2. Formulary Checks
Health plans shuffle preferred medications between coverage tiers quarterly. This structural shifting instantly breaks static electronic prescription pathways and leads to immediate medication denials at the pharmacy counter.
- Tier movements: A drug that was fully covered last week may suddenly require a special authorization stamp this week.
- Data lag: Standard software tools often wait months to update their drug catalogs, leading to massive friction.
- Point-of-sale failures: Patients face surprise costs at the pharmacy counter because the system missed a tier shift.
3. New Documentation Rules
Payers regularly add new required fields to their intake portals. These include specific blood test histories or mandatory diagnostic codes that your system must extract before submission.
- Missing evidence: Forms get rejected instantly if they lack the newest lab tests or doctor notes.
- Field variation: Every major insurance network demands different data sets for the exact same medical procedure.
- Clerical errors: Manual teams easily miss these new fields, causing immediate rejections that ruin administrative metrics.
4. Step Therapy Updates
If a payer introduces a new rule requiring a patient to fail a cheaper medication first, a static platform will submit a high-tier drug request without attaching that critical failure history.
- Trial tracking: The software must prove the patient tried and failed the insurance company’s preferred baseline drug first.
- Workflow blocks: Skipping this check leads to immediate rejections, requiring staff to rebuild the entire medical claim.
- Care delays: Patients wait weeks for their correct treatments while staff manually pull old pharmacy receipts.
5. Specific Requirements
High-cost fields like oncology or orthopedics undergo monthly policy updates. This makes them highly vulnerable to sudden rule modifications that break standard AI prior authorization denial prevention logic.
- High-friction care: Cancer therapies and joint surgeries have the strictest insurance review layers in healthcare.
- Complex data needs: These cases require heavy clinical history files, not just basic doctor forms.
- Fast rule decay: Specialized medical guidelines evolve rapidly, causing fixed software tools to break within weeks.
Why Drift Causes Denials
Deploying an automation tool without an active rule-checking engine simply means you are delivering bad data to the insurance company faster. If your software does not continuously parse incoming policy modifications, your automated requests will fail to align with the active payer medical necessity criteria.
Recent industry data shows that these automated rule gaps cause average insurance denial rates to spike by 12% across major health networks (Source: HFMA, 2025). This continuous policy drift shows exactly why your platform needs a highly intelligent, real-time feature architecture.
Core Features Every AI Prior Authorization Platform Must Include
A production-ready platform needs requirement detection, payer-rule logic, evidence extraction, electronic submission, status tracking, denial prevention, security, and analytics. Building these layers ensures that your system can handle the messy reality of healthcare data without dropping critical transactions.
Without these core modules, your software will act as a basic data template rather than a true automated intelligence network.
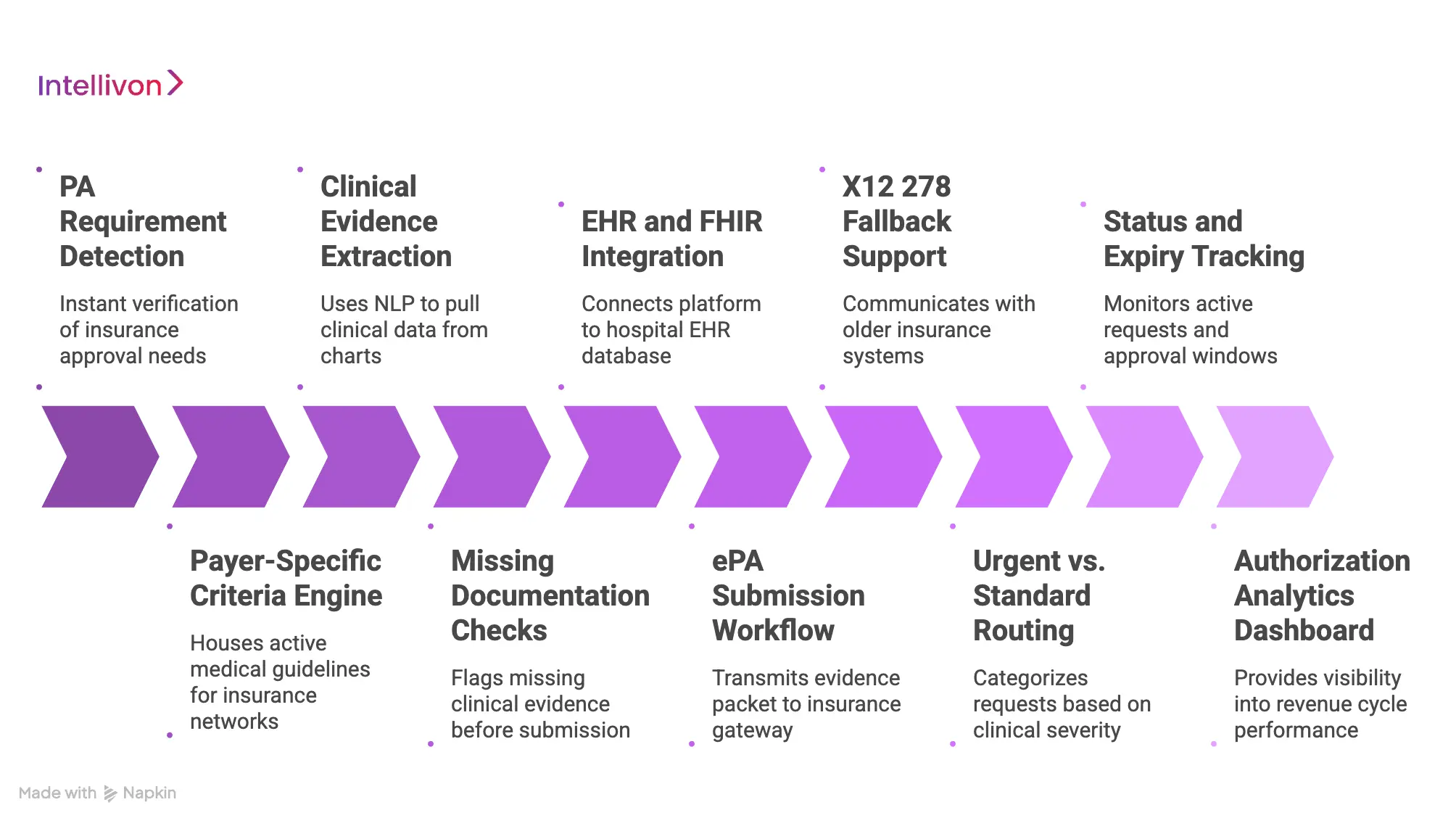
1. PA Requirement Detection
This module checks every scheduled appointment and medical order in real time to see if an insurance approval is actually required. It stops staff from wasting time on procedures that do not need a prior authorization stamp.
- Instant verification: The system scans the scheduled CPT codes against the patient’s specific insurance plan rules immediately.
- Workflow integration: Checks run quietly in the background without forcing the doctor to click extra screen buttons.
- Time savings: Eliminates up to 40% of manual phone checks by filtering out green-lit procedures instantly.
2. Payer-Specific Criteria Engine
This engine houses the active medical guidelines for every insurance network your hospital handles. It acts as the core brain of your prior authorization workflow automation build, matching patient files against precise insurance policies.
- Rule isolation: Separates rules by payer, plan type, and region to ensure extreme data matching precision.
- Drift management: Ingests daily policy text updates to keep its background logic completely accurate.
- Automated matching: Evaluates if a patient’s lab history satisfies the exact text rules of the insurance company.
3. Clinical Evidence Extraction
This module uses clinical natural language processing to read unstructured charts, physician notes, and laboratory PDFs. It pulls out the exact clinical data needed to justify the medical procedure.
- Contextual reading: Identifies relevant history items, like a patient failing a preferred drug tier six months ago.
- Code parsing: Automatically converts typed text sentences into clean, structured ICD-10 and CPT data formats.
- Zero data copying: Cuts out manual copy-paste work by pulling evidence straight from the medical chart.
4. Missing Documentation Checks
This pre-submission gate acts as a programmatic audit layer that flags missing clinical evidence before the request leaves your network. It serves as your primary defense line for AI prior authorization denial prevention.
- Proactive warnings: Alerts the billing team if a required X-ray report or blood panel is missing from the packet.
- Error blocking: Stops incomplete applications from being sent out, eliminating instant clerical rejections.
- Smart prompting: Gives users clear text instructions on exactly what medical file needs to be uploaded.
5. EHR and FHIR Integration
This infrastructure layer connects your platform directly to the hospital’s electronic health record (EHR) database. It relies on standard data hooks to pull and push patient information without disrupting clinical workflows.
- Bi-directional sync: Keeps medical records and authorization statuses perfectly updated across all systems simultaneously.
- Standard protocols: Uses HL7 and FHIR R4 data streams to ensure compatibility with modern healthcare networks.
- Data protection: Securely accesses information pipelines without exposing private patient text to outside networks.
6. ePA Submission Workflow
This engine handles the formal transmission of the complete evidence packet to the insurance company’s intake gateway. It represents the transactional core of your custom ePA software development project.
- Direct connections: Sends clean data packets straight into insurance intake APIs without manual portal hopping.
- Format assembly: Packages text notes, lab values, and application forms into a single, encrypted payload.
- Instant receipt tracking: Logs the insurance plan’s official digital tracking number the second a submission finishes.
7. X12 278 Fallback Support
This legacy transaction tool ensures your platform can communicate with older insurance systems that lack modern API technology. It translates your clean data into standard electronic data interchange (EDI) message streams.
- Universal connectivity: Guarantees your platform can send requests to small regional payers who still use old mainframe technology.
- EDI translation: Automatically maps modern FHIR database structures into rigid X12 278 data files.
- Error parsing: Reads old-school electronic rejection codes and turns them into plain, readable human text alerts.
8. Urgent vs. Standard Routing
This triage module automatically categorizes incoming approval requests based on clinical severity. It ensures that life-critical treatments bypass standard queues to prevent dangerous delays in patient care.
- Severity scanning: Scans physician notes for urgent markers to prioritize critical cases instantly.
- Timeline tracking: Adjusts system timers to match federal response windows, like the 72-hour limit for urgent care (Source: CMS, 2024).
- Alert systems: Flashes bright visual flags on staff dashboards if an urgent request is nearing its filing deadline.
9. Status and Expiry Tracking
This background monitoring tool continuously checks the active state of all submitted requests and approved authorization windows. It alerts teams well before an approval window closes to prevent costly workflow drops.
- Live status polling: Pings insurance data clearinghouses automatically to capture real-time approval updates.
- Expiration alerts: Warns scheduling teams if an approved surgery window will expire before the patient’s appointment.
- Utilization tracking: Tracks how many approved therapy visits a patient has used up versus how many remain valid.
10. Authorization Analytics Dashboard
This management screen gives healthcare executives complete visibility into their entire revenue cycle performance. It highlights hidden operational bottlenecks and measures the financial impact of your automation.
- Denial tracking: Pinpoints which specific insurance networks reject the most claims and flags the root causes.
- Speed metrics: Measures exactly how long each insurance plan takes to return a final approval stamp.
- Staff metrics: Tracks volume and accuracy across your utilization review teams to optimize daily labor allocations.
AI Prior Authorization Platform Architecture and Technical Design
An enterprise AI prior authorization platform architecture relies on a decoupled, multi-layered data pipeline that translates unstructured clinical workflows into structured, compliant transactional payloads.
This system isolates data ingestion, clinical NLP processing, and regulatory rule matching into distinct services to guarantee sub-second system response times and high data availability.
At the same time, by utilizing modern HL7 FHIR frameworks alongside legacy EDI conversion layers, this technical blueprint allows healthcare organizations to maintain real-time EHR integration while fulfilling complex CMS prior authorization compliance software mandates.
Architectural Layer Blueprint & Technology Stack
| Architecture Layer | Core Functional Purpose | Primary Technology Stack & Tools |
| User Layer | Renders responsive administrative dashboards and clinical tracking screens for authorization staff. | React.js, Tailwind CSS, TypeScript, WebSockets (for real-time status updates) |
| Workflow Orchestration Layer | Manages asynchronous task state, background queues, and event-driven clinical processing schedules. | Apache Airflow, Temporal.io, Node.js, RabbitMQ / Apache Kafka |
| EHR and FHIR Data Integration Layer | Handles bi-directional communication, data ingestion, and semantic mapping between medical records and the platform. | FHIR prior authorization API integration, HL7 v2 Engines (Mirth Connect), HAPI FHIR Server |
| Payer API & Integration Layer | Dispatches compliant transactional payloads to external health plan endpoints and clearinghouses. | FHIR R4 Prior Authorization API (Da Vinci PAS), AWS Lambda, X12 278 transaction parsers |
| Medical Necessity Rules Layer | Evaluates clinical documentation data against active insurance policies and localized utilization management rules. | Drools Rules Engine, Python Rule Interpreters, PostgreSQL (for static rule libraries) |
| AI Evidence & Denial Prediction Layer | Extracts text from charts via clinical NLP and computes numerical probability scores for insurance denial risks. | PyTorch, Hugging Face Transformers, Amazon Comprehend Medical, OCR Engines (Tesseract) |
| Status Management Layer | Polls, clearinghouses, and tracks approved windows to handle background authorization expiry tracking. | Redis (for rapid status caching), Celery Workers, PostgreSQL Time-Series Databases |
| Security & PHI Protection Layer | Enforces strict data access controls, tokenization, and end-to-end encryption for patient information safety. | OAuth 2.0 / OIDC, AWS KMS (Key Management Service), HashiCorp Vault, TLS 1.3 |
| Analytics ROI Measurement Layer | Collects operational data logs to build performance summaries and trace long-term financial metrics. | ClickHouse (for high-speed analytical queries), Apache Superset, Python Pandas |
| Admin Configuration Layer | Allows systems managers to adjust intake settings, update tenant parameters, and tune machine models. | Angular, Python Django REST Framework, PostgreSQL |
| Multi-Tenant SaaS Architecture | Separates database storage and system configurations securely across distinct hospital networks. | PostgreSQL Row-Level Security (RLS), Docker, Kubernetes (K8s) Namespace Isolation |
This decoupled architectural design ensures that heavy clinical NLP background processing never disrupts the front-end user experience or stalls primary EHR transaction speeds.
By building on this structured framework, engineering teams can scale individual microservices independently as transaction volumes grow across your health system network.
How AI Agents Enhance Prior Authorization Platforms
A mature AI prior authorization platform should not rely on a single, general-purpose AI model. This platform must use task-specific agents that coordinate across EHR records, payer guidelines, evidence checks, submissions, follow-ups, and human reviews. At the same time, major technology infrastructure firms have framed prior authorization as a highly effective multi-agent healthcare use case.
This modular design reduces processing time from days to minutes while maintaining extreme compliance and workflow accuracy:
Agent 1: PA Requirement Detection at Order Entry
This specialized agent acts as the initial validation gate, checking whether a treatment order requires prior authorization before a procedure is scheduled or a medication is prescribed. These agents intercept healthcare data live within the clinician’s workspace to eliminate late-stage administrative obstacles.
- Data scanning: Parses the patient’s plan, service code, diagnosis, payer network, clinic location, and provider credentials simultaneously.
- Instant filtering: Cross-references this tracking data against known insurance rules to clear exempt orders instantly.
- Surprise prevention: Catches approval requirements at the point of care, long before the patient leaves the clinic or a claim fails.
Agent 2: Evidence Extraction From Clinical Records
This agent operates as a focused clinical data miner, scanning patient records to extract documentation that proves medical necessity. It isolates factual historical evidence from raw text without modifying or inventing information.
- Multi-source scanning: Scans unstructured physician notes, laboratory spreadsheets, pathology imaging reports, medication histories, and historic referral documents.
- Targeted extraction: Pulls exact clinical data points that correspond directly to the targeted payer’s medical coverage rules.
- Immutable source citations: Attaches strict, unalterable database tags and line citations to every extracted detail to keep data fully auditable.
Agent 3: Payer Criteria Matching and Gap Checks
This agent acts as an automated audit layer, evaluating the extracted clinical evidence directly against the targeted insurance plan’s active rule library. It connects directly to a versioned payer criteria engine to handle updating rules safely.
- Logic validation: Compares the structured evidence packet against specific criteria rules, ensuring the medical justification holds up.
- Gap identification: Flags missing laboratory panels, failed alternative therapies, or incomplete diagnostic details before data submission.
- Denial mitigation: Prevents clean-claim failures by blocking incomplete authorization packets from leaving the secure local network.
Agent 4: Submission, Follow-Up, and Status Tracking
This agent operates as an active orchestration layer rather than a basic notification tool, handling the transactional delivery and long-term monitoring of the file. It manages the communication channel with the payer across multiple tech generations.
- Omnichannel routing: Dispatches completed claims through the FHIR R4 Prior Authorization API, older legacy X12 278 transactions, secure portals, or automated fax loops.
- Asynchronous tracking: Monitors active approval statuses, parses specific insurance denial reasons, tracks expiration dates, and updates internal tasks.
- Queue minimization: Eliminates manual phone queues and portal-checking chores by automating background status polling.
Agent 5: Denial Prevention and Appeal Support
This final agent functions as a risk management tool, scoring every outbound file for rejection risks and assembling structured appeals when a denial occurs. It ensures the administrative workflow remains operational even when facing an insurance rejection.
- Risk analysis: Scores prepared applications before transmission, flagging packets that have a high statistical probability of insurance rejection.
- Packet compilation: Automatically builds structured appeal packets, objective denial summaries, and concise brief files for peer-to-peer physician reviews.
- Human-led control: Keeps final clinical decisions human-led by presenting clear data choices to utilization management nurses rather than acting autonomously.
Agent Coordination Blueprint: Multi-Agent Task Delegation
| AI Agent Specialist | Primary Input Data | Primary Operational Output |
| 1. Requirement Detector | Scheduled CPT codes & Patient Plan ID. | Boolean PA determination flag. |
| 2. Evidence Extractor | Unstructured EHR charts & Provider notes. | Labeled, cited clinical text snippets. |
| 3. Criteria Matcher | Extracted text snippets & Live Payee PDFs. | Gap analysis report and readiness score. |
| 4. Submission Orchestrator | Validated clinical evidence payload. | Transaction ID & Live status updates. |
| 5. Denial Architect | Inbound rejection codes & Appeal guidelines. | Structured appeal brief for human review. |
This distributed multi-agent approach keeps all artificial intelligence recommendations fully explainable, auditable, and reviewer-approved.
Utilizing a system of specialized agents ensures that each model performs a narrow, highly verified task, which keeps the broader data pipeline stable and secure
[For a deeper breakdown of multi-agent software coordination, see our guide on Enterprise AI Agent Orchestration Platform Development.]
How to Build an AI Prior Authorization Platform: 8-Stage Development Process
Building an enterprise AI prior authorization platform requires a structured engineering roadmap that balances front-end clinical workflows with complex back-end healthcare data integrations.
Moving systematically from clinical workflow mapping through production scaling prevents structural data bottlenecks and keeps the platform fully secure and compliant with modern medical data regulations.
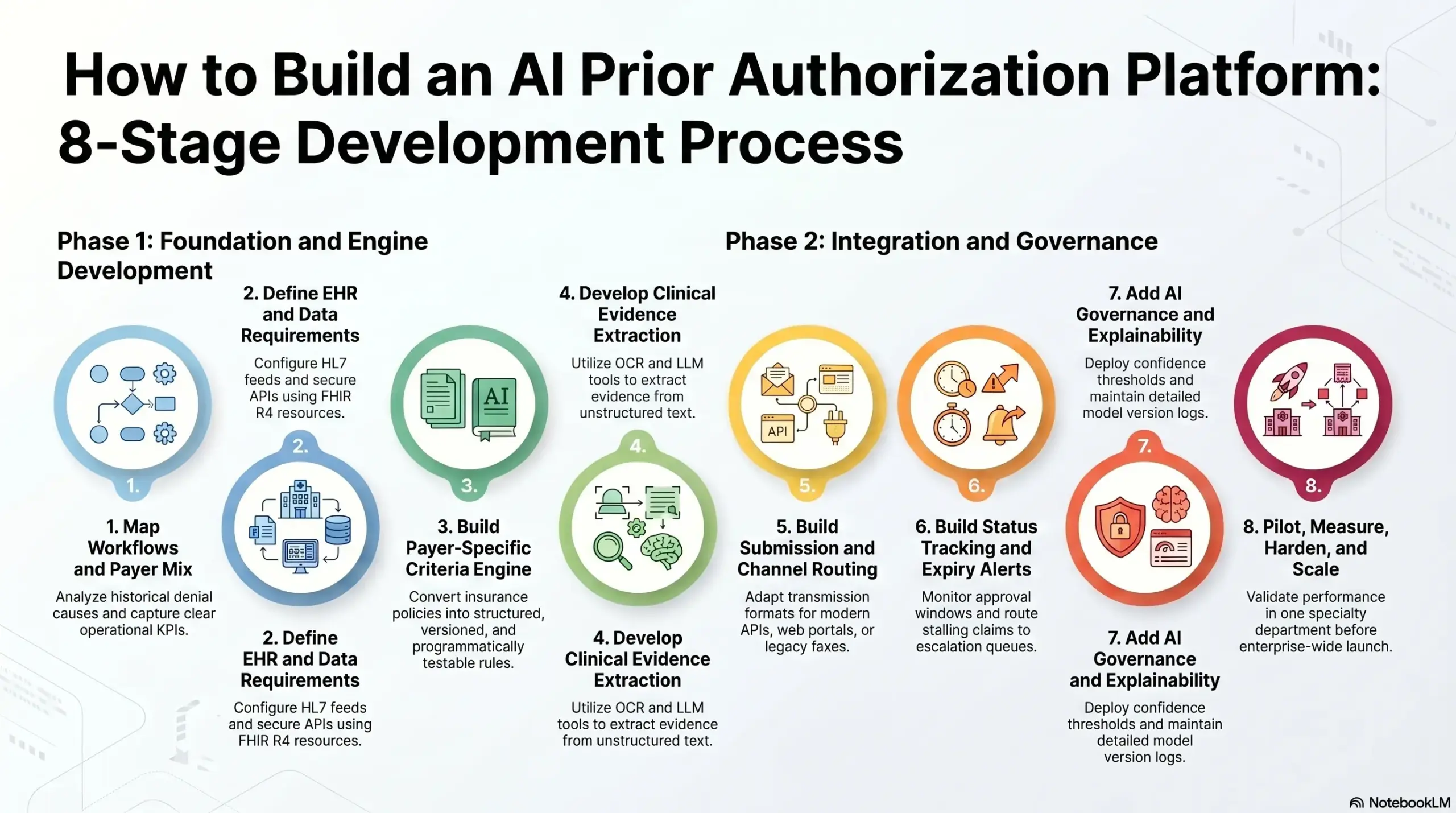
Stage 1: Map Prior Authorization Workflows and Payer Mix
The development process begins by mapping your existing prior authorization volume, regional payer mix, core service lines, historical denial causes, daily staff tasks, and insurance approval timelines.
- Technical execution: Establish continuous workflow discovery audits across your scheduling departments, separate your distinct service-line pipelines, and execute comprehensive data analysis on past insurance denials. Developers must catalog every manual task your staff performs alongside your historical authorization turnaround times to capture clear operational KPIs.
- Risk of failure: Skipping this initial step causes your engineering team to automate low-value, low-friction administrative workflows while your highest-cost, most complex prior authorization bottlenecks remain completely manual.
- The Intellivon approach: We start every project by identifying and defining your highest-value, most expensive authorization lane before any code architecture or model selection begins.
Stage 2: Define EHR, FHIR, and Data Access Requirements
Your platform must know exactly which clinical records, insurance coverage fields, medical orders, and care documentation details it needs to capture before any artificial intelligence models are designed.
Building clear data access requirements guarantees that the software can securely query medical databases without stalling standard electronic medical record networks.
- Technical execution: Map out your required data connections across your primary EHR integration network by configuring modern HL7 data feeds and secure EHR APIs. Engineers must structure the ingestion pipeline around core FHIR R4 resources, including Patient, Coverage, Condition, MedicationRequest, ServiceRequest, Observation, and DiagnosticReport, while setting strict programmatic data quality filters.
- Risk of failure: The platform will extract incomplete or fragmented clinical evidence, which creates false confidence metrics and produces weak prior authorization packets that trigger immediate insurance plan rejections.
- The Intellivon approach: We map your specific clinical evidence requirements directly against available EHR database schemas before choosing or training any underlying machine learning models.
Stage 3: Build the Payer-Specific Criteria Engine
The criteria engine serves as the logical core of your software, converting complex, text-heavy insurance policies into structured, versioned, and programmatically testable authorization rules. This module translates changing human insurance guidelines into clean code parameters that your automation scripts can execute instantly.
- Technical execution: Construct a rule interpreter that handles complex medical necessity logic, automated formulary checks, active step therapy conditions, and combined diagnosis-procedure validations. The system must run on a strict Git-style version control framework that logs clear, effective dates for every insurance rule modification to manage ongoing policy drift.
- Risk of failure: Your platform will simply submit bad data packets faster, sending incomplete or non-compliant requests that fail to match active insurance criteria.
- The Intellivon approach: We treat payer logic as a continuously maintained, live product component rather than leaving it buried as hardcoded backend software code.
Stage 4: Develop Clinical Evidence Extraction and Documentation Checks
The platform must run automated workflows to find required medical evidence across structured EHR database tables, free-text doctor notes, laboratory spreadsheets, and uploaded imaging PDFs.
This layer acts as your system’s primary clinical intelligence tool, turning unstructured medical text into clear administrative proof.
- Technical execution: Build multi-stage data processing pipelines utilizing advanced Optical Character Recognition (OCR), clinical natural language processing, and open-source Large Language Model (LLM) text extraction tools. Program the software to generate direct line citations, compute statistical confidence scores, and trigger real-time missing-document alerts on the user dashboard.
- Risk of failure: The platform fails to prove medical necessity clearly enough to pass automated insurance screening, which spikes your denial rates and forces staff back into manual entry queues.
- The Intellivon approach: We separate extracted clinical evidence from generated summaries to ensure your utilization review nurses can validate raw source text safely before submission.
Stage 5: Build ePA Submission and Channel Routing
The system must automatically route each prepared prior authorization request through the most efficient electronic communication channel available while maintaining reliable analog fallbacks.
Because different insurance carriers utilize completely different technology standards, your platform must adapt its transmission format on the fly.
- Technical execution: Engineer a channel-aware submission engine that natively dispatches requests using the modern FHIR prior authorization API integration pathway or standard EDI X12 278 transaction clearinghouse nodes. Developers must build secure automated web portal scraping scripts alongside legacy digital fax loops to manage low-tech payers, while maintaining complete electronic transmission logs.
- Risk of failure: Staff is forced to manually type information into insurance portals after your AI has already prepared the data packet, which destroys your technology ROI.
- The Intellivon approach: We design smart, channel-aware routing logic directly into the submission core because every insurance plan operates at a different stage of digital readiness.
Stage 6: Build Status Tracking, Expiry Alerts, and Escalation Workflows
Prior authorization management requires continuous tracking across the entire lifecycle of a medical claim, long after the initial data packet is successfully sent out.
The tracking module keeps your revenue cycle running smoothly by eliminating hidden timeline gaps and monitoring active approval windows in the background.
- Technical execution: Configure automated polling services that check insurance gateways for real-time status updates, log approved insurance numbers, and parse official denial reason strings. Program background timers to monitor authorization expiry dates, issue automated renewal alerts, and route stalling claims directly into priority clinical escalation queues.
- Risk of failure: Approved authorization windows expire silently, staff lose total operational visibility, and high-cost clinical claims get hit with retroactive insurance denials.
- The Intellivon approach: We connect your live authorization tracking states directly into your downstream revenue cycle management (RCM) billing tools to prevent financial leakage.
Stage 7: Add AI Governance and Explainability Controls
Your platform must be built to support clinical teams with evidence-backed recommendations rather than attempting to act as an unmonitored decision-maker.
Enforcing strict AI governance protocols keeps your automation patterns fully transparent, auditable, and aligned with federal clinical software safety guidelines.
- Technical execution: Deploy hardcoded confidence score thresholds that automatically route low-confidence AI Extractions into human review queues for mandatory manual approval. Build unalterable backend model version logs, maintain detailed prompt history databases, capture every manual human override action, and format clear explainability readouts for auditing teams.
- Risk of failure: The system becomes impossible to defend during official government audits, internal payer disputes, or sensitive medical compliance reviews.
- The Intellivon approach: We build all artificial intelligence outputs as evidence-backed recommendations that explicitly present their source references to your clinical reviewers.
Stage 8: Pilot, Measure, Harden, and Scale
The final deployment phase requires launching the platform inside a single, controlled clinical environment to validate system performance before scaling the technology across your entire enterprise network.
This gradual rollout allows engineers to fine-tune integrations under real-world operating conditions without interrupting daily patient care.
- Technical execution: Launch your pilot workflow within one high-volume specialty department, execute intensive User Acceptance Testing (UAT), run penetration security scans, and perform heavy infrastructure load testing. Monitor automated KPI tracking systems daily, gather structured feedback from your front-line medical staff, and follow a modular scaling roadmap to onboard subsequent clinics.
- Risk of failure: A fragile software build that works perfectly inside a simulated testing environment crashes completely when exposed to messy real-world EHR environments and daily staff workloads.
- The Intellivon approach: We treat the initial pilot as an active, production-grade learning phase where data logs drive the final performance hardening of your system.
Following this system generates a scalable enterprise-grade AI prior authorization platform.
Top Healthcare Companies Using AI Prior Authorization
Specialized healthcare technology companies are actively deploying AI prior authorization platform models inside production networks to remove administrative friction across the entire care spectrum.
Therefore, examining how these live operational networks scale proves that the market is moving permanently toward API-first, agent-driven prior authorization architectures to protect healthcare operational cash flows.
1. Cohere Health: AI-Driven Utilization Management
Cohere Health implements advanced clinical intelligence to manage broad utilization networks, handling multi-step care tracks rather than isolated data submissions.
Their system processes complex clinical evidence across both payer and provider platforms to reduce decision turnaround times.
- Platform capabilities: The software uses clinically trained AI models to automate up to 90% of routine prior authorization requests while maintaining high provider satisfaction levels
- Interoperability footprint: Their system has safely processed millions of discrete transactions through standard FHIR prior authorization API integration frameworks.
- Operational outcome: Clinicians experience up to a 40% reduction in total administrative handling time, allowing healthcare workers to focus on active patient care.
2. Develop Health: Medication Access Prior Authorization
Develop Health targets specialized prescription workflows, automating benefits verification and evidence formatting for high-cost specialty medications.
This platform’s technology integrates directly into active pharmacy pipelines to prevent long distribution delays at the counter.
- Platform capabilities: The platform uses large language models and clinical NLP to read unstructured physician notes and automatically fill out complex payer forms.
- Submission coverage: The system features channel-aware routing that dispatches completed packets via custom ePA software development pipelines, direct portal scripts, or automated fax loops.
- Operational outcome: Case studies reveal that automating clinical evidence extraction drives an 83% reduction in manual authorization handling time per request.
3. Rhyme: Touchless Prior Authorization Network
Rhyme constructs dedicated electronic collaboration pathways that securely link large insurance payers directly with local health system databases.
This platform bypasses traditional portal structures entirely, focusing on completely touchless automated decision loops.
- Platform capabilities: The system connects providers and payers inside a shared transaction dashboard to confirm coverage requirements and verify active clinical parameters.
- Network footprint: The network securely orchestrates more than 4 million prior authorizations annually across dozens of major enterprise provider systems.
- Operational outcome: Eliminates repetitive phone queues and administrative portal logging by automating real-time bi-directional status updates.
4. basys.ai: Explainable AI for Utilization Management
basys.ai applies highly auditable generative AI algorithms to manage utilization review, medical necessity scoring, and long-term payment integrity.
Their software infrastructure prioritizes algorithmic transparency to ensure all machine decisions can be fully traced by medical auditors.
- Platform capabilities: The engine cross-references patient text against deep policy databases to calculate exact compliance scores before files are delivered to payers.
- Industry recognition: The company’s secure, adaptive AI compliance architecture was formally recognized in Gartner’s 2025 Hype Cycle for Intelligent Prior Authorization.
- Operational outcome: Protects clinical operations against sudden rule changes by pairing automated policy parsing with strict model governance tracks.
5. Infinitus: Voice AI for PA Follow-Up
Infinitus automates the post-submission lifecycle by deploying specialized conversational voice AI agents to handle phone-based insurance tracking.
This software layer targets the hidden administrative burden that occurs after a claim is already dispatched.
- Platform capabilities: The voice agents navigate complex insurance phone trees and interact naturally with payer representatives to capture live status updates.
- Data extraction: Programmatically logs crucial verbal data, including precise authorization numbers, active validity windows, and missing document requirements.
- Operational outcome: Eliminates manual phone queue holding times for clinic staff, drastically improving backend data collection speed and administrative accuracy.
Market Validation: Production-Grade AI Impact Metrics
| Technology Innovator | Primary Architectural Focus | Documented Operational Performance |
| Cohere Health | Multi-step clinical intelligence networks. | Automates up to 90% of routine prior authorization steps. |
| Develop Health | Specialty medication access pipelines. | Achieves an 83% drop in manual file handling times. |
| Rhyme | Collaborative touchless provider networks. | Coordinates over 4 million requests without portal hopping. |
These live production implementations demonstrate why health systems are rapidly abandoning static, template-based software systems.
For a deeper breakdown of constructing high-volume automated data pipelines that secure patient information across complex networks, see our guide on AI Healthcare Claims Processing Software Development.
Seeing these operational successes helps clarify how your engineering team can accurately calculate financial returns before writing platform code.
How Much Does an AI Prior Authorization Platform Cost?
A custom AI prior authorization platform usually costs $90,000–$350,000+, depending on workflow complexity, payer integration depth, FHIR readiness, AI model scope, HIPAA controls, and whether you are building an internal workflow tool or a commercial SaaS platform.
The lower end usually covers a focused MVP for one service line, limited payer rules, basic evidence extraction, and simple authorization tracking. The higher end applies when the platform needs FHIR R4 integration, SMART on FHIR workflows, X12 278 transaction support, payer-specific criteria engines, denial prediction, multi-role dashboards, audit trails, and enterprise deployment.
| Development Phase | Estimated Cost | What It Covers |
| Discovery and workflow mapping | $8,000–$20,000 | PA workflow review, payer mix, denial analysis, MVP scope |
| UX/UI and workflow design | $10,000–$30,000 | Review queues, dashboards, admin tools, escalation flows |
| Backend and workflow engine | $25,000–$75,000 | Case management, task routing, state machines, analytics |
| EHR, FHIR, and payer integrations | $25,000–$100,000 | FHIR R4, SMART on FHIR, HL7, X12 278, payer APIs |
| Payer criteria engine | $15,000–$60,000 | Medical necessity rules, step therapy, and formulary checks |
| AI model development | $30,000–$120,000 | OCR, NLP, LLMs, denial prediction, evidence retrieval |
| HIPAA, security, and audit controls | $15,000–$50,000 | RBAC, encryption, logs, BAA readiness, monitoring |
| Testing, deployment, and pilot | $12,000–$40,000 | QA, UAT, model validation, rollout, training |
Ongoing maintenance usually costs 18%–30% of the initial build cost per year. This covers payer-rule updates, model monitoring, security patches, API changes, compliance documentation, cloud infrastructure, and new workflow improvements.
The smartest cost plan starts with a narrow, high-value MVP. Then, the platform can expand across payers, service lines, AI modules, and compliance requirements after the first workflow proves measurable ROI.
Free Cost Estimate: Get Your AI Prior Authorization Platform Cost Estimate
Planning an AI prior authorization platform budget? Intellivon can help you estimate the cost based on your payer mix, workflow scope, AI modules, FHIR and EHR integrations, compliance depth, and launch timeline.
Build vs. Buy Framework for Prior Authorization Software
Buy when your clinical workflows are completely standard, and market speed matters most. Build when high payer complexity, specialized medical workflows, unique product roadmap goals, complete data ownership, or strict compliance controls make custom logic absolutely necessary.
Therefore, choosing the wrong path can tie up your engineering teams for quarters or leave you trapped with a generic vendor tool that cannot read your specialized patient charts.
When to Build, Buy, or Combine
| Strategic Option | Optimal Operational Context | Primary Engineering Advantage | Bottom-Line Financial Risk |
| Choose Buy | Standard primary care workflows, minimal system customization needs, and short compliance deployment timelines. | Zero initial coding; fast setup using pre-built vendor data connections. | High long-term licensing fees and severe vendor feature lock-in. |
| Choose Build | Highly specialized clinical fields, proprietary software roadmaps, and massive prior authorization volumes. | Complete IP ownership; custom matching logic tailored to your exact clinic rules. | High upfront engineering costs and ongoing maintenance overhead. |
| Choose Hybrid | Mixed provider networks requiring fast base connectivity paired with advanced custom AI extraction layers. | Rapid deployment of base forms paired with highly tailored clinical NLP engines. | Complex multi-vendor integration layers and split system debugging tasks. |
| Do Not Build | Low monthly authorization volumes, highly fragmented EHR database access, or limited technical support budgets. | Avoids sinking capital into complex, niche software development projects. | System crashes and data bottlenecks if small internal teams fail to manage updates. |
Vendor Limits vs. Custom Workflow Control
Ready-made prior authorization software often runs on fixed, rigid templates that force your clinical staff to change how they naturally document care. These packaged tools struggle to process unique clinical workflows, such as multi-step orthopedic surgery tracks or complex oncology drug cycles.
At the same time, building a custom AI prior authorization platform gives your product team 100% control over the user experience, allowing you to design data capture screens that mirror your doctors’ exact charting habits.
1. Integration, Ownership, and Data Control
When you buy a standard vendor tool, your private patient health information (PHI) must travel out to an external third-party server for processing. This data handoff introduces major compliance risks and leaves your network vulnerable to vendor system downtime.
- Complete data residency: Building a custom platform lets your enterprise keep all clinical data within your own secure cloud environment.
- Direct database hooks: Custom code allows you to create deep, bi-directional database connections that sync information instantly without relying on a vendor’s slow public API.
- Audit log control: Your IT team retains unalterable, native access logs for every transaction, making compliance reviews stress-free.
2. Long-Term Maintenance and SaaS Differentiation
While buying software has a lower upfront cost, the licensing fees scale up aggressively as your patient volume grows. Furthermore, relying on the same generic tool as your competitors prevents you from building a unique operational advantage.
For digital health startups and large revenue cycle companies, a custom build creates a valuable proprietary technology asset that sets your brand apart in the market.
If you are constructing an internal tool for a health system, your main focus is on reducing staff burnout and stopping localized revenue leakage. However, if you are a software founder building a commercial SaaS product, your architecture must prioritize multi-tenant data isolation and highly flexible API layers.
For a deeper breakdown of constructing scalable multi-tenant architectures that remain safe and compliant, see our guide on Enterprise AI Agent Orchestration Platform Development.
Therefore, understanding these product differences helps clarify the total capital needed to fund your project.
Build an AI Prior Authorization Platform With Intellivon
At Intellivon, we help hospitals, specialty practices, RCM companies, digital health startups, and healthcare SaaS teams build AI prior authorization platforms around real operational workflows.
Our approach focuses on the foundation first. Here, we define the right scope, design the platform architecture, plan FHIR and EHR integrations, build AI evidence extraction workflows, create payer-specific criteria engines, and add HIPAA-ready audit controls from the start.
This helps your team reduce manual PA work, improve documentation quality, prevent avoidable denials, and track ROI clearly.
A. Help You Define the Right Platform Scope
We map your payer mix, service lines, authorization volume, denial patterns, clinical workflows, and launch goals before development begins.
This helps your team decide whether to start with imaging, specialty medication, surgery, referrals, or another high-value PA workflow.
B. Design the Architecture and Integration Roadmap
Our experts plan the system around your EHR, FHIR resources, payer APIs, X12 278 workflows, clearinghouse routes, user roles, dashboards, and reporting needs.
This gives your platform a clean technical foundation before AI modules are added.
C. Build AI Evidence and Payer Criteria Workflows
We develop AI workflows that extract clinical evidence from notes, labs, reports, and documents, then match that evidence against payer-specific criteria.
This helps staff identify missing documentation before submission.
D. Add HIPAA, Audit, and ROI Controls
We design secure PHI handling, access controls, audit logs, reviewer approvals, model traceability, and performance dashboards. Owing to this, your team can track authorization turnaround time, denial risk, staff workload, and ROI as the platform scales.
Whether you are looking to deploy specialized clinical NLP engines to read unstructured charts or need to engineer a scalable, multi-tenant SaaS platform that connects directly with modern FHIR networks, our engineering team can help.
Let’s build a platform that scales. Schedule a technical consultation with an Intellivon architect today to map your data requirements, evaluate implementation costs, and draft a production-ready development blueprint for your team.
Conclusion
Deploying a custom AI prior authorization platform is a foundational healthcare infrastructure layer that unifies live EHR data, versioned payer criteria, FHIR APIs, and clinical NLP into a resilient revenue engine.
For health systems, digital health startups, and RCM firms managing complex specialty care or high transaction volumes, a custom build is the only viable path to achieve absolute data ownership and eliminate rule decay.
Therefore, as you evaluate your development roadmap, partner with an experienced practitioner team like Intellivon to architect a secure, compliance-ready automation layer that eliminates manual administrative friction.
Things To Know About AI Prior Authorization Platforms
Q1. How much does AI prior authorization software development cost?
A1. Building a production-ready AI prior authorization platform generally ranges from $180,000 to $450,000 for an initial enterprise deployment. At the same time, the total capital requirement scales based on your required EHR data integrations, the number of distinct insurance carriers connected to your payer-specific criteria engine, and the complexity of your clinical NLP models.
Q2. How long does it take to build a prior authorization automation system workflow?
A2. Developing a fully integrated build prior authorization automation system takes between 5 and 7 months from initial discovery to final pilot launch. Therefore, setting up baseline data access pipelines and rule engines takes 12 weeks, while refining multi-agent models and completing deep EHR system testing requires an additional 8 to 16 weeks.
Q3. Can an AI prior authorization platform be HIPAA-compliant?
A3. Yes, a custom platform can achieve full compliance by incorporating end-to-end data tokenization, localized cloud storage hosting, and role-based access rules. At the same time, designing an internal system lets your technical team retain absolute data residency and control unalterable audit trails, which eliminates the security vulnerabilities of third-party vendor platforms.
Q4. What AI models are needed for AI prior authorization denial prevention?
A4. Effective AI prior authorization denial prevention relies on a hybrid model layer that coordinates clinical NLP text extraction with deep-learning classification networks. Here, Named Entity Recognition models pull specific facts from free-text charts, while specialized transformers score data packets against target coverage rules to flag rejection risks before delivery.
Q5. What integrations matter most in electronic prior authorization platform development?
A5. Successful electronic prior authorization platform development depends on secure, bi-directional HL7 data streams and modern FHIR R4 API integrations to synchronize patient charts smoothly. At the same time, the platform must also link natively with clearinghouse networks using legacy X12 278 data standards to communicate with older, non-API insurance workflows.