

Key Takeaways:
-
Generative AI RCM uses LLMs, RAG pipelines, and clinical NLP to support coding, appeals, and authorization.
-
EHR, FHIR, HL7 CDA, EDI 837/835, and private model hosting are core enterprise architecture requirements.
-
Hallucination controls, PHI protection, model grounding, and human review determine real production value.
-
A focused MVP costs $140,000 to $280,000, while enterprise platforms reach $300,000 plus.
-
Intellivon builds GenAI RCM as a governed revenue infrastructure, not a chatbot layer added to billing.
Generative AI RCM software development means building revenue cycle systems that read unstructured clinical text and convert it into billable, compliant code sets. Rules-based automation handles structured data well, but 80% of all clinical data exists as unstructured text, and that is precisely where standard RCM systems stall and significant ROI disappears.
The gap in standard GenAI RCM builds is specialty-specific fine-tuning. A general-purpose language model applied to oncology or orthopedic billing produces code suggestions that might pass front-end checks, yet fail at the payer level. When fine-tuned on specialty clinical language and paired with confidence scoring, these models can prevent up to 85% of avoidable denials.
Intellivon has spent over 10 years building GenAI systems for healthcare workflows with specialty-aware fine-tuning pipelines. This blog covers model selection, training data requirements, EHR integration specs, compliance controls, and real development cost ranges, so you can make an informed decision before the development process begins.
What Is Generative AI Revenue Cycle Management Software?
Generative AI revenue cycle management software is a healthcare system that uses large language models and clinical AI to handle the language-heavy parts of the revenue cycle, including coding assistance, prior authorization drafting, denial appeals, payer correspondence, and remittance interpretation. It generates, summarizes, and validates revenue cycle work automatically, while keeping human review and audit control in place throughout.
1. GenAI RCM vs Traditional RCM Automation
Traditional revenue cycle management relies on rigid business rules engines and Robotic Process Automation (RPA) to process structured data fields.
While effective for repetitive scripts, these legacy platforms immediately break when forced to interpret unstructured medical charts or nuanced clinical contexts.
| Capability Layer | Traditional RCM Automation (RPA) | Generative AI RCM Platforms (LLM / RAG) |
| Data Ingestion | Restructured CSV, EDI 270/271, and fixed database fields. | Unstructured clinical notes, PDFs, scans, audio transcripts. |
| Logic Execution | Hard-coded if-then statements; breaks on schema changes. | Context-aware semantic understanding and dynamic reasoning. |
| Output Generation | Static form completion with zero narrative capability. | Complex medical narrative and appeal letter generation. |
By moving away from brittle scripts, healthcare networks can transition from reactive tracking to proactive revenue preservation. This architectural shift allows systems to ingest highly specialized vocabularies and scale administrative outputs dynamically without constant manual code updates.
2. Technology Stack Capabilities
The underlying technology stack introduces specific cognitive capabilities that traditional automation simply cannot replicate.
These core mechanisms allow the platform to read, analyze, and execute complex billing operations with human-like comprehension:
- Large language models in healthcare RCM parse intricate clinical narratives that defy standard rule matching.
- Retrieval-augmented generation links the LLM directly to active electronic health records (EHR) to ensure absolute factual grounding.
- Clinical text summarization compresses multi-page discharge summaries into dense, auditable data packets.
- Structured output generation forces the model to return valid JSON payloads instead of unpredictable free text.
- Explainable AI recommendations maintain a clear coding audit trail by linking every suggestion to its exact clinical source.
These foundational tools translate directly into automated, high-fidelity operational workflows across the department.
3. Healthcare-Specific Workflows
Deploying these systems inside enterprise environments requires targeting specific, high-overhead billing bottlenecks.
Engineers can embed AI into four critical transaction layers to replace legacy manual review sequences.
1. GenAI medical coding software
The engine uses clinical NER models to run unstructured clinical text processing on raw chart data.
The system then delivers automated ICD-10-CM code suggestion outputs and CPT code recommendation options directly into the biller’s workspace, maintaining a verifiable coding audit trail for compliance.
2. GenAI prior authorization software development
This pipeline uses a payer rules engine to extract authorization criteria from external portals via a FHIR document API.
It automates prior authorization letter drafting and compiles a medical necessity validation package, reducing manual submission delays from days to minutes.
3. GenAI denial management software
When a claim is rejected, the platform parses the explanation of benefits summarization layer to isolate the exact rejection reason.
It coordinates a targeted AI-assisted denial response drafting sequence and outputs a complete appeal letter generation package cross-referenced with internal clinical documentation.
4. LLM-powered healthcare billing automation
This foundational layer manages the end-to-end financial transaction cycle by automating remittance advice interpretation and payer correspondence automation.
The system boosts first-pass resolution rates and lowers the cost per claim by eliminating friction in data processing.
Transitioning to these intelligent pipelines allows health systems to dramatically reduce administrative drag and optimize their baseline financial operations.
Why GenAI RCM Has Become a Build Priority Now
Generative AI RCM has become a build priority because claim denials, payer complexity, administrative cost, prior authorization pressure, and staffing constraints are pushing healthcare organizations beyond rule-based automation. The global AI in RCM market was estimated at $20.63 billion in 2024 and is projected to reach $70.12 billion by 2030.
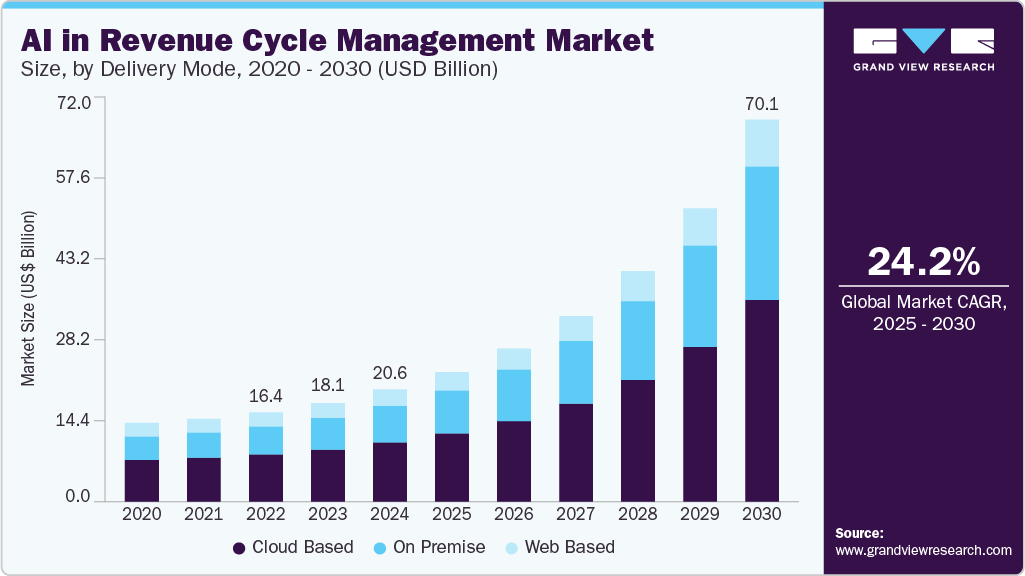
This rapid expansion proves that automated intelligence is no longer a luxury for hospital finance teams.
1. Market Pressures Driving Adoption
The modern billing landscape has become too volatile for static, rule-based systems to survive. Insurance companies update their guidelines continuously, creating an administrative maze that manual workflows cannot scale to meet.
- Explosive Market Growth: The industry is expanding at a 24.16% compound annual growth rate as health networks ditch legacy software.
- Rising Denial Complexity: Payer rules change daily, causing an unprecedented surge in revenue leakage from automated rejections.
- Staffing Constraints: A shortage of certified medical coders makes human chart review too slow and expensive to maintain.
- Regulatory Deadlines: Federal mandates are forcing a rapid migration toward open data sharing and instant verification systems.
These operational compounding pressures require technology leaders to move away from rigid if-then scripts entirely.
2. Core Strategic Focus Areas
According to industry research from McKinsey & Company (2023), generative language applications provide massive optimization potential because they handle text-heavy processes natively.
Engineering teams use this infrastructure to transform how administrative documents are reviewed and generated:
1. Clinical Documentation Improvement (CDI)
The platform runs clinical text summarization algorithms across long discharge summaries to ensure patient records match the true severity of care.
This alignment captures accurate risk scores and stops documentation omissions before billing submission.
2. Medical Necessity Narrative Generation
By analyzing unstructured clinical text processing layers, the software automatically matches doctor notes with internal hospital guidelines.
It drafts cohesive necessity statements that prove exactly why a specialized procedure or drug was ordered.
3. Appeal Letter Generation
When a claim gets rejected, the system interprets the explanation of benefits summarization payload to isolate the specific denial code.
It then drafts a highly targeted appeal letter cross-referenced with the patient’s actual chart data.
4. Electronic Prior Authorization
The platform connects with insurance portals via a FHIR document API to check approval rules instantly.
According to the Centers for Medicare & Medicaid Services (2026), impacted health insurance plans must implement and maintain standardized electronic prior authorization APIs by January 1, 2027.
This market shift creates a clear financial and regulatory opportunity, but only if teams define what GenAI should and should not own inside RCM. Transforming these manual administrative tasks into autonomous infrastructure allows health systems to lower their cost per claim while protecting their core cash flow.
What GenAI Can Safely Own Inside RCM Workflows
Generative AI can safely own RCM tasks that involve summarizing, drafting, extracting, comparing, and preparing information for review. It should not independently approve claims, finalize codes, override payer rules, or submit high-risk decisions without validation.
The safest early workflows include denial drafts, prior authorization letters, CDI prompts, EOB summaries, and coding suggestions.
A. Automation Boundaries by Risk Level
Instead of viewing AI as an all-or-nothing replacement for billing staff, engineering teams must deploy software using strict, risk-adjusted boundaries.
GenAI excels at text-heavy, operational tasks but lacks the deterministic logic required for final transactional submissions.
| RCM Workflow | GenAI Role | Human Review Needed? | Risk Level |
| Denial summary | Summarize the denial reason and next steps | Yes | Medium |
| Prior auth draft | Generate a medical necessity narrative | Yes | High |
| Coding support | Suggest ICD-10-CM / CPT options | Yes | High |
| EOB summary | Explain the payer decision | Sometimes | Medium |
| Claim appeal | Draft evidence-backed appeal | Yes | High |
| Payment posting notes | Summarize remittance mismatch | Sometimes | Medium |
B. Tasks GenAI Can Safely Support
The platform handles unstructured clinical language processing tasks with high accuracy, drastically shortening the time required to compile records.
1. Clinical text summarization
The model condenses multi-page health records into a single discharge summary analysis sheet, highlighting key clinical markers. This helps billing teams find specific treatments without reading raw text files manually.
2. Denial letter summarization
The platform runs explanation of benefits summarization scripts to find out exactly why a claim failed. It then executes an AI-assisted denial response drafting routine to build a customized, evidence-backed appeal document.
3. Prior authorization letter drafting
The software reviews the active chart against external payer guidelines to create a prior authorization letter drafting file. It automatically builds a clean medical necessity validation package to speed up approval processing timelines.
4. Payer correspondence automation
The system reads complex insurance letters and translates unstructured payer updates into clear tasks. If a chart lacks clear details, it runs automated physician query generation routines to get the right documentation from doctors.
5. Explanation of benefits
The platform parses raw insurance files and translates complex remittance data into structured output generation layers. This makes it easy for billing teams to spot payment mismatches and track financial adjustments.
C. Tasks GenAI Should Never Own Alone
High-risk operations require deterministic guardrails and strict validation layers before any data leaves the hospital network.
1. Final coding decisions
The platform must never make a final ICD-10-CM code suggestion or CPT code recommendation without a certified human coder checking the work. Automated outputs should serve as a coding audit trail, not a final submission file.
2. Prior authorization approval decisions
While AI can draft the medical necessity narrative generation files, it cannot legally approve a medical procedure or make final necessity determinations. A licensed clinician must review every document to protect patient care safety.
3. Payer-rule interpretation without retrieval
Models should never guess internal insurance rules from their base training weights, as this causes hallucination risks. Instead, use a strict retrieval-augmented generation framework linked directly to an updated local payer rules engine.
4. Human-in-the-loop RCM review
The architecture enforces human-in-the-loop RCM review by assigning a real-time confidence scoring metric to every output. If a draft falls below a set quality threshold, the software flags it for manual inspection.
5. Structured output generation
The software translates unstructured clinical text into clear JSON arrays while providing explainable AI recommendations. This ensures that every billing suggestion references specific pages and paragraphs inside the original medical chart.
Once the safe ownership boundary is clear, the real product opportunity sits in the claim narrative layer.
Where Generative AI Fits Across Revenue Cycle Workflows
Generative AI fits best in RCM workflows where staff already read, compare, summarize, justify, or draft information from clinical and payer documents.
The highest-value areas include CDI, coding assistance, prior authorization letters, medical necessity narratives, denial response drafting, appeal letter generation, EOB summarization, remittance advice interpretation, and payer correspondence automation.
1. Front-End RCM (Patient Intake & Approvals)
The front end of the billing cycle focuses entirely on gathering clean data and securing insurer approvals before a patient receives care.
This early stage is highly manual and relies on cross-checking complex doctor notes against changing insurance policy sheets.
- Insurance Verification Summaries: The platform reads long, messy policy documents from insurance portals and creates a simple, text-based coverage cheat sheet. This highlights exact copay amounts and deductible balances so front-desk staff do not have to hunt for them.
- Prior Authorization Letter Drafting: Instead of making humans write long letters to prove a patient needs a specific scan or drug, the software does it. It pulls data directly from the clinical chart to outline the patient’s medical history automatically.
- Documentation Requirement Extraction: The software scans incoming doctor orders and checks them against specific insurance rules. It then builds a clear checklist of what exact details or signatures are missing before the hospital schedules the visit.
- Medical Necessity Validation: The engine reads clinical charts to confirm that a planned treatment matches the insurance company’s internal guidelines. This active step spots and fixes coverage mismatches before the claim ever gets sent out.
2. Mid-Cycle RCM (Clinical Documentation & Coding)
Mid-cycle workflows translate actual patient care into standard, billable codes. This stage is highly text-heavy, meaning language models can directly accelerate how charts are reviewed and processed. (Source: BillingParadise, 2025)
- Discharge Summary Analysis: The model reviews massive, multi-page hospital exit summaries to extract every relevant medical event. It groups these details into clean, structured data lists that a human coder can scan in seconds.
- Clinical Documentation Improvement (CDI): The software runs constantly in the background to ensure clinical notes match the true severity of a patient’s illness. If a note looks too vague, it flags the file to protect the hospital’s risk adjustment scores.
- Physician Query Generation: When a doctor’s chart note lacks critical details needed for billing, the platform drafts a short, polite clarification note. This saves coding teams from spending hours typing custom emails to doctors.
- ICD-10-CM Code Suggestion: The engine reads unstructured clinical text and suggests the most accurate diagnostic codes for the bill. It acts as an assistant that speeds up human work while maintaining a clear audit trail.
- CPT Code Recommendation: The platform scans procedure notes to recommend the best treatment codes and billing modifiers. This prevents coders from missing small procedural details that could lead to an underpayment.
- HCC Risk Adjustment Automation: The software tracks chronic conditions across long patient histories to calculate accurate health status scores. This automation ensures the hospital gets fair reimbursement for managing highly complex cases.
3. Back-End RCM (Claims, Denials & Remittance)
The back end of the cycle handles billing submissions, tracks incoming payments, and fights insurance rejections. This layer is highly adversarial, requiring teams to build strong, text-based arguments against complex insurance claim denials.
- Denial Response Drafting: When an insurance company rejects a claim, the system reads the rejection code and finds the underlying issue. So, it immediately drafts a tailored response targeting the specific reason the payer gave.
- Appeal Letter Generation: The system builds detailed, evidence-backed appeal packets by pairing the original claim with the patient’s actual medical chart. This replaces hours of manual writing with a single click.
- EOB Summarization: The software translates complex explanations of benefits sheets into clear summaries. This highlights exactly how much the insurance paid, what was adjusted, and what amount rolls over to the patient.
- Remittance Advice Interpretation: The platform reads electronic payment sheets to find deep financial mismatches. So, it flags odd payment cuts or balance issues, so billing teams know exactly which accounts need attention.
- Underpayment Investigation Support: The engine compares the insurance company’s actual payment against the hospital’s original contract rules. So, if the payer shorted the check, the platform flags the underpayment and highlights the broken contract rule.
These use cases only become useful when the architecture can ground every generated answer in trusted clinical and payer evidence.
RAG for GenAI RCM Software
GenAI RCM software should usually start with RAG, structured prompts, rules engines, and human review before fine-tuning. RAG grounds outputs in clinical records and payer documents. Rules engines validate billing logic.
At the same time, fine-tuning becomes useful only when the team has enough approved examples, repeatable tasks, and clear evaluation criteria.
1. Core Architecture Components
Building a functional model stack requires separating unstructured language tasks from hard transaction rules.
A standalone model will hallucinate medical necessity codes, meaning engineering teams must wrap foundations in strict data retrieval and validation loops.
- RAG Pipeline for Clinical Documentation: The retrieval architecture reads active patient charts, converts the text into vector embeddings, and stores them locally. When drafting documents, it pulls exact sentence fragments to provide the active context window with fresh evidence.
- Foundation Model Healthcare Adaptation: Teams use larger open-weights foundations that undergo explicit adaptation training on massive clinical and biomedical texts. This step ensures the system naturally understands medical shorthand and structural chart layouts.
- LLM Fine-Tuning for Revenue Cycle: Fine-tuning modifies actual model weights to lock in explicit styling rules, rigid output lengths, and niche operational procedures. This method is used when the system must write in a highly specific brand voice across thousands of repeated accounts.
- Clinical NER Models: These specialized sequence-labeling models run named entity recognition routines across text blocks to extract clear items like drug names, dosages, and exact anatomical sites. They supply downstream billing tools with structured data points.
- NLP Clinical Language Understanding: This layer uses advanced natural language processing to infer relationships between separate chart notes. It confirms if a documented symptom directly supports a secondary procedure ordered later by a different physician.
2. Advanced Intelligence Layers
Moving beyond simple data extraction requires layers that handle multi-step reasoning, threat protection, and real-time risk scoring.
- Structured Output Generation: This layer wraps around inference engines to force models to return clean, machine-readable JSON payloads. It maps text responses directly to predefined data fields, preventing formatting errors from breaking downstream applications.
- Prompt Engineering for Healthcare: Engineering teams design complex prompt trees that contain explicit role definitions, negative constraints, and few-shot reasoning steps. These instructions keep the model strictly focused on administrative tasks.
- Payer Rules Engine: This deterministic validation layer checks generated data arrays against active payer policy rules. It serves as a hard mathematical wall that flags clear billing errors before they leave the application.
- Predictive Denial Models: These lightweight machine learning algorithms run alongside generative systems to score the rejection likelihood of an upcoming claim. If the risk score crosses a set limit, the platform pauses automation.
- Model Routing: A smart routing router evaluates incoming task complexity to select the cheapest, fastest model for the job. On the other hand, simple text translations go to small models, while multi-stage charts route to larger engines.
3. Strategy Evaluation Framework
The table below breaks down the optimal engineering approaches for primary revenue cycle development tracks based on data complexity and execution risk.
| Model Approach | Best For | RCM Example | Risk If Misused |
| RAG | Evidence-backed generation | Appeal letter with payer policy citations | Bad retrieval creates bad output |
| Fine-tuning | Repeated output style and task patterns | Specialty-specific coding rationale | Can memorize weak patterns |
| Clinical NLP | Entity extraction | Diagnosis, procedure, and medication extraction | Misses context if used alone |
| Rules engine | Hard validation | NCCI edits, payer rules, claim checks | Cannot draft narratives |
| Predictive ML | Risk scoring | Denial likelihood prediction | Needs clean historical labels |
| LLM orchestration | Multi-step reasoning | PA draft + evidence + review queue | Needs guardrails and monitoring |
Our technical governance practices mirror leading industry benchmarks. The National Institute of Standards and Technology (2024) Generative AI Profile emphasizes risk management across the AI lifecycle, which supports evaluation, governance, monitoring, and deployment controls for generative AI systems.
Following these core lifecycle steps prevents platform drift, guards against prompt injections, and guarantees complete system observability.
The model stack only works when the underlying architecture can move clinical, payer, and financial data safely.
GenAI RCM Architecture From EHR Data to Reviewer Action
A GenAI RCM architecture needs ingestion, normalization, retrieval, orchestration, validation, review, and monitoring layers.
At the same time, the platform must connect EHR documents, FHIR resources, HL7 CDA files, EDI 837/835 transactions, payer policies, coding edits, and work queues before it generates or recommends anything inside revenue workflows.
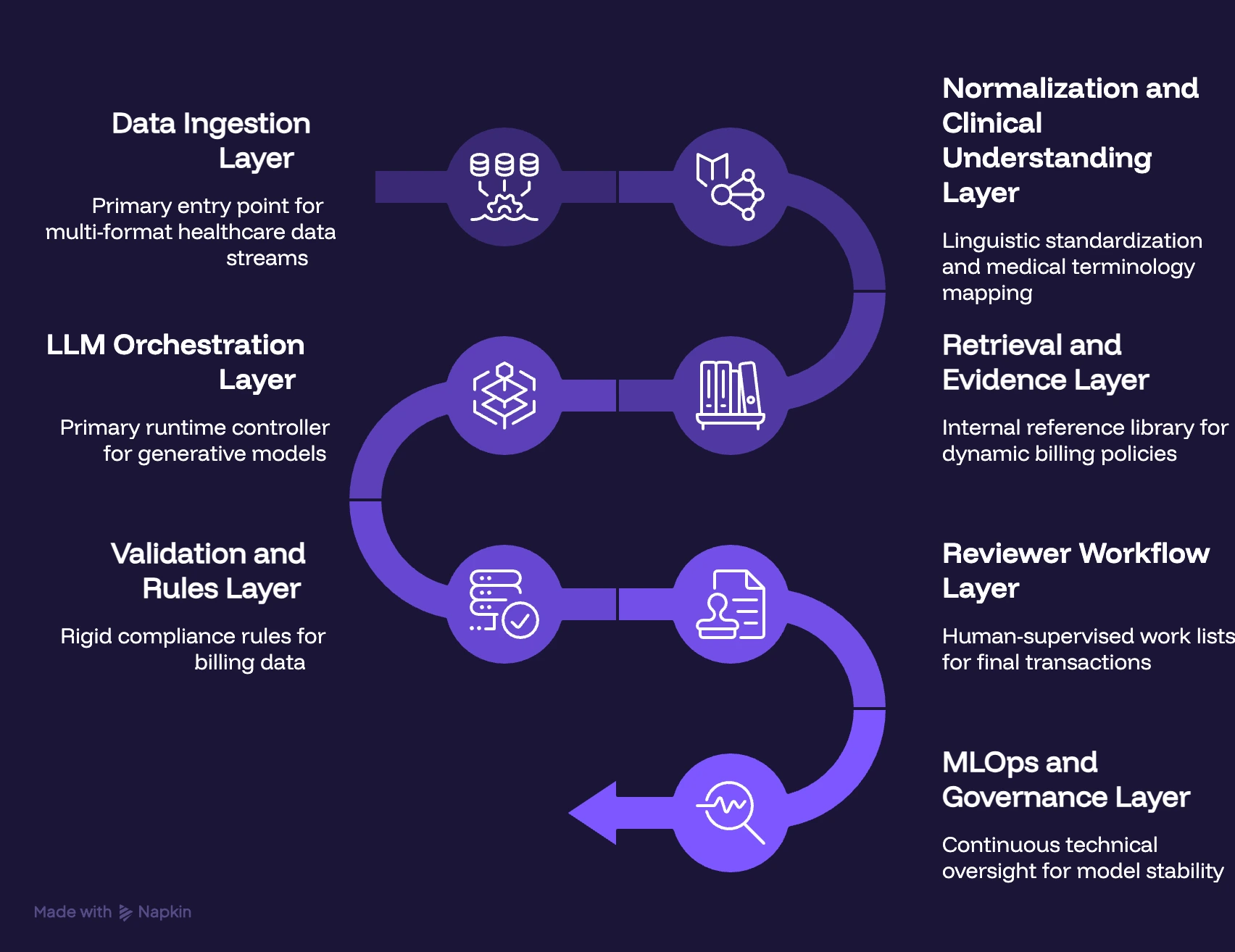
1. Data Ingestion Layer
The ingestion pipeline functions as the primary entry point for multi-format healthcare data streams. It continuously pulls information from internal clinical databases, structured standard files, and external insurance interfaces.
- EHR Data Extraction: Automated cron tasks run background scripts to fetch real-time updates directly from the provider database.
- FHIR Document API: The software leverages REST endpoints to stream standardized, resource-mapped clinical information without disturbing database performance.
- HL7 CDA Integration: Background listeners capture and parse Continuity of Care Documents containing vital patient medical history.
- EDI 837 Claim Ingestion: The engine breaks down outbound billing transaction files to analyze exact line-item records before submission.
- EDI 835 Remittance Ingestion: Incoming electronic payment files drop directly into the parser to extract precise payment and adjustment codes.
- Payer Portal Data: Headless web tools automatically scrape and download real-time approval records from external insurance web spaces.
- Prior Authorization Documents: The storage bucket organizes incoming insurance approval slips, matching them against open provider orders.
- Uploaded PDFs and Scanned Documents: Optical character recognition tools scan paper clinical chart copies, turning flat images into editable text strings.
2. Normalization and Clinical Understanding Layer
Raw data from disparate channels arrives completely unformatted and requires linguistic standardization. This layer parses messy text fragments into clean, contextually organized medical terminology maps.
- Unstructured Clinical Text Processing: Heavy linguistic cleaning scripts strip out layout artifacts, note formatting errors, and unreadable doctor shorthand.
- Clinical NER Models: Named entity recognition tools identify specific medical categories like active diagnoses, procedures, and drug dosages.
- Patient-Encounter Matching: Smart deterministic logic uses basic identity variables to link loose clinical notes with specific billing accounts.
- Service-Line Tagging: The platform categorizes extracted medical procedures under broad hospital departments like radiology or emergency care.
- Provider, Facility, Payer, and Plan Mapping: The software maps unique doctor IDs and insurance policy numbers to internal tracking files.
3. Retrieval and Evidence Layer
A standalone language model cannot reliably guess dynamic billing policies without hallucinating. This layer acts as an internal reference library, feeding active context into the model window.
- RAG Pipeline for Clinical Documentation: The system indexes patient charts into vector structures, making it easy to fetch matching medical records.
- Payer Policy Retrieval: Local storage buckets continuously index active insurance rules documents gathered from commercial web portals.
- Medical Necessity Criteria: The software organizes clinical evidence alongside active national coverage guidelines to prove treatment validity.
- Coding Guidelines: Up-to-date manuals are indexed into searchable databases to verify specific code bundling constraints.
- Denial Reason Mappings: Rejection code indexes map raw numbers to human-readable explanations to help shape downstream arguments.
- Document Version Control: The storage system tracks policy document changes to ensure appeals are judged against historical rules.
4. LLM Orchestration Layer
The orchestration layer acts as the primary runtime controller for all deployed generative models. It manages how text prompts are styled, tracks execution costs, and controls active model behavior.
- Prompt Routing: A smart gateway routes simple text translations to small engines while directing multi-step chart reviews to larger instances.
- Structured Output Generation: The system uses strict schema validation rules to force models to return clean machine-readable JSON payloads.
- Model Grounding: System instructions force language models to use only the facts provided in the retrieved reference text.
- Confidence Scoring: The platform prints a mathematical score alongside every draft, indicating the model’s certainty level.
- Tool Calling: Advanced APIs allow the language model to query external database indices when it needs fresh information.
- Output Formatting: Specialized modules clean up raw text outputs, removing stray characters before delivering drafts to the user interface.
5. Validation and Rules Layer
Even the most grounded language models require hard mathematical checks before transmitting billing data. This layer applies rigid compliance rules to catch errors before they exit the platform.
- NCCI Edit Validation: The system runs automated logic checks to catch unbundled or conflicting procedure combinations instantly.
- Payer Rules Engine: This validation filter checks every generated claim against known insurance exclusions to prevent preventable rejections.
- Medical Necessity Validation: Software rules check that the recorded diagnosis code perfectly justifies the specific procedure billed.
- Prior Authorization Requirement Checks: The platform confirms that high-cost treatments are backed by a valid insurer approval token.
- CARC/RARC Mapping: The engine translates claim adjustment reason codes into clear, actionable tasks inside the billing workspace.
6. Reviewer Workflow Layer
The system avoids automated submissions by routing all generated outputs into human-supervised work lists. This approach keeps human specialists in complete control of the final financial transactions.
- Human-in-the-Loop RCM Review: The interface places generated appeal drafts alongside original medical charts for mandatory human verification.
- Coding Audit Trail: A clear visual sidebar displays the exact source page and paragraph used to justify each code suggestion.
- Exception Queues: If an output receives a low confidence score, the system routes the file into a manual priority queue.
- Reviewer Comments: Billing specialists can type custom correction notes directly into the application to edit drafts quickly.
- Approval and Rejection Tracking: The database logs every time a user accepts or edits an AI suggestion to build internal performance data.
7. MLOps and Governance Layer
Deployed enterprise models require continuous technical oversight to ensure long-term stability and cost efficiency. This final operational layer tracks pipeline health, processing latency, and security anomalies.
- MLOps for Generative AI: Automated pipelines manage code deployment tracking, asset tracking, and software testing across staging environments.
- Model Drift Monitoring: Monitoring tools track output distributions over time, flagging if response quality drops after vendor model upgrades.
- Prompt Injection Controls: Security filters inspect incoming text data fields to neutralize rogue user commands before inference.
- LLM Guardrails: Real-time semantic layers block the generation of inappropriate text, keeping outputs professional and compliant.
- Healthcare-Specific LLM Evaluation: Automation metrics score draft quality against expert-approved training charts to verify medical accuracy.
- Token Cost Optimization: Prompt caching mechanisms save frequently used policy context to lower infrastructure costs.
- Inference Latency Monitoring: Real-time trackers alert engineers if database or model pipelines slow down during peak usage hours.
This architecture also defines where PHI can leak if the system is designed carelessly.
How to Build a Generative AI Revenue Cycle Platform
Building a generative AI revenue cycle platform requires five components: a fine-tuned clinical LLM, a payer rules engine, a RAG layer for policy retrieval, an EHR integration framework, and a human-in-the-loop review layer.
This architecture handles coding, prior authorization, denial appeals, and remittance interpretation, with audit control at every stage.
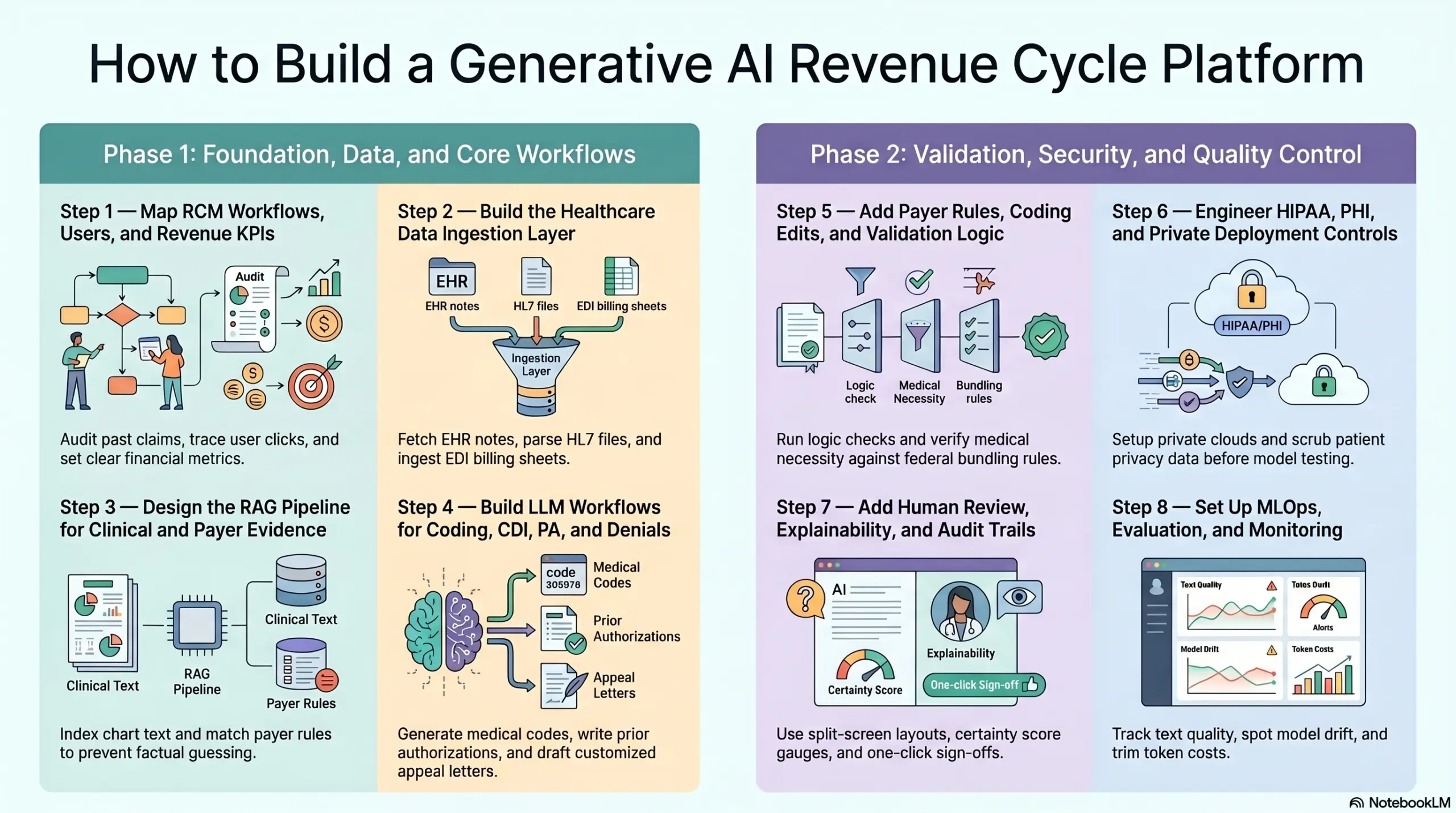
Step 1 — Map RCM Workflows, Users, and Revenue KPIs
We anchor early project discovery around your current operational realities rather than model selection.
At the same time, our team works to map out systemic revenue leakage points, explicit user decision nodes, cross-system handoffs, internal compliance approval gates, and individual KPI ownership parameters before establishing your technical architecture plans.
- Tracking Cash Leakage: We audit your past claims data to find exactly where you lose money, such as missing chart notes or slow code tracking.
- Mapping User Clicks: We trace every single step your billers and coders take to find where they spend the most time reading or typing.
- Fixing Team Handoffs: We document how data moves from the front desk to the coding team so information never drops through the cracks.
- Locating Checkpoints: We pinpoint the exact spots where a human manager must check a document before it goes out to an insurance portal.
- Setting Financial Goals: We tie every software feature directly to a clear metric, like reducing your days in accounts receivable or cutting your cost per claim.
What goes wrong if skipped: The platform becomes a generic text interface that produces nice essays but does not reduce denials, shorten payment cycles, or cut down on manual rework.
Once the workflow is scoped, the platform needs reliable healthcare data access.
Step 2 — Build the Healthcare Data Ingestion Layer
We design your core ingestion architecture around production-grade communication channels, preparing integrations early to manage the unique data formats of legacy clearinghouses, commercial payer web portals, and external financial packages.
- EHR Note Fetching: We build automated background pipelines to pull fresh patient notes and doctor charts straight from your medical databases.
- FHIR Link Streaming: We use standardized healthcare web links to stream patient data securely without slowing down your active hospital networks.
- HL7 File Parsing: Our tools open and read standard continuity documents to gather past medical histories automatically.
- EDI File Breakdown: We ingest standard billing files like insurance claims and remittance sheets to track every dollar billed and paid.
- Portal Data Scraping: We run automated tools to grab and compile up-to-date insurance rules and coverage sheets from payer websites.
What goes wrong if skipped: The language model generates convincing but completely wrong recommendations because it cannot see the full clinical, coding, or payment history.
After ingestion, the platform needs a retrieval design so every generated output has evidence.
Step 3 — Design the RAG Pipeline for Clinical and Payer Evidence
We build your retrieval architecture as a strictly governed evidence verification layer, avoiding simple, unmonitored vector store connections. Our pipelines are engineered to actively filter records by the exact commercial payer, specific insurance plan, state-level regulations, clinical specialties, encounter dates, and user access levels.
- Chart Text Indexing: We break long, complex medical files into tiny, searchable text pieces and store them in a secure local database.
- Smart Content Fetching: When you need a document drafted, our search engine grabs only the specific paragraphs that apply to that exact case.
- Payer Rules Matching: We sort and index commercial insurance coverage books by plan type and date to keep your appeals accurate.
- Source Label Mapping: The system attaches an electronic tag to every text fragment, tracking its exact source file name and page number.
- Context Window Delivery: We package the fetched text facts neatly and feed them directly into the language model to prevent factual guessing.
What goes wrong if skipped: The model may hallucinate coverage rules, cite outdated policy language, or generate appeal arguments that fail an audit.
With evidence retrieval in place, the build can move into workflow-specific LLM features.
Step 4 — Build LLM Workflows for Coding, CDI, PA, and Denials
We build each specialized language pipeline around matching user interaction screens, version-controlled edit histories, and clean API handoffs into your core billing software.
- Medical Code Generation: The platform reads doctor narratives to suggest precise diagnostic and procedure codes directly inside the coder’s screen.
- Documentation Improvement Tracking: The software runs in the background to flag vague chart notes that might cause an insurance rejection later.
- Prior Authorization Writing: The system uses chart evidence to draft clear approval requests for high-cost treatments automatically.
- Appeal Letter Drafting: When a claim fails, the tool combines your chart data and payer rules to write a customized appeal packet.
- Insurance Update Summarization: The language engine translates long, complex payment explanations into plain text notes for your billing staff.
What goes wrong if skipped: The platform may process documents in the background but fails to deliver clear, useful outputs inside daily work queues.
For a deeper breakdown of coding workflows, see our guide on How to Build an AI Medical Coding Platform.
Generated outputs still need hard validation before they influence claims or appeals.
Step 5 — Add Payer Rules, Coding Edits, and Validation Logic
We isolate your generative language workflows from your hard transaction validation layers. This approach allows the system to utilize natural language capabilities for drafting tasks while preserving absolute, audit-ready deterministic control over your final billing numbers and payer submissions.
- Logic Check Engine: We run every suggested code and text draft through hard math rules to catch obvious errors instantly.
- Bundling Rule Checks: The software verifies your code combinations against federal guidelines to stop you from billing overlapping items.
- Necessity Proof Verification: We check that the listed patient illness code completely justifies the expensive medical procedure being billed.
- Token Match Validation: The tool checks that your high-cost bills are linked to a verified prior approval number before submission.
- Warning Sign Alarms: We use soft warnings for tiny typos but apply hard stops that send broken files straight to human exception lists.
What goes wrong if skipped: The system drafts highly polished but completely non-compliant letters that increase your denial risk instead of reducing it.
Validation protects accuracy, but compliance protects whether the platform can run at all.
Step 6 — Engineer HIPAA, PHI, and Private Deployment Controls
We build enterprise data security safeguards directly into your core system layout before any model testing starts. Our team establishes precise patient data flow maps, role-based access rules, network deployment boundaries, and complete audit tracking systems from day one of development.
- Private Cloud Setup: We install open-weights models inside your own secure virtual cloud, so your data never gets shared with public tools.
- Patient Privacy Scrubbing: The software strips out names, birthdays, and social security numbers, swapping them with safe reference keys.
- Data Lock Encryption: We encrypt all clinical records and text prompts whether they are sitting in storage or traveling across networks.
- User Guard Controls: We tie system access directly to strict role rules, ensuring staff only see data needed for their active tasks.
- Audit Trail Collection: The platform logs every single prompt, search query, and model answer to give compliance teams unalterable usage logs.
What goes wrong if skipped: Security becomes a massive blocker before launch, and your risk of a sensitive patient data leak increases across prompts, logs, and summaries.
Even with secure deployment, the platform still needs human review to control clinical and financial risk.
Step 7 — Add Human Review, Explainability, and Audit Trails
We build your review screens to fit directly into your team’s existing revenue workflows rather than forcing staff to run a separate standalone tool.
- Split-Screen Layouts: We display the AI-written draft right next to the original patient chart so reviewers do not have to flip tabs.
- Evidence Highlight Sidebars: The system highlights the exact book paragraph and chart page used to back up every billing suggestion.
- Certainty Score Gauges: We print a real-time confidence percentage next to each draft so workers know which files need a close look.
- Change History Loggers: The database tracks every single edit a human worker makes to the text, keeping a clean record of changes.
- One-Click Sign-Offs: Once a specialist clicks approve, the platform packages the file and drops it straight into your billing stream.
What goes wrong if skipped: Workers either trust the AI completely without checking or ignore it entirely, which destroys your return on investment.
For a deeper breakdown of denial workflow design, see our guide on AI Denial Prediction Software Development for Hospitals.
Human review controls decisions today, while MLOps controls system quality over time.
Step 8 — Set Up MLOps, Evaluation, and Monitoring
We treat long-term platform monitoring as a core component of your system architecture, deploying performance tracking screens that monitor model behavior and financial KPIs side by side.
- Text Quality Tracking: The platform runs continuous comparison checks to ensure your AI summaries remain accurate and readable.
- System Shift Spotters: We monitor live outputs over time to catch model drift if a vendor updates their core software parameters.
- Rogue Prompt Blockers: We insert security filters to block unauthorized user inputs and stop malicious commands from disrupting loops.
- Token Cost Trimmers: Our systems use smart context caching tools to reuse policy data, preventing expensive repeat model bills.
- Incident Log Files: The software tracks system latency and dropped connections so your IT team can maintain sub-second response times.
What goes wrong if skipped: A model that works perfectly during a pilot can degrade quickly when insurance companies update their coverage rules or text patterns shift.
The final build decision usually comes down to cost, timeline, and scope.
Generative AI RCM Platform Development Cost
Generative AI RCM platform development usually costs $60,000–$200,000, depending on workflow scope, data readiness, EHR integrations, payer connectivity, LLM architecture, RAG depth, HIPAA controls, private deployment, MLOps, and reviewer workflows.
The higher range applies when the platform needs deeper healthcare integrations, PHI-safe model hosting, payer-policy retrieval, reviewer dashboards, audit trails, and production monitoring.
This matters because HHS requires covered entities and business associates to protect ePHI through administrative, physical, and technical safeguards.
Cost Breakdown by Development Phase
| Development Phase | Estimated Cost | What It Covers |
| Product discovery and RCM workflow mapping | $5,000–$12,000 | Workflow scope, user roles, revenue leakage analysis, MVP roadmap |
| UX/UI for billing and reviewer teams | $7,000–$18,000 | Work queues, dashboards, review screens, approval flows |
| Data ingestion and normalization | $10,000–$28,000 | Clinical notes, claims data, remittance files, payer documents |
| EHR, clearinghouse, and payer integrations | $12,000–$45,000 | EHR data, FHIR APIs, HL7 CDA, EDI 837/835, payer connectivity |
| RAG pipeline and document intelligence | $10,000–$35,000 | Document chunking, embeddings, retrieval, source grounding, payer-policy indexing |
| LLM workflow development | $12,000–$40,000 | PA drafts, denial responses, appeal letters, coding support, CDI prompts |
| Payer rules and validation logic | $8,000–$25,000 | Medical necessity checks, NCCI edits, claim validation, denial-code mapping |
| HIPAA security and access controls | $8,000–$25,000 | PHI controls, RBAC, audit logs, encryption, secure deployment setup |
| MLOps, testing, and monitoring | $8,000–$22,000 | Model testing, prompt monitoring, drift checks, latency, and token cost tracking |
| Deployment and go-live support | $5,000–$15,000 | QA, UAT, rollout support, documentation, team training |
Cost by Build Type
| Build Type | Estimated Cost | Best For |
| GenAI RCM proof of concept | $60,000–$90,000 | One narrow workflow, limited integrations, controlled pilot |
| Focused MVP | $90,000–$140,000 | One production workflow with reviewer screens and basic RAG |
| Production GenAI RCM platform | $140,000–$200,000 | Integrated workflow with PHI controls, validation logic, and monitoring |
- A $60,000–$90,000 proof of concept works when the goal is to validate one workflow before committing to a larger build. For example, a healthtech founder may test denial letter summarization or prior authorization draft generation using a controlled dataset and limited reviewer access.
- A $90,000–$140,000 MVP is more practical when the system needs to support real users. This version usually includes workflow-specific dashboards, RAG-backed document retrieval, structured LLM outputs, source references, human review, and basic audit logging.
- A $140,000–$200,000 production platform is the better fit when the product must connect with EHRs, clearinghouses, payer data, or billing systems. CMS’s interoperability and prior authorization final rule also increases the importance of API readiness for payer-provider workflows, especially as required API implementation dates move into 2027.
What Pushes the Cost Higher?
The biggest cost driver is not the LLM itself. It is the surrounding infrastructure that makes the output safe, useful, and auditable.
Costs increase when the platform needs:
- Multiple EHR, FHIR, HL7, or EDI integrations.
- A payer-specific RAG pipeline with policy versioning.
- Private model hosting or on-premise deployment.
- PHI de-identification and tokenization.
- Reviewer dashboards with role-based permissions.
- Human-in-the-loop approval workflows.
- Payer rules, medical necessity, and NCCI validation.
- Model monitoring, prompt logging, and drift detection.
- Multi-tenant architecture for SaaS buyers.
NIST’s Generative AI Profile also emphasizes lifecycle risk management for GenAI systems, which makes monitoring, evaluation, and governance important parts of production planning rather than optional add-ons.
Ongoing Maintenance Cost
Ongoing maintenance usually costs 18%–30% of the initial build cost per year. For a $120,000 MVP, that means roughly $21,600–$36,000 annually for model monitoring, payer-rule updates, prompt improvements, integration maintenance, security reviews, and feature refinements.
This maintenance budget matters more in GenAI RCM than in a standard admin tool. Payer policies change, documentation patterns shift, denial reasons evolve, and LLM behavior needs regular evaluation.
Building a GenAI RCM platform without a cost model can lead to scope creep fast. Intellivon helps healthcare SaaS founders, RCM companies, and digital health teams define the right workflow scope, architecture, integrations, compliance controls, and MVP roadmap before development begins.
How to Reduce Hallucination Risk in Clinical and Billing AI
Hallucination risk in clinical AI drops when the platform grounds outputs in retrieved evidence, limits model freedom, validates structured fields, uses confidence thresholds, and routes uncertain cases to human reviewers.
For RCM, the system should never let an LLM invent payer rules, diagnosis support, coding rationale, or appeal evidence.
1. Technical Risk Controls
Mitigating hallucination risk in clinical AI requires technical layers that restrict model freedom and force adherence to factual source documents. If left unguarded, foundation models will invent codes or insurance policies, which break billing compliance and increase liability.
- Model Grounding and RAG: The platform uses retrieval-augmented generation to feed real-time patient charts and active payer policies directly into the prompt context. This setup forces the model to draw its answers exclusively from the provided text blocks.
- Prompt Engineering for Healthcare: System instructions include strict negative constraints, explicitly telling the model to output “Information Not Found” instead of guessing when context is missing.
- Structured Output Generation: We apply schema enforcement tools to guarantee the model returns clean JSON data fields rather than unpredictable, free-form text narratives.
- Confidence Scoring: Every text recommendation receives a mathematical score based on token probabilities, allowing the platform to gauge its own reliability before presenting data to users.
- Human-in-the-Loop Review: The software automatically routes drafts with low certainty scores into manual exception queues for human review.
2. Process Auditing Safeguards
Continuous evaluation and hard runtime gates prevent deployed applications from drifting or introducing bad formatting into your downstream billing pipelines.
- Source Citations in Generated Drafts: The user interface displays inline hyperlinks next to every code suggestion, tracing back to exact page numbers in the chart.
- Guardrails for Payer Policy and Coding Logic: Generated payloads pass through an independent, code-based verification layer to double-check bundling rules and exclusion lists.
- Prompt Injection Controls: Ingestion tools strip out hidden text commands from uploaded records to stop unauthorized model behavior.
- Pre-Deployment Testing: Development pipelines run automated test batteries across thousands of historical charts to score accuracy prior to launch.
- Clinical Accuracy Benchmarking: Engineers track system output using specialized language comparison metrics to verify text summaries stay close to human baselines.
Following standard safety rules preserves long-term platform trust. The National Institute of Standards and Technology (2024) Artificial Intelligence Risk Management Framework outlines clear parameters for pre-deployment validation, model testing, and continuous monitoring.
These governance steps protect billing platforms from logical drift and keep system actions transparent.
Once risk controls are defined, leadership can decide whether to build custom software or buy an existing tool.
Build GenAI Healthcare Revenue Cycle Platform With Intellivon
Intellivon helps healthcare SaaS founders, RCM companies, health systems, and digital health teams build GenAI healthcare revenue cycle platforms around real workflows.
The work should begin with scope, architecture, compliance controls, integration planning, model design, human review, MLOps, and revenue KPIs before full development begins.
1. Define the Right GenAI RCM Automation Scope
Intellivon helps teams choose the first GenAI RCM workflow by mapping revenue leakage, claim volume, denial patterns, reviewer capacity, and integration effort. The roadmap covers MVP planning, workflow prioritization, build vs buy decisions, and ROI assumptions before development starts properly.
2. Design the Platform Architecture Around RCM Operations
Intellivon designs the platform around RCM operations, not isolated AI features. The architecture covers microservices, event-driven workflows, EHR, FHIR, HL7, and EDI integrations, data normalization, reviewer queues, and audit-ready system design for healthcare revenue teams and leaders.
3. Build LLM Workflows That Revenue Teams Can Trust
Intellivon builds LLM workflows that generate structured, evidence-backed outputs for review. The model layer can include clinical NLP, RAG pipelines, LLM orchestration, confidence scoring, and source-linked recommendations for coding, CDI, prior authorization, denials, appeals, and payment workflows.
4. Make GenAI RCM Secure and Monitorable
Intellivon designs GenAI RCM platforms with HIPAA-ready architecture, PHI controls, role-based access, audit logs, model monitoring, guardrails, and prompt injection controls. This helps teams manage security, output quality, drift, latency, and model behavior after launch in production.
If you are planning to build generative AI for RCM software development around coding, CDI, prior authorization, denials, appeals, or payment workflows, Intellivon can help you define the roadmap before development begins.
The strongest GenAI RCM platforms are built with workflow discipline, not model-first experimentation.
Conclusion
Deploying a custom revenue platform transforms your administrative processing from a manual bottleneck into a scalable financial infrastructure. So, by anchoring your data ingestion pipelines, retrieval systems, and human verification screens in strict compliance controls, your organization can permanently plug revenue leaks, bypass changing payer walls, and protect cash flow.
Additionally, partnering with an experienced development firm guarantees that your custom software workspace is engineered for long-term production stability.
Things To Know About Generative AI Revenue Cycle Management
Q1. How much does genAI RCM platform development cost?
A1. Generative AI RCM platform development usually costs $140,000–$900,000+. At the same time, a focused MVP for denial response drafting, prior authorization letters, or coding assistance may cost $140,000–$280,000. Additionally, a full enterprise platform with EHR integrations, RAG, HIPAA controls, private deployment, MLOps, and multi-tenant architecture can exceed $450,000–$900,000.
Q2. How long does it take to build a genAI revenue cycle platform’s capabilities?
A2. A focused MVP usually takes 4–7 months. At the same time, a production-grade platform for one major workflow takes 7–12 months. Specifically, a multi-workflow enterprise built with EHR integration, payer rules, RAG, LLM evaluation, HIPAA controls, and MLOps usually takes 12–18 months.
Q3. Can LLM revenue cycle management software use PHI safely?
A3. Yes, LLM revenue cycle management software can use PHI safely when the architecture controls prompts, logs, embeddings, outputs, APIs, and reviewer access. At the same time, the platform needs encryption, RBAC, audit trails, BAA coverage, PHI minimization, private inference, and retention policies. Additionally, the HHS requires safeguards for electronic protected health information.
Q4. What integrations are required to develop an LLM-powered RCM platform workflow?
A4. To develop LLM-powered RCM platform workflows, plan for EHR, FHIR, HL7 CDA, EDI 837, EDI 835, clearinghouse, payer API, billing system, document repository, identity, and reporting integrations. Additionally, CMS’s prior authorization rule also increases the importance of API readiness for payer-provider data exchange.
Q5. Can generative AI medical coding software replace coders?
A5. Generative AI medical coding software should assist coders before it replaces coders. Additionally, It can suggest ICD-10-CM, CPT, HCPCS, and HCC codes, but complex charts still need sequencing logic, payer awareness, documentation judgment, and audit review. At the same time, coders expect AI to support suggestions and error checks, not remove human judgment entirely.



