

Key Takeaways:
-
AI RCM platforms connect eligibility, coding, claims, denial prevention, payments, and analytics for hospitals.
-
EHR integrations, FHIR R4 APIs, payer-rule logic, and EDI 837/835 workflows are foundational requirements.
-
NLP, predictive denial models, human-in-the-loop review, and MLOps monitoring ensure long-term platform accuracy.
-
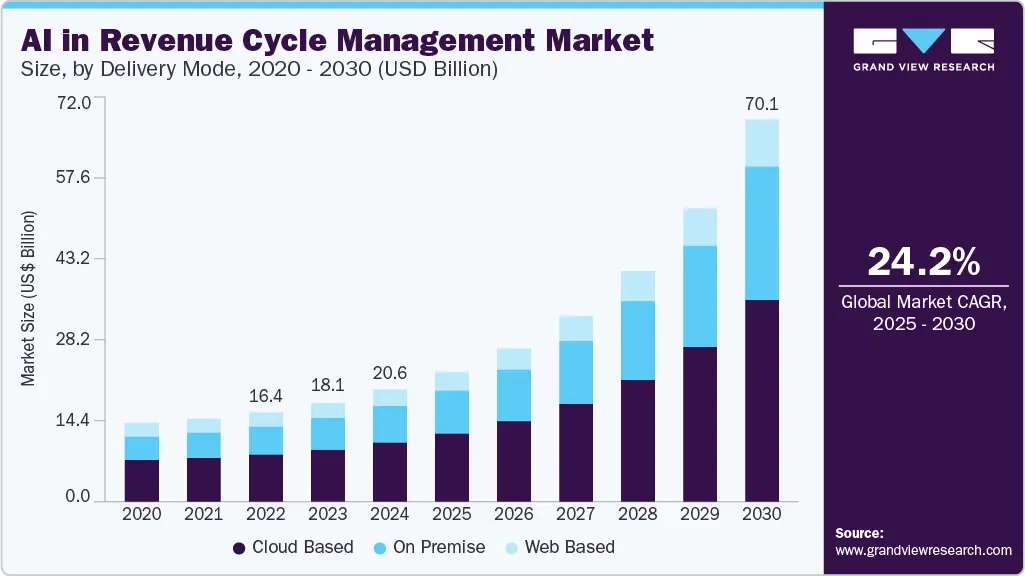
Custom hospital RCM builds cost $50,000 to $170,000, depending on AI depth and integration scope.
-
How Intellivon builds AI RCM platforms as a compliant revenue infrastructure designed specifically for hospital operations.
An AI revenue cycle management platform for hospitals is a system that unifies patient, clinical, coding, payer, and financial data across all service lines, and then applies AI to reduce denials, accelerate payment, and close revenue gaps at scale. Hospitals need this because their revenue cycle spans inpatient, outpatient, surgical, and emergency workflows at the same time, and no single billing tool has ever been built to handle that range.
The reason hospital AI RCM implementations fall short is the data layer sitting underneath it. When patient, clinical, and payer data live in fragmented systems across departments, the AI works from incomplete information, and revenue decisions get made with false confidence. Building the platform data-first, with a unified normalization layer before any AI model touches the data, turns $18 billion of the $25.7 billion hospitals spend annually on unnecessary claims adjudication into recoverable revenue.
With years of experience, Intellivon has built AI RCM platforms for hospital workflows with a data-unification-first architecture. This is the foundation that makes AI reliable across every service line and payer contract you operate. This blog covers platform architecture, data layer requirements, AI model selection, payer integration specs, HIPAA controls, and real development cost ranges, so you walk away with a build plan you can actually use.

What Is an AI RCM Platform for Hospitals?
An AI revenue cycle management platform is specialized software that uses machine learning and clinical NLP to automate hospital financial workflows. The system manages the entire revenue lifecycle across inpatient and outpatient settings by processing facility and professional claims.
It directly handles complex payer edits, denial predictions, and remittance processing to optimize net collection rates.
The End-to-End AI RCM Workflow
An enterprise AI platform operates across the entire patient encounter, transforming unstructured operational and clinical data into clean institutional claims.
The system automates tasks sequentially from patient intake through final payment posting to eliminate operational leakage.
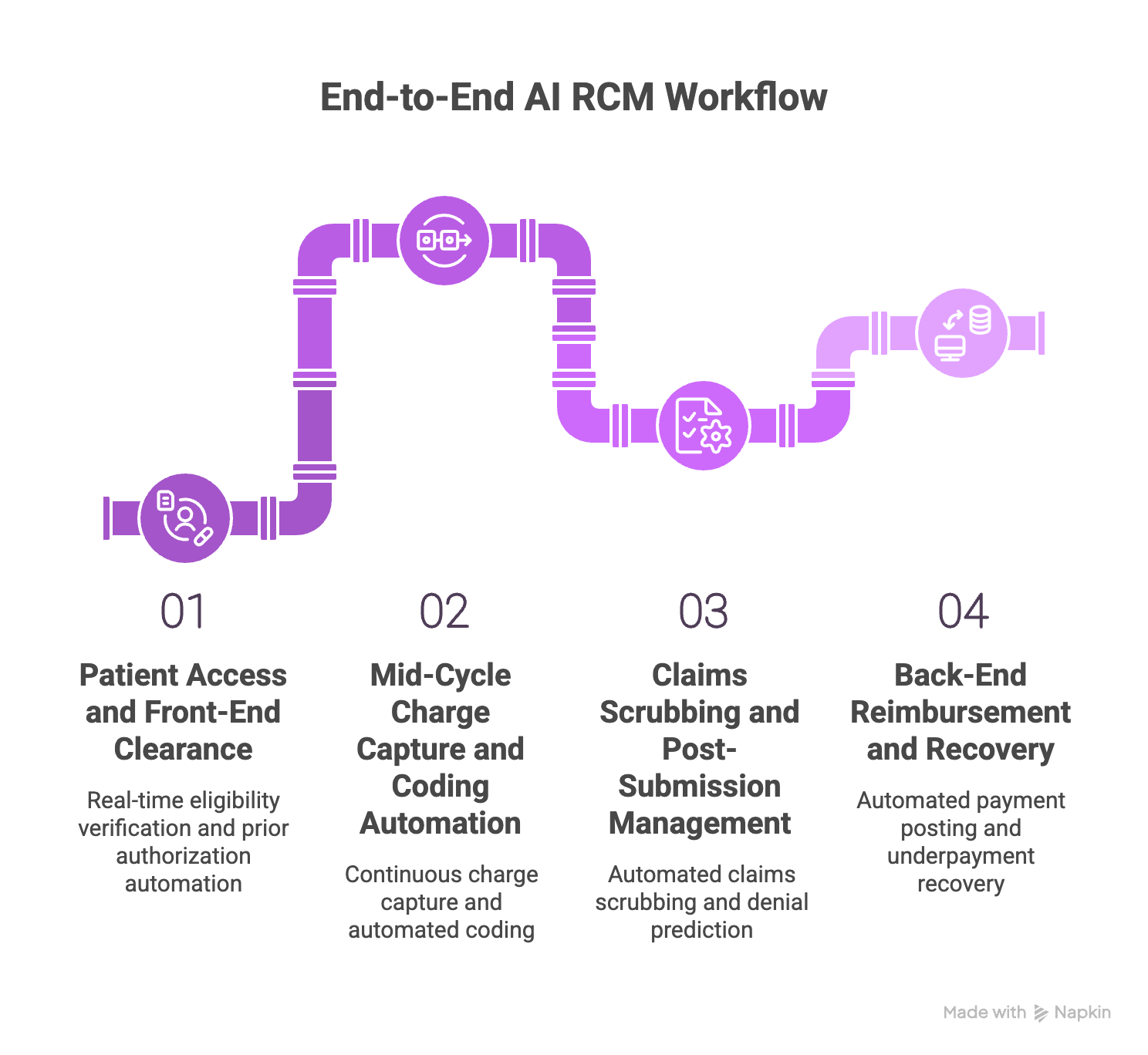
1. Patient Access and Front-End Clearance
The platform initiates automation at registration by executing real-time eligibility verification at patient access. The system ingests HL7 ADT messages to extract insurance details and confirm coordination of benefits, establishing immediate patient financial clearance.
Simultaneously, a clinical NLP model automates the prior authorization for hospital procedures by cross-referencing clinical notes against specific payer policies.
2. Mid-Cycle Charge Capture and Coding Automation
The system runs continuous charge capture automation by monitoring the EHR to ingest provider documentation and lab results. This real-time analysis flags missing charges against the hospital charge description master (CDM) to optimize the case mix index.
The platform then uses transformers to automate ICD-10-CM inpatient coding, ICD-10-PCS procedure coding, and CPT code assignment.
3. Claims Scrubbing and Post-Submission Management
Before submission, an automated hospital claims scrubbing engine evaluates the institutional claim against NCCI edits, LCD, and NCD rules.
This medical necessity validation step calculates a confidence score before routing the EDI 837I file to the clearinghouse. If flagged, a denial prediction model executes an automated denial root cause analysis on the incoming EDI 835 remittance.
4. Back-End Reimbursement and Recovery
The final stage accelerates cash flow through advanced payment posting automation by matching remittances to the patient accounting system ledger.
Concurrently, the engine runs underpayment recovery workflows by cross-referencing posted amounts against digitized payer contracts. This verification detects variances and opens recovery claims automatically, driving down days in AR and accelerating the net collection rate.
A hospital AI RCM platform should act as a control layer across clinical, financial, and payer workflows. The value comes from preventing revenue defects before claims move downstream. That means the next section should separate platform infrastructure from ordinary billing automation.
[To learn more about how automated claims scrubbing works in a hospital RCM system, read our blog on AI Claims Scrubbing Software Development for Healthcare. ]
AI RCM Platform vs Traditional Billing Software
Traditional hospital billing software records financial work after a medical event happens. An AI revenue cycle management platform evaluates the entire event while it is still easy to fix. It instantly flags missing eligibility data, weak clinical records, wrong DRG logic, and denial probability before the claim goes to the payer.
1. Understanding the Structural Differences
To see how these systems differ, it helps to compare their main features side by side. Traditional tools wait for human input, while intelligent systems work in the background to stop billing mistakes.
| Capability | Traditional Hospital Billing Software | AI Revenue Cycle Management Platform |
| Workflow control | Static queues | Event-driven workflow orchestration |
| Coding support | Manual code entry | NLP-assisted code suggestions |
| Inpatient logic | Coder-led DRG assignment | DRG validation and CDI prompts |
| Claim quality | Rules-based edits | Rules plus denial prediction model |
| Denial response | Reactive appeal worklists | Root cause prediction and prevention |
| Compliance | Manual audits | Coding audit trail and explainable AI |
| Payer updates | Manual rules updates | Payer rule decay management |
| Analytics | Retrospective reports | Predictive revenue cycle KPIs |
How AI Changes Daily Hospital Operations
- Task vs. Risk: Old billing software helps staff complete tasks, but AI infrastructure controls financial risk across all workflows.
- Human-in-the-Loop: The platform does not replace your billing experts. It routes easy claims automatically and sends uncertain cases to specialists.
- Better Cash Flow: Catching errors early improves your clean claim rate and raises your first-pass acceptance rate.
- Lower Overhead: Automated checks protect your revenue integrity and stop your accounts receivable aging from growing too old.
- Smart Analytics: The platform lowers your overall cost to collect while running instant denial root cause analysis on rejected files (Source: CAQH Index, 2024; Source: HFMA MAP Keys).
The distinction matters because hospital leaders often compare an AI RCM platform against the wrong category. It should not be judged only by billing automation speed. It should be judged by how much revenue risk it detects before staff must chase it manually.
Where AI RCM Automation Software Creates the Most Value
AI in hospital revenue cycle automation software creates the most value where small errors compound into delayed or reduced payment. The best candidates for this technology are front-end entry, mid-cycle coding, and back-end collections.
Instead of chasing mistakes, the platform stops leaks at the specific points where transaction volume and financial risk are highest.
1. Patient Access and Financial Clearance
The front end of the billing cycle is where most preventable denials start. Automated tools protect your margins before care is ever delivered.
- Instant Verification: The system runs real-time eligibility verification at patient access by matching registration details with live insurance data.
- Active Discovery: Automated insurance discovery tools scan secondary databases to find active coverage options that patients might omit.
- Data Validation: Integrated demographic validation systems instantly catch spelling errors or wrong policy numbers to stop simple rejections.
- Clear Clearance: The engine calculates out-of-pocket costs to establish patient financial clearance and set up automated payment plans early.
- Prior Authorization: Built-in models handle prior authorization requirement detection by checking scheduled procedures against ever-changing payer rules.
By stopping errors at intake, health systems prevent expensive front-end denials from stalling cash flow later.
2. Mid-Cycle Coding and Revenue Integrity
The middle cycle requires deep medical knowledge to translate clinical events into exact billing codes. AI acts as a digital helper for your certified coders.
- Documentation Improvement: The platform drives CDI for inpatient coding by reading charts in real-time and asking doctors for missing details.
- Inpatient Automation: Deep learning models handle complex DRG coding automation to ensure precise MS-DRG assignment and APR-DRG coding.
- Facility vs. Professional: The system simultaneously processes ICD-10-CM inpatient coding and ICD-10-PCS procedure coding while assigning correct CPT codes.
- Medical Necessity: The engine checks clinical documentation against local coverage determinations (LCD) and national coverage determinations (NCD) to ensure full LCD / NCD compliance.
- Integrity Checks: Automated audits scan for undercoding detection to find missed revenue, and overcoding detection to keep the hospital audit-safe.
This constant layer of protection ensures absolute revenue integrity without slowing down your human coding team.
3. Claims and Denials
Once documentation is complete, the platform packages the data for submission and actively checks for payer traps.
- Institutional Scrubbing: The system builds EDI 837I institutional claims and runs them through a custom hospital claims scrubbing engine.
- Edit Matching: Claims are checked against the National Correct Coding Initiative (NCCI) edits and specific, hidden payer edits before submission.
- Acceptance Focus: Fixing these issues raises your clean claim rate and hits a much higher first-pass acceptance rate.
- Predictive Defense: A trained denial prediction model flags claims that have a high probability of rejection so staff can fix them first.
- Smart Appeals: If a denial slips through, the automated appeals management workflow extracts the exact needed records and writes a targeted appeal.
4. Payments, Contracts, and AR
The final stage of the cycle ensures you actually receive every single dollar you are legally owed under your insurance contracts.
- Remittance Posting: The platform reads incoming EDI 835 remittance processing files to handle payment posting automation without human data entry.
- Contract Auditing: Digital payer contract management tools store your specific fee schedules and insurance terms directly in the cloud.
- Variance Recovery: The underpayment recovery module compares paid amounts against those contracts to flag shortfalls and open recovery files.
- Aging Management: Preventing manual delays directly lowers your overall days in AR and improves your total net collection rate.
- Efficiency Metrics: Automating these redundant clerical tasks drops your overall cost to collect while keeping cash predictable.
Hospitals should not try to automate every single workflow at one time. They should start where high transaction volume and high manual rework meet.
Focusing your AI infrastructure here creates measurable movement in your clean claim rate, shortens your cash cycle, and protects thin margins.
Hospital-Specific Logic Your AI RCM Platform Must Support
A hospital AI revenue cycle platform must support facility billing rules that do not exist in ordinary physician billing workflows. Inpatient cases require complex MS-DRG assignment, APR-DRG logic, and ICD-10-PCS procedure coding.
The system must run continuous CDI reviews and medical necessity checks, backed by audit trails that explain every coding recommendation.
1. The Hospital Coding Logic Map
Hospital operations involve two different billing streams: professional billing for provider services and facility billing for hospital resources like rooms, supplies, and operating time. The table below outlines how the AI platform supports these complex workflows and identifies when a human specialist must step in.
| Revenue Workflow | AI Support Needed | Human Review Trigger |
| Inpatient admission | DRG prediction and CDI prompts | Low documentation confidence |
| Discharge coding | MS-DRG and ICD-10-PCS validation | High-value DRG shift |
| Surgery billing | CPT, HCPCS, implant, and supply validation | Missing charge or modifier conflict |
| Outpatient procedure | Medical necessity and LCD/NCD check | Payer-specific coverage risk |
| Emergency department | E&M coding validation | Incomplete documentation |
| Risk adjustment | HCC risk adjustment review | Unsupported diagnosis capture |
1. Professional vs. Facility Billing Complexities
Professional billing covers provider services, while facility billing tracks hospital resources like rooms, supplies, and operating time.
An enterprise platform runs separate data pipelines to ensure hospital overhead is fully captured alongside professional fees.
2. Inpatient Care and DRG Logic Automation
Inpatient billing relies on grouping systems rather than individual line items. The platform uses clinical NLP to analyze charts for accurate MS-DRG assignment and APR-DRG coding.
It runs real-time CDI prompts while patients are admitted to capture missing secondary diagnoses, optimizing the case mix index.
3. Outpatient Operations and APC Mapping
Outpatient visits use APC logic, requiring validation of every individual service. The platform tracks outpatient workflows by assigning the correct CPT codes and HCPCS codes.
Machine learning checks modifier applications and catches missing details before submission to protect outpatient charge capture.
4. Resource Tracking and Charge Integrity
The platform connects to the charge description master (CDM) to audit surgeries, pharmacy, and lab resources.
It verifies that expensive implants and medications match provider orders. If data conflicts occur, the system routes the file to a human-in-the-loop review queue.
Hospital RCM AI becomes risky when it treats all billing like outpatient claims. Inpatient workflows need a deeper logic layer because one coding decision can shift reimbursement, audit exposure, and case mix index. That logic also shapes the platform architecture.
Core Architecture of a HIPAA Compliant RCM Platform
A HIPAA-compliant hospital RCM platform must use a simple, layered setup to move financial data safely. This architecture divides big tasks into smaller, isolated software parts.
By doing this, the platform can process thousands of bills at the same time without slowing down, making mistakes, or exposing private patient records.
The Seven-Layer AI RCM Architecture
To keep things organized, we split the software into seven basic building blocks. The table below breaks down exactly what each layer does and the simple tools used to run it.
| Architecture Layer | What Happens Within the Layer | Specific Technology Within the Layer |
| 1. Ingestion Layer | Grabs raw data from hospital computer systems and live insurance feeds. | HL7 ADT messages, FHIR R4 API, and basic Epic or Cerner database connectors. |
| 2. Workflow Layer | Acts as a traffic cop to route tasks and open work bills for hospital staff. | Microservices hospital billing architecture and event-driven billing workflow systems. |
| 3. AI Processing Layer | Reads plain medical notes and guesses the right billing codes or rejection risks. | Clinical NLP text readers, automated coding models, and a denial prediction model. |
| 4. Payer Rules Layer | Checks every bill against standard government rules and insurance policies. | NCCI edits checker, Local Coverage Determinations (LCD), and National Coverage Determinations (NCD). |
| 5. Security Layer | Locks down private data and hides patient names to follow the law. | HIPAA Security Rule tools, PHI tokenization, and simple role-based access control. |
| 6. Human Review Layer | Shows hard cases to real people and asks for help when the AI is confused. | Exception management screens, confidence scoring, and explainable AI recommendations. |
| 7. Monitoring Layer | Watches the AI models in the background to ensure they do not become outdated. | MLOps pipeline tools, model drift monitoring, and payer rule decay management. |
Splitting the software into seven basic layers keeps the system clean and easy to fix. In fact, if an insurance company changes its rules, you only have to update the rules layer. You do not have to rebuild or break the rest of your hospital billing software.
EHR, HIS, and Payer Integrations AI RCMs Need
Hospital RCM software development requires deep data connections before AI can create reliable output. The platform must gather clear facts from Epic, Cerner, Meditech, and internal accounting systems.
Without these connections, the AI only sees broken fragments instead of the full billing event, which causes incorrect risk predictions.
1. The Basic Hospital Connection Map
To build a complete financial picture, your software must talk to many different systems. The table below lists the essential connections your platform needs to manage hospital claims safely.
| Integration Name | Why It Is Important | What Data Moves Through It |
| Epic EHR integration | Pulls clinical records and directs provider orders. | Patient visits, diagnoses, procedures, and doctor notes. |
| Cerner integration | Supports clinical steps and active billing workflows. | Patient files, visit numbers, codes, and charge items. |
| Meditech integration | Handles hospital operations and patient accounts. | Admission data, item charges, and final discharge notes. |
| HL7 ADT Feeds | Tracks patient movement inside the hospital walls. | Live records for admissions, discharges, and transfers. |
| FHIR R4 API | Shares clean, organized clinical data across systems. | Condition resources, patient identities, and exact procedures. |
| Clearinghouse Link | Sends completed hospital bills and receives updates. | EDI 837I institutional claims and EDI 835 payments. |
| Payer Portal Tools | automates approvals and follows up on slow claims. | Approval statuses, policy rules, and appeal updates. |
| Finance Systems | Updates general ledgers and tracks corporate revenue. | Final settled cash, balance shifts, and bad debt data. |
2. Supporting Old and New Data Streams
Your new platform must handle both modern API connections and older, legacy formats. Many commercial insurance companies still use old tech networks, so your software must bridge that gap smoothly.
- HL7 v2 Feeds: These older text messages still matter for tracking daily patient movement events like admissions and transfers.
- FHIR R4 APIs: This modern standard works best for pulling structured clinical data directly from the EHR (Source: HL7 FHIR R4 specification).
- EDI 837I Formats: This specific electronic file format is critical for packing and shipping institutional claims to payers (Source: X12 837 institutional claim implementation guide).
- EDI 835 Files: The platform must read these files to handle automated payment posting and remittance processing.
- Payer Portals: Browser automation tools are necessary because many insurance networks do not have modern developer APIs.
Automating these portal steps is especially helpful for meeting the latest CMS prior authorization final rule mandates (Source: CMS prior authorization final rule).
3. The Intellivon Integration Discovery Plan
At Intellivon, we plan out your data connections long before drawing a single dashboard screen. We follow a strict operational sequence to ensure your data pipelines are solid:
- System Inventory: We list every software version running in your hospital.
- Data Availability Review: We check if the EHR blocks or allows external reads.
- Message Mapping: We align your hospital codes with standard insurance formats.
- Interface Design: We build clean API adapters for each facility.
- Security Model Setup: We lock down the pathways using modern encryption.
- Test Environment Build: We simulate fake patient stays to check data flows.
- Transaction Validation: We ensure test bills pass clearinghouse audits.
- Go-Live Monitoring: We watch the live data streams to stop initial dropouts.
A software platform cannot predict claim risk accurately if it cannot see the full patient context. Your data integration depth determines your final model accuracy, audit quality, and rollout speed. Establishing clear data contracts across your network is the best way to ensure project success.
The Revenue Cycle Data Contract Hospitals Need Before AI Development
The revenue cycle data contract is the agreement that defines which data each hospital team must provide, validate, own, and update before AI can act on billing workflows. It covers patient access, health information management (HIM), clinical documentation improvement (CDI), coding, billing, finance, compliance, IT, and payer operations.
This document ensures the AI platform works from one shared source of truth.
1. The Hospital Data Governance Map
Instead of just talking about “clean data” generally, you need a clear checklist that assigns responsibility for every piece of billing information. The table below outlines how different hospital domains feed the AI models and who is responsible when data breaks down.
| Data Domain | Department Owner | Required Data Fields | AI Platform Use Case | Error Impact If Missing |
| Patient Demographics | Patient access | Name, DOB, payer name, subscriber ID | Eligibility checks, claim creation | Front-end eligibility denial |
| Encounter Data | HIM / EHR team | Admit date, discharge date, patient status | DRG prediction, tracking DNFB | Delayed or blocked final bill |
| Clinical Documentation | Providers / CDI | Progress notes, orders, operative reports | Automated coding, CDI prompts | Undercoding or overcoding risk |
| Charge Data | Revenue integrity | CDM code, department units, modifiers | Charge capture automation | Missed revenue or wrong charges |
| Claim Data | Billing department | Finished claim lines, active edit logs | Automated claim scrubbing | Immediate claim rejection |
| Remittance Data | Finance team | ERA files, CARC, and RARC codes | Automated payment posting | Missed payer underpayments |
| Payer Rules | Payer contracting | Payer rule versions, coverage criteria | Denial prediction models | Payer rule decay and high write-offs |
2. What to Include in Your Working Data Contract
A good data contract acts like an instruction book for your engineering team. It makes sure every department knows exactly what data their software systems must share with the AI platform.
- Source and Field Rules: The contract names the department owner for every data point and provides exact field definitions. It outlines which inputs are required and how often they must be refreshed.
- Fixing and Auditing Errors: The plan specifies validation rules and names a clear error owner to handle broken data. It also assigns an audit owner to review system logs regularly.
- Security and Workflow Paths: The agreement defines model-use permissions and restricts PHI access levels by employee role. Finally, it maps out every downstream workflow affected by a data change.
Building an AI billing platform without a clear data contract is like building a house without blueprints. When you explicitly define who owns each data point, you stop bad information from entering your system. This groundwork ensures your automated billing tools produce highly accurate financial results from day one.
[To learn more about how we build AI-powered medical billing platforms, read our blog on How to Build a Smart Healthcare Billing AI Platform. ]
AI Models Needed Inside a Hospital RCM Platform
A hospital AI revenue cycle platform usually needs several individual models working together, not just one large model. Your system should combine clinical text readers, document copy systems, and risk calculators to manage bills from start to finish.
This multi-model approach creates a strong safety net that catches small typos before they become expensive losses.
1. The Hospital RCM Model Map
To run a smart billing department, you must match the right type of math tool to each specific financial job. The table below lists the essential models your system needs and the safety boundaries they must follow.
| AI Model / Method | Revenue Cycle Use Case | Required Controls and Guardrails |
| Clinical NLP | Reads long doctor notes to find hidden diseases and treatments. | Must show the original text evidence to human coders. |
| Classification Model | Calculates the chance of an insurance company rejecting a bill. | Uses custom alert levels for each major insurance company. |
| Rules Engine | Runs classic government checks like NCCI edits and LCD guidelines. | Needs a version library that updates every single month. |
| RAG Workflow | Pulls matching insurance policy text out of giant contract folders. | Only shows answers directly grounded in official documents. |
| LLM Summarization | Writes plain text summaries for appeal letters or medical briefs. | Humans must read and sign off before anything is mailed. |
| Anomaly Detection | Spots weird drops in standard pricing, overcoding, or undercoding. | Sends all weird outliers straight to a human review line. |
| Forecasting Model | Guesses your future monthly cash flow and vital billing metrics. | Constantly watches for performance drift in the background. |
| Risk Adjustment Model | Checks provider charts to support correct HCC insurance tracking. | Requires an audit trail to prove medical necessity. |
2. Strict Guidelines for Ethical AI Use
When you build machine learning tools for hospital finance, safety rules are just as important as the code itself. Your platform must follow strict ethical guidelines to keep your health system safe from fraud investigations and legal penalties.
- No Faking Data: The platform must never invent medical notes or guess missing details. If a doctor did not write down a condition, the AI cannot add it to the bill.
- No Auto-Submitting: The software must never send out high-risk claims without a human review. All complicated facility billing changes must pass through a real certified coder.
- Full Explainability: The system must show exactly why it made a suggestion. It must display a clear confidence score, the source evidence text, and the next recommended action.
A reliable AI RCM platform relies on a team of small, focused models rather than one giant brain. When you wrap these automated tools in strong ethical guardrails, you protect your hospital from compliance audits.
This combined method allows your team to automate simple administrative tasks safely while keeping full human control over your financial data.
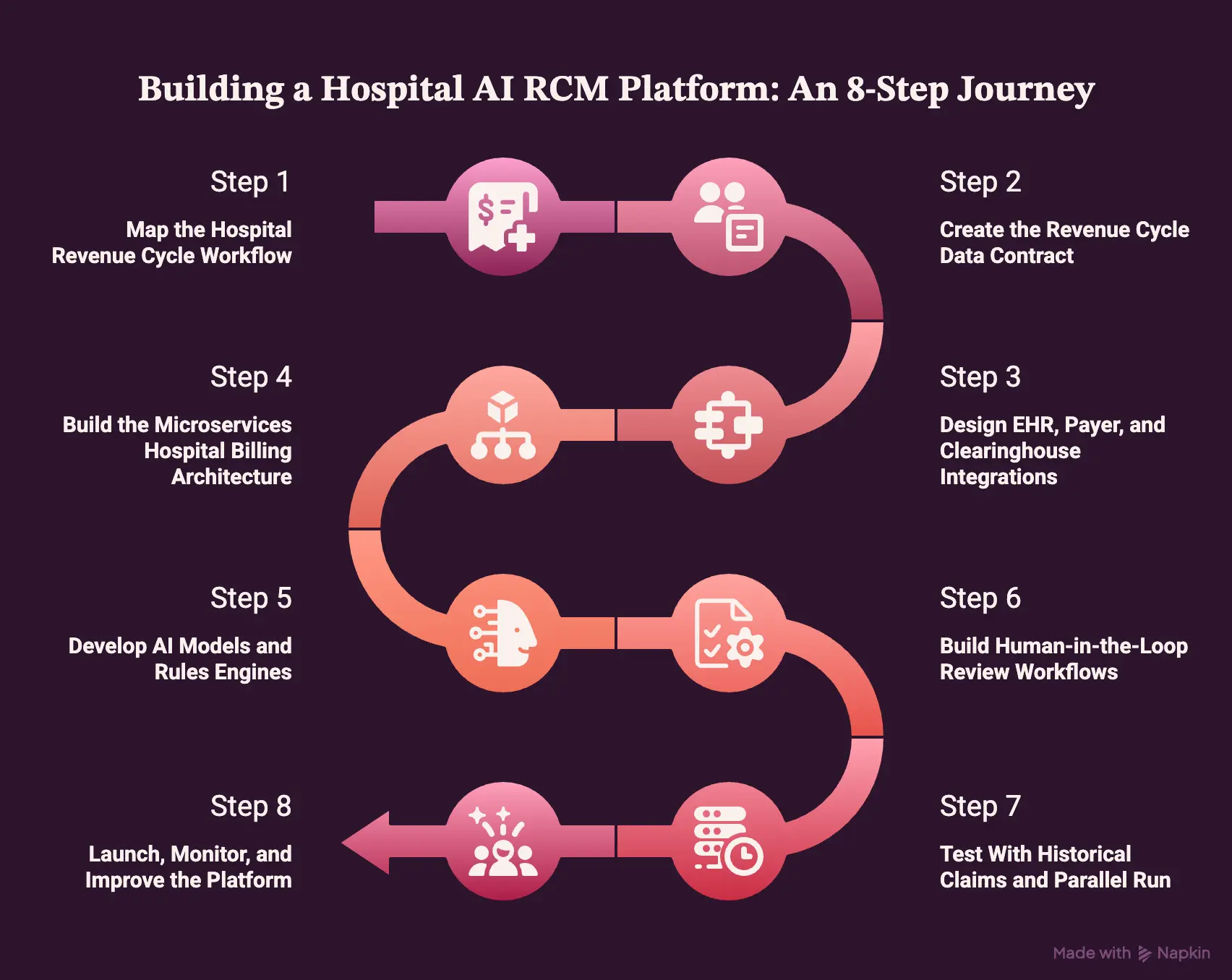
How to Build an AI RCM Platform for Hospitals
Building a hospital AI revenue cycle management platform requires executing eight sequential phases: mapping the current revenue workflow, creating a master data contract, engineering live EHR data integrations, deploying a secure microservices architecture, training clinical NLP and denial classification models, configuring human-in-the-loop review screens, validating the system with backtesting, and launching monitoring.
This precise engineering lifecycle prevents you from deploying machine learning models before your real-world financial workflows and data boundaries are fully defined.
Step 1 — Map the Hospital Revenue Cycle Workflow
The first step is to map how revenue moves from patient access to final payment across every facility.
This includes inpatient billing automation, outpatient billing automation, eligibility, prior authorization, CDI, coding, charge capture, claims, denials, appeals, payment posting, underpayment recovery, and AR follow-up.
Technical Work Required
- Conduct detailed interviews with hospital billing staff.
- Inventory all existing financial and administrative software tools.
- Map the exact lifecycle of a claim from entry to settlement.
- Analyze historical denial reasons from primary insurance payers.
- Review current Discharge Not Final Billed (DNFB) bottlenecks.
- Audit accounts receivable aging buckets across all facilities.
- Segment the hospital system’s active medical payer mix.
- Identify high-volume procedures causing repetitive manual rework.
| Assessment Area | What We Analyze | Target Metric |
| Front-End Operations | Patient registration and intake bottlenecks | Eligibility denial rate |
| Mid-Cycle Work | Clinical documentation and manual coding delays | Days in DNFB |
| Back-End Billing | Remittance errors and manual appeal writing | Total cost to collect |
The Intellivon Approach
We document your current workflows, failure points, manual queues, data handoffs, and measurable revenue cycle KPIs before defining the MVP. This groundwork ensures we build solutions for your real operational friction points.
Operational Insight: Mapping workflows prevents engineering teams from automating broken manual habits. Once the workflow is entirely clear, the next step is to define the specific data that the AI can safely use.
H3: Step 2 — Create the Revenue Cycle Data Contract
The second step is to define which data the platform can trust, where it comes from, and who owns it. This includes EHR data, HL7 ADT messages, FHIR R4 resources, charge data, payer rules, coding data, claim history, EDI 837I files, and EDI 835 remittance files.
Technical Work Required
- Build a comprehensive master data dictionary for the project.
- Assign field-level ownership to specific department databases.
- Establish validation logic rules for incoming data streams.
- Configure strict PHI handling and security tokenization rules.
- Define model-use permissions for clinical text records.
- Set up data retention and storage policies for claims.
- Gather audit evidence requirements for compliance teams.
| Data Type | Primary Source System | Update Frequency |
| ADT Records | Hospital Information System (HIS) | Real-time events |
| Clinical Notes | Electronic Health Record (EHR) | Continuous sync |
| Remittance Data | Payer Portals / Clearinghouse | Daily batch |
The Intellivon Approach
We convert these data definitions into a working build artifact signed by your engineering, compliance, and revenue cycle teams. This strict data contract keeps our development pathway clear of data quality surprises.
Operational Insight: A clear contract stops incomplete data from polluting your machine learning pipelines. Once the data contract is ready, integration design can begin with fewer technical unknowns.
H3: Step 3 — Design EHR, Payer, and Clearinghouse Integrations
The third step is to design integrations that connect clinical, financial, and payer data into one platform. Hospital RCM software development usually requires Epic EHR integration, Cerner integration, Meditech integration, hospital information system integration, patient accounting system integration, clearinghouse connectivity, payer portal automation, and finance system connections.
Technical Work Required
- Configure live HL7 interfaces for patient movement tracking.
- Set up secure FHIR R4 APIs for clinical documentation extraction.
- Build data parsers for EDI 837I institutional claims.
- Develop processing engines for incoming EDI 835 remittances.
- Deploy secure API gateways with strict corporate encryption.
- Connect internal interface engines to manage data routing.
- Create automated error queues for dropped network packets.
- Establish transaction reconciliation rules for daily verification.
| Target Interface | Integration Standard | Core Purpose |
| Core EHR | FHIR R4 API / HL7 v2 | Read clinical notes and provider orders |
| Clearinghouse | X12 EDI 837I and 835 | Submit claims and receive payment files |
| Insurance Portals | Browser automation / API | Check authorizations and claim statuses |
The Intellivon Approach
We build all your integration logic inside reusable microservices. This modular strategy ensures the underlying platform can easily support a multi-facility deployment across different regional hospitals.
Operational Insight: Deep connectivity turns static billing records into actionable data streams. After the integration design is finished, the platform needs a modular architecture that can process events safely.
H3: Step 4 — Build the Microservices Hospital Billing Architecture
The fourth step is to build a modular architecture that separates patient access, coding, claims, denials, payments, compliance, and analytics into controlled services.
A microservices hospital billing architecture helps hospitals scale workflows across departments, update modules independently, and monitor each revenue event from intake to reimbursement.
Technical Work Required
- Deploy an enterprise event bus to handle communication.
- Build an event-driven billing workflow orchestration engine.
- Create isolated microservices for claim preparation tasks.
- Develop a dedicated service for automated coding validation.
- Construct a microservice to manage denial prediction scores.
- Build a payment posting microservice for automated ledger balance.
- Deploy a centralized rules service for compliance tracking.
- Set up secure role-based access control services.
| Microservice Name | Input Trigger | Primary Output |
| Ingestion Service | New EHR event or HL7 message | Tokenized JSON data payload |
| Scrubbing Service | Completed coding file | Clean EDI 837I claim file |
| Denial Service | Incoming EDI 835 rejection | Automated appeal brief draft |
The Intellivon Approach
We design each individual microservice around actual hospital department boundaries, not just engineering convenience. This matches our technical architecture directly with your real-world team operations.
Operational Insight: Isolated software services prevent a single system failure from crashing your entire billing operation. Once the architecture is stable, AI models can be added to the correct decision points.
H3: Step 5 — Develop AI Models and Rules Engines
The fifth step is to build the AI and rules layer that supports revenue decisions. This includes clinical NLP, denial prediction, CDI prompts, code validation, charge capture automation, medical necessity validation, undercoding detection, overcoding detection, payer contract checks, and explainable AI recommendations for human reviewers.
Technical Work Required
- Prepare and clean historical claims data for model training.
- Establish a robust medical chart labeling strategy for NLP.
- Execute feature engineering for denial prediction metrics.
- Segment training models by specific commercial insurance payers.
- Calculate statistical confidence scoring for automated outputs.
- Deploy a RAG system for instant insurance policy retrieval.
- Build a version-controlled library for national coding rules.
- Run model evaluation audits against standard gold test sets.
| Model Type | Core Algorithm / Framework | Training Data Source |
| Clinical NLP | Transformer-based text extraction | Historical physician charts and reports |
| Denial Prediction | Gradient-boosted classification models | Historic EDI 837I and EDI 835 logs |
| Policy Retrieval | Vector database with RAG workflow | Payer contracts and LCD/NCD files |
The Intellivon Approach
We avoid generic, one-model-fits-all designs. Our platforms intelligently combine hardcoded rules, standard machine learning, and advanced NLP based on the specific financial risk of the task.
Operational Insight: Focused algorithms perform much better than single, massive language models. After models are built, review workflows decide how much autonomy the platform can safely support.
H3: Step 6 — Build Human-in-the-Loop Review Workflows
The sixth step is to define when AI acts, when it recommends, and when a human must review the case. Human-in-the-loop coding review is essential for complex inpatient claims, low-confidence DRG changes, high-value denials, audit-sensitive documentation, medical necessity risk, and payer-specific exceptions.
Technical Work Required
- Create customized reviewer queues for different billing teams.
- Establish automated escalation rules for high-value claims.
- Set hard confidence thresholds for hands-free automation.
- Build tracking logs to record when humans override AI choices.
- Configure mandatory audit note entry fields for compliance.
- Design coder feedback loops to improve model training data.
- Build dedicated interfaces for formal compliance sign-off.
- Program case prioritization rules based on account age.
| Confidence Score | System Action | Destination Queue |
| High (Greater than 90%) | Auto-approve and submit claim | Clearinghouse outbound track |
| Medium (60% – 90%) | Flag anomalies and show suggestions | Staff review dashboard |
| Low (Less than 60%) | Block claim and request a full edit | Specialist exception queue |
The Intellivon Approach
We design your review screens around real coders, CDI, and billing workflows. We focus on showing clear evidence trails rather than providing simple, unhelpful approve or reject buttons.
Operational Insight: Smart interfaces turn your billing staff into efficient editors rather than data entry clerks. Once review logic exists, testing must prove the platform improves revenue outcomes without increasing compliance risk.
H3: Step 7 — Test With Historical Claims and Parallel Run
The seventh step is to test the platform against historical claims before production rollout. Hospitals should compare AI recommendations against actual claim outcomes, denials, payments, appeals, coding audits, underpayments, and AR resolution. This creates a measurable baseline for clean claim rate, first-pass acceptance rate, days in AR, and DNFB.
Technical Work Required
- Run massive backtesting files through the completed models.
- Deploy the software in shadow mode using live data streams.
- Initiate a parallel run alongside your old billing software.
- Compare AI risk predictions against real insurance outcomes.
- Review false positive flags to tune system sensitivity.
- Analyze false negative misses to fix hidden gaps.
- Calculate the projected denial lift using historical files.
- Calibrate confidence scores across different facility locations.
| Testing Phase | Data Volume | Primary Objective |
| 1. Backtesting | 12-24 months of historic claims | Baseline model accuracy check |
| 2. Shadow Mode | Live production data streams | System speed and pipe testing |
| 3. Parallel Run | Active multi-facility caseload | Direct performance comparison |
The Intellivon Approach
We run a highly controlled, phased validation process. Also, we check your system using a specific workflow, payer, facility, and claim type before allowing any code to scale across your network.
Operational Insight: Parallel testing uncovers hidden bugs before they can disrupt your active cash flow. After this validation wraps up, the health system can move safely from pilot to production deployment.
H3: Step 8 — Launch, Monitor, and Improve the Platform
The final step is to launch the platform in phases and monitor both AI performance and revenue cycle outcomes.
A production platform needs an MLOps pipeline, model drift monitoring, payer rule decay management, audit log review, denial trend feedback, integration uptime monitoring, and KPI dashboards for revenue leaders.
Technical Work Required
- Deploy a continuous MLOps pipeline for regular upkeep.
- Configure drift alerts to watch for model performance drops.
- Set up regular updates for your payer rule decay management.
- Establish automated log reviews for all system actions.
- Feed new denial trends back into the engineering loops.
- Track integration uptime across all active EHR connection nodes.
- Build clean KPI dashboards for health system executives.
- Create a continuous training loop using human override data.
| Monitoring Monitor | What It Tracks | Alert Trigger |
| Model Drift Engine | Drop in coding prediction accuracy | Accuracy falls below 85% |
| Payer Rule Monitor | Changes in commercial insurance rules | Spike in novel denial codes |
| API Pipeline Monitor | Network latency across FHIR/HL7 routes | Response time greater than 2 seconds |
The Intellivon Approach
We include long-term MLOps and compliance monitoring as a core part of our initial platform design. At the same time, we never treat system maintenance like an afterthought or a secondary phase.
Building a hospital AI system is an ongoing operational commitment, not a simple one-time install. With the build path clear, healthcare leaders need a realistic budget before choosing the right development scope.
AI RCM Platform Development Cost
AI RCM platform development usually costs $70,000–$200,000, depending on workflow scope, EHR connectivity, claims automation depth, AI model complexity, HIPAA controls, and deployment requirements.
A focused MVP may cover claims scrubbing, denial prediction, coding support, and basic dashboarding, while a higher-end build includes deeper integrations and compliance workflows.
| Development phase | Estimated cost | What it covers |
| Discovery and revenue workflow mapping | $5,000–$12,000 | Workflow interviews, denial analysis, payer mix, DNFB review, MVP scope |
| Data contract and integration planning | $6,000–$15,000 | Data dictionary, system inventory, EHR mapping, EDI/FHIR planning |
| UX/UI for hospital revenue teams | $8,000–$18,000 | Worklists, dashboards, reviewer queues, coder screens, and admin tools |
| Backend and workflow orchestration | $15,000–$35,000 | Workflow engine, task routing, event handling, and role-based access |
| EHR, clearinghouse, and payer integrations | $18,000–$45,000 | EHR data flow, HL7/FHIR setup, EDI 837I, EDI 835, payer connectivity |
| AI model development | $20,000–$50,000 | NLP, denial prediction, coding support, RAG, anomaly detection |
| Rules engine and payer policy layer | $10,000–$25,000 | NCCI edits, LCD/NCD checks, medical necessity, payer rule versioning |
| HIPAA security and compliance controls | $8,000–$22,000 | PHI controls, encryption, RBAC, audit logs, BAA-ready documentation |
| Testing, backtesting, and parallel run | $8,000–$20,000 | Historical claims testing, model validation, integration QA |
| Deployment and rollout support | $7,000–$18,000 | Production release, training, monitoring dashboards, support setup |
Maintenance Cost
Annual maintenance usually runs 18%–30% of the initial build cost. For a $70,000–$200,000 platform, that usually means $12,600–$60,000 per year, depending on how often the platform needs payer-rule updates, model monitoring, compliance reviews, and integration support.
Maintenance typically covers:
- EHR and clearinghouse changes
- Payer rule updates
- Coding updates
- Model drift monitoring
- Security patching
- Compliance reviews
- Cloud infrastructure
- Support and QA
Need a Hospital AI RCM Cost Model Before Development?
Contact Intellivon to estimate your MVP scope, integration budget, AI model requirements, compliance controls, and rollout timeline before development begins.
The safest budget is tied to workflow scope, not feature count. A hospital should price the build around claims volume, payer complexity, integration depth, inpatient coding requirements, and compliance risk. This also helps leaders decide whether to build a focused AI RCM MVP first or expand into a larger hospital revenue cycle platform later.
Build vs Buy Framework for AI RCMs
Hospitals should buy when they need standard workflows fast and build when revenue operations require deep customization, data ownership, multi-facility control, complex inpatient coding, proprietary payer logic, or product differentiation. A custom AI RCM system for hospitals makes sense when off-the-shelf tools cannot match workflow, governance, or integration needs.
The Build vs. Buy Decision Checklist
Choosing between buying a packaged system or building a custom platform depends on your exact operational requirements. The table below outlines how each option matches specific health system goals.
| Decision Factor | Buying Pre-Made Software | Building a Custom Platform |
| Standard outpatient billing workflows | Better fit | Usually excessive |
| Complex inpatient revenue cycle AI platform | Limited fit | Strong fit |
| Multi-facility governance | Often constrained | Strong fit |
| Proprietary payer logic | Limited control | Strong control |
| Data ownership | Vendor-controlled | Hospital-controlled |
| AI model customization | Limited | Full |
| Speed to launch | Faster | Slower |
| Long-term differentiation | Lower | Higher |
The right choice depends entirely on how much operational control your organization needs. If your hospital only wants faster execution for basic tasks, buying a vendor tool can work. However, if you need a governed, smart revenue infrastructure that scales across multiple facilities, a custom build becomes much easier to justify.
Build a Hospital AI Revenue Cycle Platform With Intellivon
Intellivon builds hospital AI revenue cycle platforms around real billing workflows, secure healthcare integrations, payer-aware rules, explainable AI, HIPAA controls, MLOps, and measurable revenue outcomes. The work starts with workflow scope, data access, architecture, compliance design, integration planning, model strategy, and phased rollout planning.
1. Define the Right AI RCM Scope
Intellivon helps hospitals define the right development scope before engineering begins. This keeps the platform focused on revenue problems that matter, instead of building scattered AI features without operational value.
- Plan the MVP around high-impact revenue cycle workflows.
- Prioritize coding, claims, denials, and payment automation.
- Separate inpatient and outpatient billing requirements clearly.
- Assess build-versus-buy tradeoffs before platform investment.
- Estimate ROI based on claims volume and denial reduction.
- Plan multi-facility rollout without disrupting revenue teams.
2. Design the Platform Architecture Around Hospital Ops
Hospital RCM platforms need architecture that reflects how revenue teams actually work. Intellivon designs the system around hospital workflows, integration needs, compliance controls, and long-term operational visibility.
- Build microservices for billing, coding, claims, and denials.
- Use event-driven workflows for real-time task routing.
- Integrate with EHR, HIS, and patient accounting systems.
- Connect clearinghouses for claims and remittance workflows.
- Automate payer portal actions where APIs are limited.
- Maintain audit-ready logs across every revenue workflow.
3. Build AI Models Revenue Teams Can Trust
AI only works in RCM when teams can understand and verify its recommendations. Intellivon builds AI models with explainability, confidence scoring, and human review so revenue teams stay in control.
- Use clinical NLP to extract coding and documentation signals.
- Build denial prediction models around payer-specific patterns.
- Support coding teams with evidence-linked recommendations.
- Add CDI prompts for documentation improvement workflows.
- Show confidence scores for every AI recommendation.
- Route complex cases to human reviewers before action.
4. Make the Platform Secure and Monitorable
Hospital billing AI must protect PHI, support compliance, and stay reliable after launch. Intellivon designs security, monitoring, and governance into the platform from day one.
- Design HIPAA-ready architecture for sensitive revenue data.
- Use PHI tokenization to reduce exposure risk.
- Apply role-based access control across user groups.
- Maintain audit logs for coding, claims, and appeals.
- Use zero-trust controls for secure platform access.
- Prepare BAA-ready documentation for vendor governance.
- Set up MLOps pipelines for production model monitoring.
- Track model drift as payer and coding rules change.
If you are planning to build a hospital AI revenue cycle platform around coding, claims, denials, payment posting, underpayment recovery, or multi-facility RCM operations, Intellivon can help you define the roadmap before development begins.
Conclusion
A hospital AI revenue cycle management platform should be planned as revenue infrastructure, not a billing add-on. The strongest builds connect patient access, CDI, coding, claims, denials, payment posting, payer contracts, analytics, and compliance into one governed operating layer.
For hospitals and health systems, the real decision is not whether AI can automate tasks. It is whether the platform can improve revenue outcomes while keeping every recommendation explainable, auditable, and safe for production. Intellivon can help teams define that roadmap before development begins.
Things To Know About AI Revenue Cycle Management Platforms
Q1. How much does a hospital AI revenue cycle platform cost?
A1. A hospital AI revenue cycle platform usually costs $180,000 to $1,200,000 to build. A focused MVP with claims scrubbing and one EHR integration sits near $180,000 to $350,000. Multi-facility platforms with complex inpatient coding, automated payer portals, and full MLOps pipelines can easily exceed $750,000.
Q2. Can a HIPAA-compliant hospital RCM platform use LLMs safely?
A2. Yes, you can use LLMs safely by implementing strict PHI tokenization and localized training pipelines inside a zero-trust architecture. The models must be limited to reading charts, drafting appeals, and retrieving rules. They must never make standalone financial decisions without a human-in-the-loop review.
Q3. What integrations matter most for hospital RCM software development?
A3. The most important connections are Epic, Cerner, and Meditech EHR platforms alongside your patient accounting system. On the delivery side, the system requires clearinghouse connectivity and automated payer portal scripts. It must process real-time HL7 ADT messages, FHIR R4 APIs, EDI 837I claims, and EDI 835 remittance files.
Q4. What makes an inpatient revenue cycle AI platform different from outpatient billing automation?
A4. Inpatient platforms manage facility billing, which relies heavily on complex MS-DRG assignment, APR-DRG coding, and ICD-10-PCS procedure mapping. Outpatient billing automation focuses instead on professional fees, tracking individual CPT codes, HCPCS codes, modifier applications, and immediate charge capture automation rules across your ambulatory clinics.
Q5. Should hospitals build or buy a custom AI RCM system for hospitals?
A5. Buy if you have standard outpatient workflows and need simple tasks automated quickly. Build a custom system if your health network requires proprietary payer logic, complete data ownership, multi-facility governance, or advanced inpatient coding. Many networks use a hybrid approach to get the best of both worlds.



