

Key Takeaways:
-
Value-based care platforms unify EHR, claims, pharmacy, lab, SDOH, RPM, and payer data into one layer.
-
Patient attribution, predictive risk scoring, care gap automation, and quality measure reporting are core features.
-
HCC coding support, contract analytics, total cost of care dashboards, and AI model governance ensure financial accuracy.
-
Custom enterprise platforms cost $180,000 to $650,000 depending on data sources and AI model depth.
-
How Intellivon builds value-based care platforms around measurable shared savings, ACO readiness, capitation risk, and compliance.
Value-based care platform features fall into six core categories, which include risk stratification, quality measure automation, care management workflows, multi-source data integration, financial risk modeling, and regulatory reporting. When an organization signs its first ACO REACH or capitation contract, the platform built for fee-for-service visit counts cannot do any of this. So the technology gap shows up fast, usually within the first reporting cycle.
Here is what other feature guides skip. If HCC and risk adjustment coding accuracy is not built into the platform from day one, every financial risk model running on top of it produces numbers that are simply wrong. As a result, ACOs with coding accuracy gaps under-report patient risk scores by 10 to 20%, which directly reduces shared savings payouts under MSSP. Fix the coding layer first, though, and every downstream model becomes reliable within a single contract year.
Intellivon builds risk adjustment accuracy and risk modeling together, as one system, not as separate add-ons. This post covers every feature category required for a value-based care transition, from risk stratification and HEDIS automation to care management workflows and CMS reporting. By the end, you will have a framework to scope your build or evaluate any vendor against.
What Is A Value-Based Care Platform And Why Do Enterprises Need It?
A value-based care platform is an enterprise healthcare system that helps providers and payers manage patient risk, care gaps, utilization, quality scores, contract performance, and total cost of care. Enterprises need it because value-based payment makes them financially accountable for outcomes, while legacy EHR and claims systems only record events after they happen.
This specialized environment serves as an operational layer above transaction-focused database architectures to mitigate financial risk.
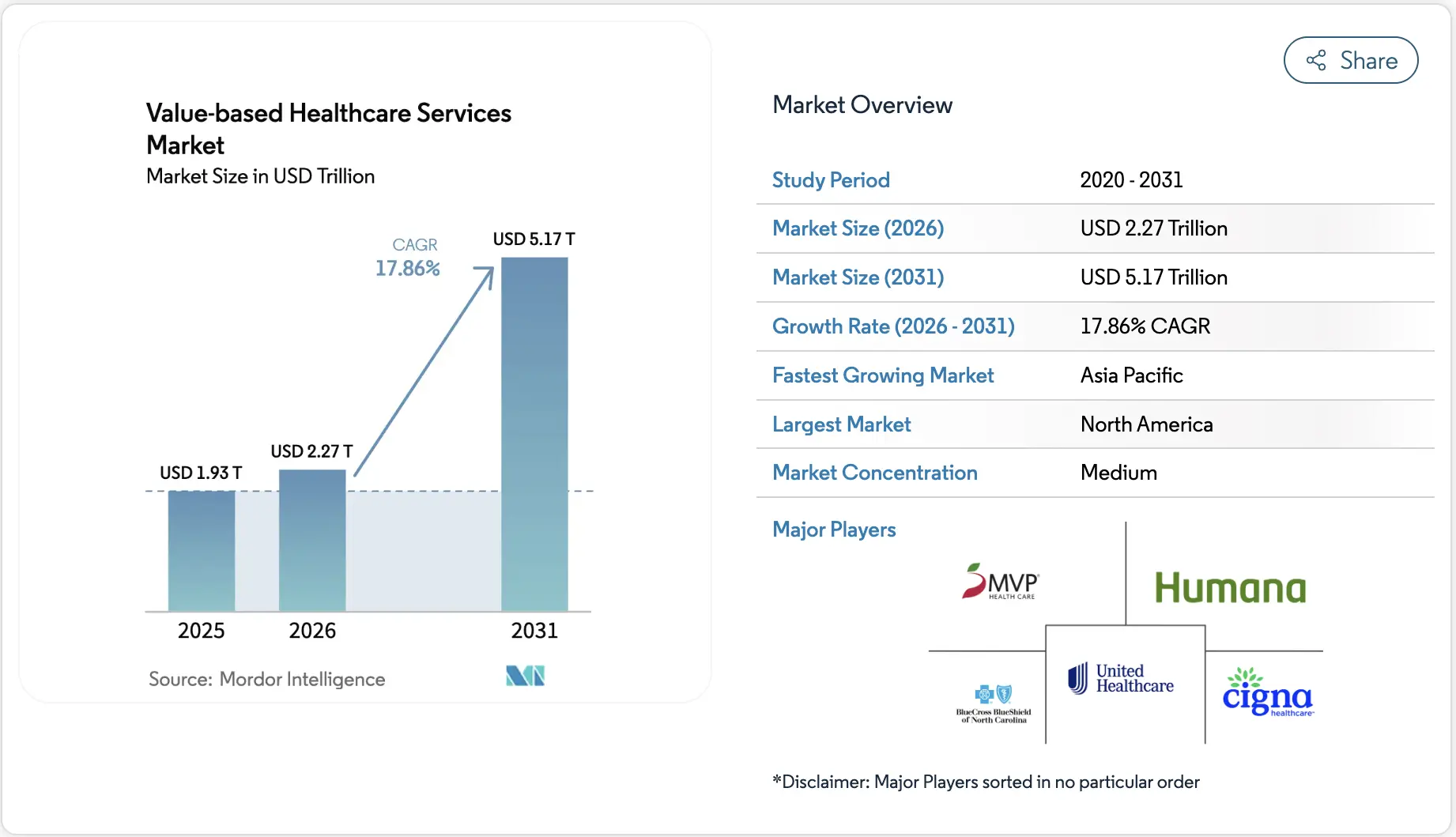
Driven by the transition away from volume, the global value-based healthcare services market is projected to reach $2.27 trillion in 2026 and surge to $5.17 trillion by 2031, growing at an impressive 17.86% CAGR (Mordor Intelligence).
Core Components of Value-Based Technology
To fully replace fee-for-service systems, a modern platform requires an architecture built around clinical risk ingestion, automated quality tracking, and deep interoperability.
1. Risk Stratification and Patient Segmentation
This component relies on automated predictive modeling to continuously ingest multi-source data and categorize population risks before high-cost events occur.
- Algorithmic Scoring: Uses predictive risk scoring models to evaluate longitudinal clinical histories alongside chronic disease risk model features.
- Rising Risk Identification: Automatically flags individuals trending toward severe clinical deterioration or frequent emergency utilization.
2. Quality Measure and Compliance Automation
Platforms must automate data collection and parsing across complex federal, state, and private quality frameworks to prevent massive administrative penalties.
- Continuous Evaluation: Tracks clinical data integration features continuously to automate HEDIS measure automation features and STARS rating measure features.
- Reporting Optimization: Feeds normalized structured pipelines directly into complex CMS quality program features and ACO quality reporting features.
3. Interoperability and Ingestion Engines
A value-based care platform requires a single, unified source of truth that normalizes highly fragmented data pipelines across the care continuum.
- Multi-Source Data Aggregation: Unifies claims and clinical data integration features with live EHR data integration VBC features.
- Holistic Patient Profiles: Integrates diverse data pipelines including social determinants screening features, pharmacy data integration features, and remote patient monitoring integration features.
4. Contract Analytics and Financial Risk Modeling
Sustaining profitability under downside risk requires precise, real-time monitoring of total cost of care analytics features against actuarial contract benchmarks.
- Financial Tracking: Models shared savings program features and capitation model technology features to track spending variation across precise patient panels.
- Leakage and Network Management: Evaluates network leakage analysis and in-network referral steering to identify wide provider and specialist cost variations.
The enterprise issue is not a lack of data, but the lack of an orchestration layer that turns disconnected records into contract-safe action. At the same time, transitioning to risk-based contracts without this technology leaves organizations exposed to unchecked margin erosion.
How Value-Based Care Platform Features Create Enterprise ROI
Value-based care platform features create ROI by reducing avoidable utilization, improving quality measure performance, protecting shared savings, increasing care manager productivity, and giving leaders better control over downside risk.
At the same time, the financial return comes from fewer readmissions, lower emergency department use, stronger HEDIS and STARS performance, better HCC capture, and more accurate contract forecasting.
When deployed efficiently, they systematically convert massive clinical operational waste directly into captured corporate revenue.
1. Avoided Utilization and Hospital Readmission Reductions
This vector uses automated clinical tracking to catch patient deterioration early and prevent catastrophic, non-reimbursable acute care expenditures.
- Preventative Alerts: Deploys automated care gap identification features and post-discharge follow-up automation to systematically reduce ED utilization.
- Proven Impact: Advanced implementations, such as Oak Street Health’s model, achieved a 51% reduction in hospital admissions and a 42% reduction in 30-day readmissions.
- Intellivon’s Production Approach: We build real-time event monitoring pipelines that link directly to regional health information exchanges (HIEs) to instantly flag emergency admissions for immediate transitional care management.
2. Quality Performance and Performance Bonus Capture
Maximizing alternative payment revenue requires continuous tracking of open care gaps to avoid millions in federal and commercial reporting penalties.
- Gap Closure Automation: Runs continuous HEDIS measure automation features alongside STARS rating measure features to scale performance scores.
- Market Scale Proof: In the CMS Medicare Shared Savings Program, 75% of participating ACOs earned performance payments totaling $4.1 billion, driven heavily by lower utilization and digital quality measure compliance.
- Intellivon’s Production Approach: We build automated clinical quality engines that match open care gaps with patient outreach automation to orchestrate high-velocity preventative scheduling.
3. Risk Adjustment Accuracy and HCC Coding Capture
Accurately capturing the true clinical complexity of your population directly elevates your baseline contract spending benchmarks, protecting your margins against artificial deficits.
- Coding Completeness: Uses hierarchical condition category capture and risk adjustment coding features to accurately capture multi-source data insights.
- Benchmark Calibration: Converts loose clinical notes into highly accurate HCC coding accuracy features via advanced clinical documentation improvement VBC features.
- Intellivon’s Production Approach: We engineer secure MLOps pipeline features VBC to parse unstructured EHR logs, surfacing historical coding gap closure features right at the point of care.
4. Care Team Efficiency and Workflow Optimization
Scaling population health programs without exponentially increasing expensive nursing headcount requires eliminating the manual overhead associated with tracking panels.
- Workflow Coordination: Implements centralized care plan automation features to streamline dense nurse navigator workflows.
- Ecosystem Triage: Coordinates clinical activities across complex environments using Risant Health’s tech-enabled value-based care platform model to drive intelligent triage and ambient documentation.
- Intellivon’s Production Approach: We build rule-driven care coordination platform features that dynamically balance care manager workload assignments based on live predictive risk scoring data.
ROI in value-based care does not come from one standalone feature. It comes from connecting risk prediction, clinical action, quality evidence, and contract economics into a continuous operational loop designed around custom infrastructure.
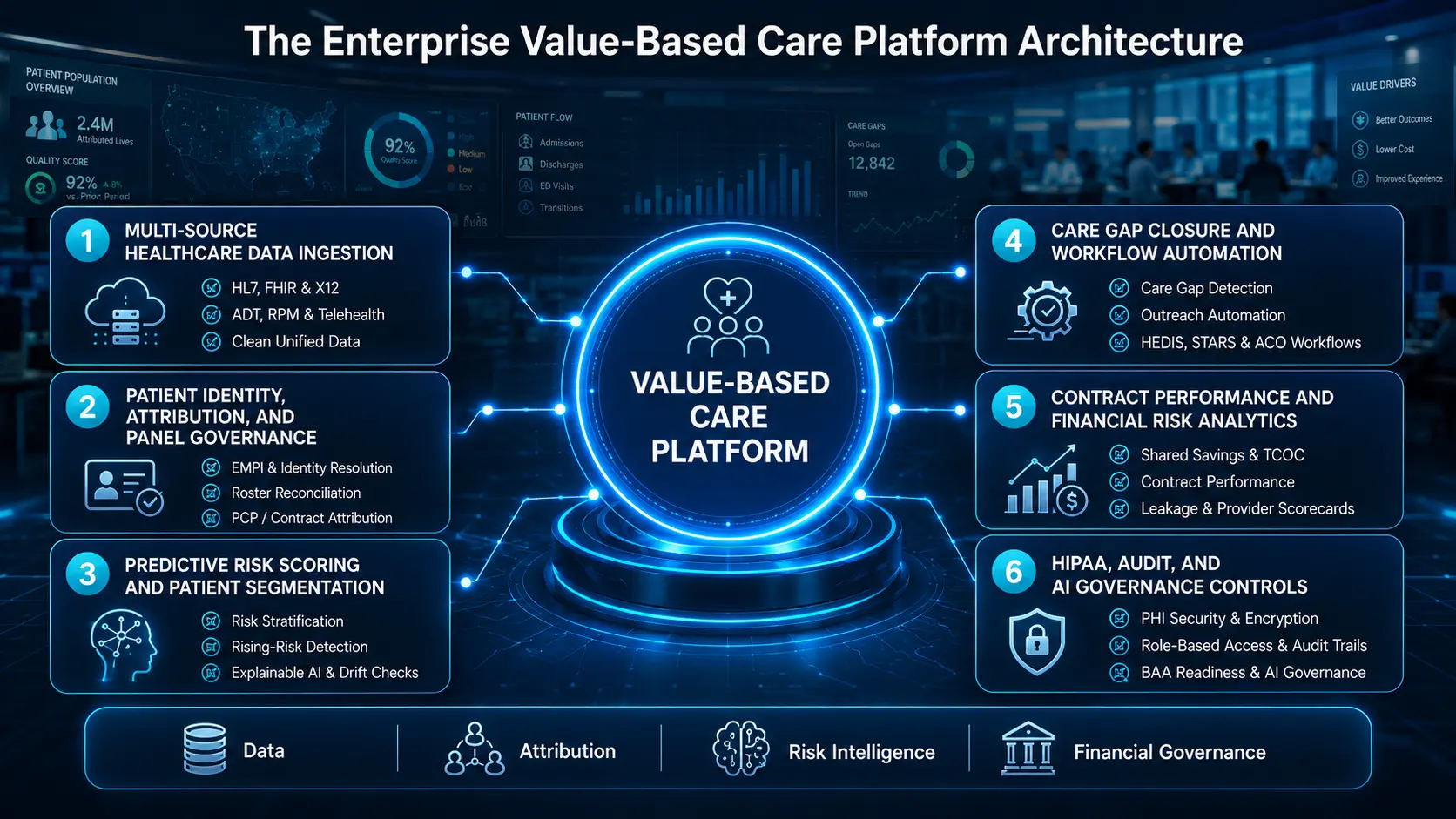
The Enterprise Value-Based Care Platform Architecture
Enterprise value-based care platform architecture needs six connected layers: data ingestion, patient identity resolution, risk intelligence, care workflow automation, contract performance analytics, and compliance governance.
Each layer must support clinical decisions, financial reporting, payer evidence, and audit readiness without forcing teams to work across disconnected dashboards.
By anchoring each layer to real-time microservices, this architectural approach guarantees that compliance-ready automated loops protect risk-bearing organizations against margin erosion.
Layer 1 — Multi-Source Healthcare Data Ingestion
The data ingestion layer pulls clinical, claims, pharmacy, lab, ADT, SDOH, RPM, telehealth, and payer contract data into one controlled environment.
This layer is the foundation for patient risk segmentation, care gap identification, chronic disease risk model features, utilization management, and value-based contract analytics across multiple payer relationships.
- Data Pipelines: Ingests HL7 v2 event streams, FHIR R4 APIs, and X12 claims files (837/835).
- Real-Time Alerts: Establishes native triggers for Admission, Discharge, and Transfer (ADT) logs.
- Diverse Channels: Coordinates streams from remote patient monitoring integration and telehealth integration VBC features.
- Data Validation: Normalizes unstructured and structured multi-payer data into a unified, clean database table.
Layer 2 — Patient Identity, Attribution, And Panel Governance
Patient identity and attribution features decide which patients belong to which provider, contract, risk pool, and care team.
Without attribution model features and patient attribution tracking, enterprises cannot calculate shared savings, assign care work, measure provider performance, or defend quality reporting during payer and CMS reconciliation.
- Identity Resolution: Deploys an enterprise master patient index using deterministic matching logic.
- Roster Reconciliation: Maps payer rosters against dynamic contract attribution rules.
- Panel Assignment: Automates primary care provider (PCP) and specialist panel relationship mapping.
- Auditing Track: Preserves historical attribution changes to prevent disputes during financial settlement.
Layer 3 — Predictive Risk Scoring And Patient Segmentation
Predictive risk scoring features identify high-risk, rising-risk, and complex-care patients before expensive events happen.
These models combine clinical history, claims patterns, medication use, social determinants, prior admissions, chronic disease indicators, and utilization trends to prioritize intervention before readmissions, ED visits, or avoidable complications damage outcomes and contract performance.
- Risk Modeling: Computes risk stratification model features and chronic disease risk model features.
- Proactive Triage: Drives rising risk identification features before acute, costly admissions occur.
- Model Integrity: Runs continuous model drift monitoring VBC features and strict population bias checks.
- Explainable Analytics: Uses explainable AI risk scoring features to surface exact clinical logic to care teams.
Layer 4 — Care Gap Closure And Workflow Automation
Care gap identification features convert quality, clinical, and payer requirements into patient-level action lists.
The platform should detect overdue screenings, missing labs, uncontrolled chronic conditions, medication gaps, annual wellness visits, post-discharge follow-ups, and preventive care reminders, then route each task to the right care manager, nurse navigator, or provider.
- Metric Automation: Powers HEDIS measure automation features and STARS rating measure features.
- Regulatory Frameworks: Supports compliance reporting for CMS quality program features and ACO quality reporting features.
- Outreach Automation: Connects open care gap closure outreach features to multi-channel patient outreach automation.
- Staff Coordination: Optimizes nurse navigator workflow features and community health worker integration features.
Layer 5 — Contract Performance And Financial Risk Analytics
Value-based contract management platform features help enterprises understand whether each payer contract is profitable, underperforming, or exposing the organization to avoidable downside risk.
The platform should calculate benchmarks, shared savings, total cost of care, episode costs, utilization trends, leakage, provider variation, and contract-specific quality thresholds.
- Actuarial Engines: Drives financial risk modeling features and accurate shared savings calculation features.
- Baseline Calibration: Evaluates performance against historical benchmark comparison features and payer contract performance features.
- Model Variety: Integrates bundled payment management features, episode of care tracking features, and capitation model technology features.
- Leakage Control: Runs network leakage analysis features to power in-network referral steering and provider scorecards.
Layer 6 — HIPAA, Audit, And AI Governance Controls
HIPAA-compliant value-based care platform features protect PHI, control user access, document model behavior, and preserve audit evidence across clinical, financial, and operational workflows.
Core requirements include data encryption, role-based access, audit trails, BAA readiness, data retention policies, model monitoring, and explainable AI controls for risk scoring.
- Data Defense: Enforces strict PHI security VBC platform protocols and comprehensive data encryption VBC platform rules.
- Access Management: Provisions granular role-based access VBC platform profiles to protect patient privacy.
- Audit Preparation: Generates immutable audit trail VBC platform logs and outputs automated compliance evidence exports.
- Vendor Compliance: Fulfills core BAA requirements VBC vendors must sustain under federal privacy frameworks.
The enterprise architecture succeeds when data ingestion, patient attribution, risk intelligence, and financial contract mapping function as a unified loop.
Therefore, removing silos across these technical layers protects risk-bearing organizations from unmonitored baseline margin erosion.
Enterprise Value-Based Care Platform Features Checklist
An enterprise value-based care platform feature checklist should cover data integration, attribution, risk scoring, care gap automation, care management, patient engagement, quality reporting, contract analytics, network performance, compliance, and AI governance.
CTOs should evaluate each feature by whether it improves contract performance, clinical action, regulatory reporting, or measurable cost control.
By auditing software capabilities against these specific architectural domains, engineering teams can guarantee that their custom environment functions as a reliable, margin-protective infrastructure.
1. Data And Interoperability Features
The data layer must continuously ingest and normalize unstructured clinical events and structured claims records across the care continuum.
- Core Data Integration: Connects claims and clinical data integration features alongside EHR data integration VBC features.
- Payer and Pharmacy Feeds: Integrates claims data integration VBC features with live pharmacy data integration features and payer roster ingestion.
- Holistic Stream Mapping: Embeds SDOH data integration features, behavioral health integration features, RPM integration, and telehealth integration.
- Standards and Diagnostics: Utilizes FHIR APIs, HL7 v2, and X12 EDI protocols to drive an internal data quality dashboard.
2. Risk Stratification And AI Features
Advanced analytical modules must process normalized patient graphs to accurately calculate risk profiles before costly acute utilization events occur.
- Algorithmic Stratification: Deploys specialized AI features for value-based care models, predictive risk scoring, and rising-risk patient identification.
- Disease and Cost Forecasting: Executes chronic disease risk modeling, high-cost patient prediction, and readmission risk scoring.
- Utilization Risk Scoring: Runs dedicated ED utilization risk scoring engines to optimize preventative preventative outreach schedules.
- Mathematical Model Governance: Protects statistical clinical integrity via explainable AI, model drift monitoring, bias monitoring, and human-in-the-loop review.
3. Care Management Workflow Features
Workflow components must translate retrospective analytical insights into real-time task queues for distributed multi-disciplinary medical teams.
- Coordination Infrastructure: Drives care management workflow features, care coordination platform features, and flexible care plan automation features.
- Team Optimization: Maps tasks across multidisciplinary care team features, care team collaboration features, and care manager workload features.
- Workflow Tracking: Automates nurse navigator workflow features, transitional care management features, and chronic care management features.
- Utilization Defenses: Operates post-discharge follow-up automation, readmission prevention features, and targeted ED utilization reduction features.
4. Quality And Regulatory Reporting Features
The reporting engine must automate data collection and parsing across complex federal, state, and commercial quality compliance frameworks.
- Core Quality Analytics: Powers automated quality measure reporting features, CMS quality program features, and clinical quality measure features.
- Compliance Framework Engines: Computes continuous updates for HEDIS measure automation features and STARS rating measure features.
- Programmatic Automation: Drives ACO quality reporting features, regulatory reporting automation VBC, and audit readiness features VBC.
- Verification Tracking: Manages NCQA accreditation features, measure denominator and numerator logic, evidence capture, and reporting deadline tracking.
5. Financial And Contract Management Features
Sustaining profitability under downside contracts requires continuous monitoring of actuarial spend performance directly against payer benchmarks.
- Economic Strategy Dashboards: Unifies value-based contract analytics features with risk-based contract platform features and shared savings program features.
- Federal Program Alignment: Runs native math for ACO REACH model features and Medicare Shared Savings Program features.
- Payment Model Tracking: Computes real-time capitation performance analytics, bundled payment analytics, and total cost of care dashboards.
- Network Optimization: Drives benchmark comparisons, provider performance analytics, network adequacy features VBC, and specialist network management features.
The feature checklist should not become an unanchored technological shopping list.
Each built capability must map directly to a clear alternative contract requirement, an active workflow owner, and a measurable performance KPI.
Features Change With Contract Models
The most important value-based care platform feature requirements change by contract model. MSSP, ACO REACH, Medicare Advantage, capitation, bundled payments, and commercial shared savings do not need the same feature priority.
A serious platform should map each contract type to data sources, required workflows, quality measures, cost controls, and reporting obligations. This clear mapping ensures that technical resources are allocated exactly where contract margins face the highest downside exposure.
1. MSSP And Shared Savings Contracts
Medicare Shared Savings Program models focus heavily on population alignment and meeting strict regulatory quality reporting guidelines.
- Performance Pathway Tracking: Automates patient attribution tracking against live CMS attribution lists to establish stable population panels.
- Mandated Quality Automation: Collects and parses the required APP Plus quality measure set to drive comprehensive ACO quality reporting.
- Financial Benchmark Matching: Runs continuous cost benchmark comparison routines directly against historical CMS fee-for-service data sheets.
- Preventative Gap Closures: Links care gap closure systems directly to preventative care outreach loops to maximize primary care panel performance metrics.
2. ACO REACH And High-Risk Medicare Populations
High-risk innovation models require deeper, non-traditional patient data integration to eliminate deep health disparities and protect global capitation margins.
- Equity Data Integration: Ingests health equity data and social determinants screening features into longitudinal patient graphs.
- Vulnerable Cohort Triage: Executes high-needs patient segmentation algorithms alongside community resource referral tracking pipelines.
- Complex Care Optimization: Fires chronic disease risk scoring models to dynamically drive care team workflow automation tasks.
- Administrative Oversight: Manages specific dually eligible patient workflows while logging system events for rigorous model governance audits.
3. Capitation And Full-Risk Contracts
Under total financial risk, platforms must pivot entirely toward aggressive utilization management, network containment, and precise actuarial cost tracking.
- Fixed Margin Monitoring: Tracks live PMPM cost tracking metrics directly against fixed monthly payer capitation allotments.
- Utilization Defenses: Deploys machine-learning utilization forecasting models to pinpoint upcoming costly institutional events.
- Network Integrity Tools: Runs network leakage analysis features to guide automated in-network referral steering features at the point of care.
- Provider Optimization: Generates provider scorecards and maps ED and admission risk models to big financial risk modeling dashboards.
4. Bundled Payments And Episode-Based Contracts
Episode-based models require longitudinal tracking across strict time windows, cross-facility settings, and discrete specialist clinical boundaries.
- Temporal Stream Tracking: Measures acute and post-acute expenditures using specialized episode of care tracking features across 30 to 90-day windows.
- Discharge Optimization: Runs post-acute cost analytics alongside automated discharge pathway tracking systems to monitor post-facility settings.
- Deficit Control Protocols: Triggers readmission prevention systems while highlighting wide specialist cost variations across standard diagnostic groupings.
- Outcome Verification: Deploys bundled payment management features integrated with procedure-specific outcome tracking questionnaires.
5. Medicare Advantage And Risk Adjustment
Medicare Advantage optimization requires clean documentation, accurate retrospective coding capture, and exceptional consumer preventative engagement scores.
- Benchmark Calibration Tools: Powers HCC coding accuracy features and risk adjustment coding features to accurately compute baseline spending benchmarks.
- Gap Closure Infrastructure: Drives hierarchical condition category capture and coding gap closure features directly within provider charting workflows.
- Performance Rating Safeguards: Monitors documentation completeness and pharmacy adherence to protect highly sensitive STARS rating measure features.
- Preventative Scaling: Controls member engagement workflows to continuously drive proactive wellness scheduling.
There is no single, generic value-based care technology package. At the same time, platform success depends on selecting and prioritizing features based on the exact financial rules and clinical metrics of your specific payer risk contracts.
What Features Support Value-Based Care Transition From Fee-For-Service?
Features needed for VBC model transition should help enterprises move from retrospective billing to proactive population management.
At the same time, the most important transition features are patient attribution, contract modeling, risk stratification, care gap closure, care management workflows, quality reporting, utilization analytics, referral management, and financial performance dashboards.
By implementing these capabilities systematically, healthcare organizations can safely migrate their technology infrastructure away from transactional fee-for-service mechanics and toward outcomes-based financial models.
Stage 1 — Readiness Assessment And Data Inventory
The transition begins with a comprehensive structural audit designed to evaluate current data completeness, map integration dependencies, and inventory active risk contracts.
- Asset Categorization: Reviews current-state EHR instances, claims systems, payer portals, and historical clinical quality measure databases.
- Gap Extraction: Conducts an objective workflow gap assessment while calculating internal data completeness scoring metrics.
- Population Profiling: Segments current patient populations against initial contract definitions to establish clean baseline attribution parameters.
- Intellivon’s Production Approach: We focus on assessing where the enterprise is losing operational visibility first. By diagnosing friction points across attribution, data quality, risk scoring, care coordination, quality reporting, or contract analytics, we establish an engineering roadmap tailored to immediate baseline protection.
- Operational Path Forward: Once the technical dependencies and data gaps are fully cataloged, teams can deploy the core ingestion infrastructure.
Stage 2 — Build The Minimum Viable VBC Data Layer
The platform must establish a foundational, highly secure clinical and administrative data repo to support basic patient timelines and contract calculations.
- Unified Stream Normalization: Pulls multi-source data including real-time EHR feeds, historical claims files, and direct patient attribution files.
- Operational Roster Mapping: Syncs dynamic quality measure data directly with active provider roster data and patient assignment lists.
- Security Architecture Implementation: Provisions robust HIPAA compliant value-based care platform features using data encryption and strict role-based access.
- Intellivon’s Production Approach: We advise clients against trying to build every complex analytical feature at once. The initial engineering release must simply prove that normalized multi-source data can support accurate patient-level decisions and contract-level reporting without breaking audit trails.
- Operational Path Forward: With a stable, compliance-ready minimum viable data layer established, the platform can safely initiate active clinical care workflows.
Stage 3 — Activate Risk And Care Gap Workflows
This stage focuses on deploying predictive machine learning models that surface clinical care gaps and automate task routing for distributed nursing teams.
- Algorithmic Stratification: Triggers automated risk stratification model features alongside rising-risk identification engines to profile panels.
- Queue Automation: Converts open care gaps into active, prioritized care gap work queues and coordinated patient outreach tasks.
- Resource Balancing: Balances live care manager workload features with chronic care management pathways and post-discharge follow-up automation.
- Intellivon’s Production Approach: We focus technical interventions on the highest-value, highest-risk clinical cohorts first. By prioritizing care plan automation features for heart failure, diabetes, COPD, CKD, and frequent ED utilizers, we maximize early utilization reductions.
- Operational Path Forward: As clinical workflows scale to reduce unnecessary utilization, the finance team must track those interventions inside contract analytics models.
Stage 4 — Add Financial Risk And Contract Analytics
The analytics layer translates clinical activity directly into actuarial contract forecasting to give executives real-time clarity regarding shared savings performance.
- Actuarial Baseline Modeling: Drives continuous shared savings forecasting and automated benchmark comparison routines across multi-payer contracts.
- Performance Diagnostics: Evaluates live capitation performance, tracks total cost of care analytics features, and runs network leakage analysis features.
- Variance Auditing: Surfaces deep provider variation metrics right alongside interactive, contract-specific value-based contract analytics dashboards.
- Intellivon’s Production Approach: We carefully decouple clinical action interfaces from executive financial dashboards. Care teams require straightforward patient action lists at the point of care, whereas financial executives need contract performance exposure analytics to manage downside actuarial risk.
- Operational Path Forward: Securing financial transparency across contracts enables the enterprise to scale its infrastructure into highly automated multi-payer operations.
Stage 5 — Scale AI, Governance, And Multi-Payer Operations
The final phase scales the architecture to support complex multi-payer arrangements while enforcing rigid model governance and algorithmic auditing standards.
- Multi-Payer Orchestration: Implements highly scalable multi-payer VBC contract features that adjust dynamically to varying payer rules.
- Algorithmic Supervision: Operates automated model monitoring pipelines that issue instant model drift alerts and check for population bias.
- Accreditation Frameworks: Integrates dedicated NCQA accreditation features and audit readiness features VBC teams can present to regulators.
- Intellivon’s Production Approach: We implement AI strictly as a controlled, deterministic decision-support layer rather than a black-box system. Our architectures ensure that machine learning models prioritize open care gaps and flag risk profiles, while absolute clinical accountability remains with care teams.
The value-based care transition must occur in structured, sequential phases because each progressive analytical layer depends entirely on the data integrity of the previous stage. Adhering to this phased technical roadmap allows enterprise leaders to accurately scope engineering costs and maximize alternative payment revenue.
For a deeper technical breakdown of how to build and maintain the compliance-ready pipelines that support this multi-stage health transition, you can watch this step-by-step engineering video manual.
This resource is highly relevant because it details the architectural layers, data logging requirements, and automated reporting systems needed to scale secure infrastructure across enterprise healthcare environments.
How Much Does A Value-Based Care Platform Cost To Build?
A custom enterprise value-based care platform typically costs $50,000 to $250,000 to build as an initial production-ready deployment or highly targeted Minimum Viable Product (MVP). The final cost within this range is driven entirely by the number of active payer contracts, the complexity of data integration, and the level of automated risk intelligence required.
While basic care tracking solutions occupy the lower end of the spectrum, deploying real-time multi-payer orchestration layers with secure MLOps pipelines will push the project budget toward the upper limit.
1. Cost Breakdown By Development Phase
To keep engineering costs transparent and predictable, development is partitioned into distinct phases that align directly with architectural milestones.
| Development Phase | Estimated Cost Range |
| Discovery, contract mapping, and workflow assessment | $5,000 – $15,000 |
| UX/UI for dashboards, care queues, and admin workflows | $5,000 – $20,000 |
| Data ingestion and interoperability layer | $12,000 – $45,000 |
| EMPI, patient attribution, and roster reconciliation | $8,000 – $25,000 |
| Risk scoring and AI model development | $10,000 – $45,000 |
| Care gap automation and care management workflows | $8,000 – $35,000 |
| Quality measure reporting and evidence capture | $6,000 – $25,000 |
| Contract analytics and financial risk modeling | $8,000 – $40,000 |
| HIPAA security, audit trails, RBAC, and governance | $5,000 – $25,000 |
| Testing, validation, UAT, and deployment | $5,000 – $20,000 |
| Total Estimated Build Cost | $50,000 – $250,000 |
2. Ongoing Maintenance
Annual infrastructure maintenance and operational support usually cost 18% to 28% of the initial software build cost.
This continuous operational expenditure covers critical payer rule updates, evolving federal quality measure changes, active model monitoring, provider integration support, routine security patching, workflow performance tuning, and automated reporting updates.
The cost of building a value-based care platform increases when the environment must support multiple commercial payers, downside risk models, and real-time data exchange.
However, executing a phased development plan ensures that your engineering investment remains tightly tied to measurable contract performance.
Compliance And AI Governance Requirements For VBC Platforms
HIPAA-compliant value-based care platform features must secure PHI, document access, govern AI models, and preserve evidence for payer, CMS, and internal audits. The platform needs encryption, role-based access, audit logs, BAAs, consent controls, explainable AI, model drift monitoring, bias review, and clear separation between recommendations and clinical decisions.
By weaving these protective controls directly into your microservices architecture, you shield your organization from legal liability and catastrophic financial penalties under risk-bearing payment models.
1. HIPAA And PHI Security Requirements
The security framework must enforce absolute data protection across all cloud database instances to maintain federal compliance.
- Data Protection Infrastructure: Mandates end-to-end encryption at rest and encryption in transit across all internal platform nodes.
- Access Barriers: Deploys strict role-based access VBC platform profiles paired with mandatory MFA and automated session controls.
- Traceability Mapping: Generates unalterable audit trail VBC platform logs while enforcing precise, automated PHI minimization protocols.
- Vendor Requirements: Secures all underlying clinical operations through rigorous automated vendor BAA requirements and validated secure backups.
2. AI Transparency And Explainability
Machine learning engines must offer clear, clinical evidence to gain physician trust and prevent blind, black-box decision-making.
- Contextual Insight: Outlines exactly why the patient was flagged and which specific variables influenced risk calculations.
- Confidence Levels: Displays explicit model confidence metrics right alongside interactive clinical point-of-care dashboards.
- Human Oversight: Integrates simple human override switches to ensure final clinical review remains with authorized care teams.
- Feedback Ingestion: Connects a live care team feedback loop to capture real-time clinician observations directly within the system.
MLOps And Model Monitoring
Automated mathematical monitoring pipelines must continuously audit active predictive models to prevent statistical decay.
- Inventory Control: Maintains a central model inventory that maps every active predictive asset running inside the cloud.
- Drift Analytics: Fires continuous drift monitoring and performance monitoring routines to track baseline statistical deviations.
- Equity Auditing: Conducts algorithmic bias analysis alongside automated retraining workflows to safeguard clinical validity.
- System Integrity: Enforces absolute version control and change approval steps inside a centralized feature store governance framework.
Reporting And Audit Readiness
The reporting engine must generate immutable logs to easily satisfy unexpected regulatory and commercial contract compliance reviews.
- Evidence Extraction: Produces exportable evidence trails that document clear measure logic documentation for external auditors.
- Action Tracking: Archives detailed care action logs alongside continuous, historical risk score history and contract calculation history.
- Access History: Records granular user access records to verify compliance with national privacy frameworks.
- Payer Packages: Assembles compiled, payer-ready reporting packages that stream performance metrics to alternative payment administrators.
Compliance must be an active part of the platform’s core architecture. At the same time, a secure platform must continuously prove exactly what it did, why it did it, who reviewed it, and what financial outcome followed.
Integrations Required For Enterprise Value-Based Care Platforms
Enterprise value-based care platform features depend on integrations with EHRs, claims systems, payer APIs, labs, pharmacy systems, HIEs, RPM devices, telehealth tools, scheduling systems, CRMs, care management tools, and analytics warehouses. Integration depth determines whether the platform becomes a live operating layer or another static reporting system.
By building clean, vendor-neutral integration points rather than fragile point-to-point connections, you shield your infrastructure from crashing every time an external vendor pushes a software update.
1. Clinical System Integrations
The clinical data tier must continuously hook into highly fragmented electronic health records to pull real-time patient metrics into the platform.
- Major Vendor Adapters: Connects directly to enterprise endpoints including Epic, Oracle Health, Meditech, Athenahealth, and eClinicalWorks.
- Standardized Interoperability: Implements high-throughput FHIR R4 APIs to map clinical data models consistently across disparate database systems.
- Event Pipeline Routing: Parses legacy HL7 v2 message types to capture real-time ADT events and structured CDA documents.
2. Claims And Payer Integrations
Financial risk reconciliation requires building robust data links with insurers to track actual utilization costs alongside baseline eligibility records.
- Transaction Standards: Processes standard X12 EDI transactions covering 837 claims submission formats and 835 remittance advices.
- Administrative Verification: Manages continuous coverage tracking using 270/271 eligibility inquiries and automated 278 prior authorization exchanges.
- Roster Synchronization: Streamlines operations by matching live payer rosters, active contract files, and central provider directories using modern web-service payer APIs.
3. Patient And Community Data Integrations
To manage rising-risk groups outside hospital walls, platforms must systematically ingest non-traditional clinical and social determinants vectors.
- Socioeconomic Screening: Connects SDOH screening tools with localized community resource platforms to automate non-clinical assistance tracking.
- Continuous Vitals Tracking: Feeds real-time biometric streams from remote patient monitoring (RPM) devices and telehealth platforms into central graphs.
- Outreach Optimization: Links pharmacy data, lab data, and patient engagement tools directly to automated SMS and email outreach pipelines.
For a deeper breakdown of clinical data exchange economics, see our guide on Cost To Develop a Healthcare Data Interoperability Platform.
Integrations completely decide whether your value-based care platform succeeds or fails visually. If data arrives late, incomplete, or without clear workflow context, distributed care teams simply cannot intervene in time to protect performance margins.
How Intellivon Builds Value-Based Care Platforms
Intellivon builds value-based care platforms as enterprise AI infrastructure that connects data, risk models, workflows, contract analytics, and compliance controls. The build process starts with contract and workflow discovery, then moves through architecture, integration, AI modeling, care workflow automation, security validation, and phased rollout.
By treating healthcare software as highly integrated, deterministic infrastructure rather than disconnected reporting dashboards, we build environments engineered to actively protect downside contract margins.
Step 1 — Map Contracts Before Features
Engineering must align directly with active payment rules to prevent wasting capital on unnecessary or unaligned software components.
- Alternative Payment Alignment: Analyzes specific operational boundaries across MSSP, ACO REACH, capitation, bundled payments, and Medicare Advantage programs.
- Financial Boundary Analysis: Maps precise commercial shared savings thresholds alongside targeted clinical quality measures to isolate downside risk exposure.
- Intellivon’s Production Approach: We scope the first build around the contracts that create the most financial exposure. This keeps feature prioritization tied to immediate ROI, ensuring that initial capital outlays directly defend the most vulnerable revenue lines.
- Operational Path Forward: Once the specific contractual math is structurally codified, we proceed to engineer the primary data lake infrastructure.
Step 2 — Build The Unified Data Foundation
The core storage tier must serve as an immutable, consolidated source of truth by ingesting highly fragmented clinical and administrative data streams.
- Holistic Ingestion: Normalizes high-volume live EHR feeds alongside historical claims ingestion and variable-quality measure data streams.
- Identity Mapping: Deploys advanced identity resolution mechanics to manage member records, contract attribution rules, and financial data assets.
- Governance Controls: Implements rigid, multi-tenant PHI controls to satisfy federal privacy frameworks during high-throughput parallel data processing.
- Intellivon’s Production Approach: We design reusable ingestion pipelines so future payer contracts do not require rebuilding the platform foundation. This decoupling ensures that adding a new commercial payer or moving to global capitation requires only simple data mapping configuration changes.
- Operational Path Forward: Establishing a validated, highly scalable data layer enables the deployment of specialized predictive machine learning models.
Step 3 — Develop AI Risk And Care Gap Models
Analytical microservices must process clean clinical graphs to accurately forecast utilization trends and capture documentation blind spots.
- Utilization Analytics: Deploys specialized predictive risk scoring models targeting readmission risk and ED utilization risk parameters.
- Clinical Profiling: Computes long-term chronic disease risk while running automated checks to support HCC coding gap support.
- Pipeline Integrity: Operates end-to-end model governance using strict MLOps tracking pipelines to prevent algorithmic performance decay over time.
- Intellivon’s Production Approach: We keep AI recommendations explainable and reviewable, especially where models influence care prioritization. Every risk flag surfaces its precise underlying clinical features so physicians can confidently act on the model’s findings.
- Operational Path Forward: Predictive insights must be wired directly to automated execution queues to transform analytical scores into active clinical interventions.
Step 4 — Automate Care Team Workflows
The workflow layer converts retrospective risk percentages into automated, real-time action lists for distributed medical staff.
- Clinical Orchestration: Generates automated care plans and coordinates automated patient outreach sequences based on open performance targets.
- Task Assignment Routing: Populates unified care manager queues to automate nurse navigator routing and assign specific community health worker tasks.
- Preventative Proactive Loops: Triggers structured, algorithmic post-discharge workflows right alongside multi-channel preventive care reminders.
- Intellivon’s Production Approach: We build workflows around how care teams already work, then remove repetitive tracking and manual prioritization. By embedding automated care tasks directly inside active clinical systems, we maximize care manager productivity without adding software fatigue.
- Operational Path Forward: As care managers execute targeted interventions, the resulting operational data must feed directly into executive performance views.
Step 5 — Add Contract, Quality, And ROI Dashboards
The analytics engine must compute real-time operational and financial variance metrics to give leadership complete visibility across active risk lines.
- Actuarial Performance Views: Models continuous shared savings projections and generates benchmark comparison charts across active payer groups.
- Quality Metrics Monitoring: Tracks live aggregated quality scores to defend highly sensitive STARS and HEDIS contract performance metrics.
- Network Diagnostics: Powers granular provider scorecards to trace macro utilization trends and identify localized network leakage anomalies.
- Intellivon’s Production Approach: We separate executive, finance, clinical, and care manager views so each team sees the decisions they own. Finance teams monitor contract exposure thresholds, while clinical directors track care gap velocities inside independent, secure access zones.
- Operational Path Forward: Final analytics modules are wrapped in automated verification checks to prepare the entire application infrastructure for production release.
Step 6 — Validate Compliance And Scale
Before launching, the platform must undergo rigorous stress testing and configuration auditing to ensure absolute system resilience and compliance.
- Security Auditing Validation: Enforces strict HIPAA controls, verifies immutable audit logs, and deploys continuous automated model monitoring tools.
- Deployment Operations: Coordinates deep security testing, User Acceptance Testing (UAT), and multi-stage phased deployment strategies.
- Continuous Maintenance: Executes systemic post-launch optimization workflows to smoothly incorporate changing clinical profiles and updated payer rules.
- Intellivon’s Production Approach: We treat launch as the start of optimization. Value-based care platforms need tuning as contracts, quality measures, and populations change, which is why we build our environments to adapt dynamically without requiring custom rewrites.
For a deeper breakdown of patient risk infrastructure, see our guide on Development Cost For An Enterprise Population Health Platform.
The strongest value-based care platforms do not start as decorative, passive analytics dashboards. They start as contract-aware enterprise operating systems designed to align population health, distributed care coordination, and financial downside risk.
Build Value-Based Care Platforms With Intellivon
Intellivon helps healthcare organizations build value-based care platforms that connect clinical data, claims data, care workflows, AI risk models, quality reporting, and contract analytics into production-ready infrastructure.
The goal is not to add another dashboard. It is to help care, finance, and operations teams manage value-based performance from one trusted system.
What Intellivon Helps Build
- Multi-source healthcare data ingestion
- EHR, claims, pharmacy, lab, SDOH, RPM, and payer integrations
- Patient attribution and roster reconciliation
- Predictive risk scoring and rising-risk identification
- Care gap automation and outreach workflows
- Chronic care and transitional care management workflows
- HEDIS, STARS, CMS, and ACO quality reporting
- HCC coding and risk adjustment support
- Contract analytics and shared savings dashboards
- HIPAA security, audit logs, RBAC, and AI governance
Why Teams Work With Intellivon
- 500K+ engineering hours
- Ex-MAANG engineering experience
- Complex healthcare integration expertise
- HIPAA-ready architecture
- AI, MLOps, LLM, and agentic workflow experience
- Production-first healthcare AI delivery
If your team is planning a value-based care platform build, Intellivon can help you define feature scope, integration requirements, AI model architecture, compliance controls, cost range, and rollout roadmap before development begins.
Conclusion
Value-based care platform features matter because risk-based care demands one trusted operating layer for attribution, risk scoring, care gaps, workflows, quality reporting, contract analytics, compliance, and AI governance.
These platforms help teams identify patients needing action, contracts carrying exposure, measures at risk, and interventions that improve outcomes and financial performance. As shared savings, capitation, ACO REACH, and bundled payments grow, this infrastructure becomes central to accountable care delivery and strategy.
Things To Know About Value-Based Care Platform Features
Q1. How much does a value-based care platform cost to build?
A1. A custom value-based care platform usually costs $180,000–$650,000+ to build, depending on data sources, contract complexity, AI depth, and reporting requirements.
A focused MVP with data ingestion, attribution, basic risk scoring, care gaps, and dashboards can start near $120,000. However, multi-payer platforms with AI models, contract analytics, quality automation, and HIPAA governance can exceed $900,000 when enterprise-scale workflows are required.
Q2. How long does value-based care platform development take?
A3. A focused MVP usually takes 14–20 weeks when the first release covers one population, one or two contracts, and limited workflows. However, a production platform with EHR integration, claims ingestion, AI models, quality reporting, and contract analytics usually takes 6–10 months.
For larger organizations, multi-payer enterprise rollouts can take 10–18 months because testing, data validation, compliance review, and workflow adoption take longer.
Q3. What features support value-based care transition fastest?
A3. The fastest transition features are patient attribution, risk stratification, care gap identification, post-discharge follow-up automation, quality measure reporting, and total cost of care analytics. These features help enterprises move from retrospective reporting to proactive care management.
As a result, teams can identify high-risk patients earlier, prioritize outreach, track contract exposure, and connect daily care actions to measurable financial and quality outcomes.
Q4. What AI features for value-based care models matter most?
A4. The most useful AI features are predictive risk scoring, rising-risk identification, readmission prediction, ED utilization prediction, HCC coding gap detection, outreach prioritization, and explainable care recommendations.
However, these models should not operate as black boxes. Each model should show why a patient was flagged, which data influenced the score, and what action the care team should review next. Therefore, human oversight must remain part of the workflow.
Q5. What integrations are required for a HIPAA-compliant value-based care platform?
A5. A production platform should integrate with EHRs, claims systems, payer APIs, pharmacy feeds, lab systems, ADT feeds, SDOH tools, RPM devices, telehealth platforms, and patient outreach tools. In addition, it needs encryption, RBAC, audit logs, BAA support, PHI access controls, and secure data transmission.
Without these controls, the platform may improve visibility but still create compliance, privacy, and governance risk.
Key Takeaways
- A value-based care platform is not a dashboard. It is the operating layer that connects patient risk, care action, quality evidence, and contract economics.
- The feature priority should change by payment model. MSSP, ACO REACH, capitation, bundled payments, and Medicare Advantage do not need the same build roadmap.
- The highest ROI usually comes from attribution accuracy, readmission prevention, care gap closure, HCC documentation support, and total cost of care visibility.
- AI only creates value when predictions trigger care workflows, model explanations, human review, and measurable outcome tracking.
- Custom development makes sense when the enterprise needs control over data, contract logic, patient segmentation, workflow design, and financial risk modeling.



